Clinical History
The patient is a 72 year old female who overall has been fairly healthy. She has struggled with a cough for several years. A CT scan in 2015 showed some tree-in-bud changes in the lungs potentially consistent with an atypical mycobacterial infection. She had a positive methacholine challenge test and was diagnosed with asthma. Her cough has not improved with inhaled asthma treatments. The cough has been persistent and is at times productive of small amounts of whitish sputum. She has not noted any progressive shortness of breath. Over the last several months she has tried trials of both nasal corticosteroids, and treatment with Prilosec for gastroesophageal reflux. Both of these trials had no effect on her cough. At the end of November 2018, a CT scan of the chest was consistent with an atypical mycobacterial infection.
In January 2019, she came back from a skiing trip. She tried to ski but was unable to because of shortness of breath; she came home on the third day prematurely. During this time, she developed increased cough, fevers and chills. An x-ray was obtained by her primary care provider, which showed a right lower lobe infiltrate, and was placed on levofloxacin for 5 days. After completing the antibiotic, she is still very fatigued and still coughing. She presented to her pulmonologist in March 2019. She denied any fevers, chills or chest pain. Her cough has continued with intermittent sputum production. Her appetite and weight have been stable, along with bladder and bowel habits.
The patient’s past medical history is significant for arthritis, cataracts, depression, polymyalgia rheumatica, and sciatic nerve pain. Her past surgical history is only a tonseillectomy in her childhood. Her social and family history is that she runs an educational travel business, is currently divorced, has never been a smoker, and has no family history significant for recurrent infections.
Laboratory Findings
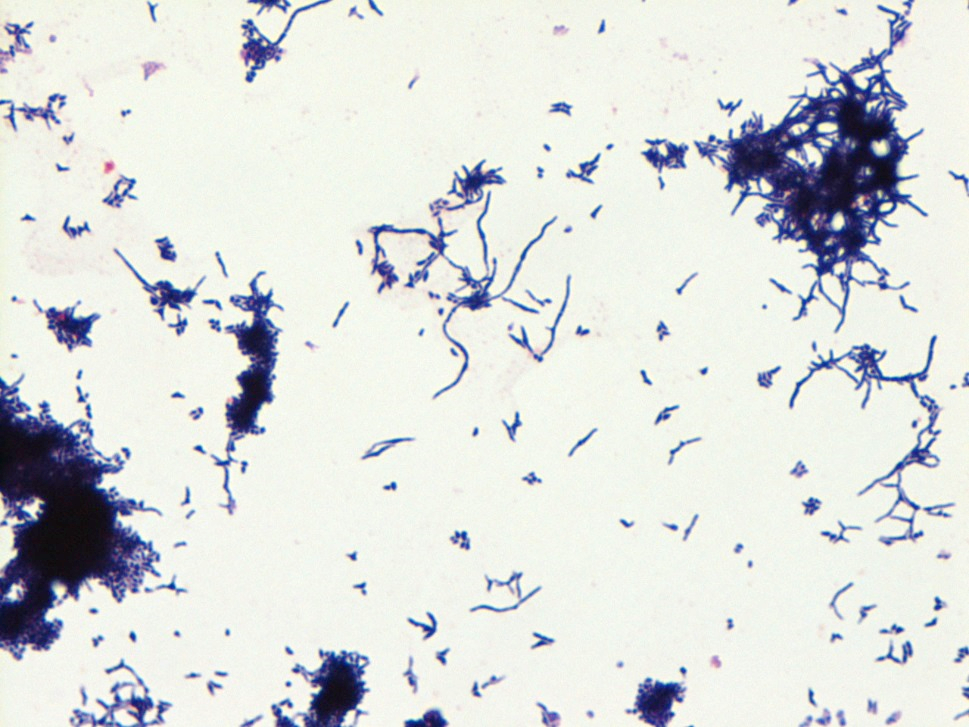
Induced sputum samples were obtained and inoculated on a 7H9 bottle that was incubated and continuously monitored for growth. Eight days later, the 7H9 bottle flagged positive for growth. A gram stain showed branching gram positive bacilli. The Kinyoun acid-fast stain was negative, but a modified Kinyoun showed rare positive staining cells. The bottle was subcultured onto chocolate agar, 7H11 agar, buffered charcoal yeast extract (BCYE) agar, and LJ slants. Two days later, all plates except the 7H11 plate showed growth of white, dry, crinkled colonies as depicted in Image 1. A gram stain of the colonies showed branching gram positive bacilli as shown in Image 2. Again, the Kinyoun stain of the colonies was negative but the modified Kinyoun again highlighted cells as seen in Image 3. A representative colony was sent for identification to Mayo laboratories a day later. MALDI-TOF performed by Mayo Laboratories revealed the bacteria to be Rothia aeria. An attempt was made to set up sensitivities but the organism was not able to grow out on the test medium.


Discussion
Rothia aeria is a very rare pathogen with a current PubMed search yielding 20 references. It was first isolated from the MIR space station (1) and genomic sequencing was perform on the bacteria (2). It has been shown to be a normal oral flora (3), but also seems to be most associated with endocarditis. A few case reports have discussed sepsis, respiratory infections, and joint infections. Importantly, it has been documented to be confused with Nocardia species (4).
References
- Li, Y. et al. Rothia aeria sp. nov., Rhodococcus baikonurensis sp. nov., and Arthrobacter russicus sp. nov., isolated from air in the Russian space laboratory Mir. Int J Syst Evol Microbiol. 2004; 54(pt. 3): 827-835.
- Nambu, T. et al. Complete Genome Sequence of Rothia aeria Type strain JCM 11412, Isolated from Air in the Russian Space Laboratory Mir. Genome Announc. 2016 Dec 29; 4(6).
- von Graevenitz, A. et al. Coryneform bacteria in throat cultures of healthy individuals. J Clin Microbiol. 1998; 36: 2087-2088.
- Saraya, T. et al. Rothia aeria: a great mimicker of the Nocardia species. BMJ Case Rep. Published Online: November 18, 2014.
-Jeff Covington, MD, PhD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
