A male teenager presented to the emergency department following a 4 wheeler accident. He sustained extensive trauma to his right lower leg with a large, dirty laceration and grossly exposed muscle. His pulses were intact and motor & sensory nerve function were preserved. The wound was irrigated at the bedside and the patient was admitted with a plastic surgery consult for wound coverage. Cefepime was empirically started. After 10 days in the hospital and multiple surgeries to care for the wound, the patient developed a fever and increased pain, erythema, and swelling at surrounding the wound. The trauma service ordered blood and wound cultures.
Laboratory Identification
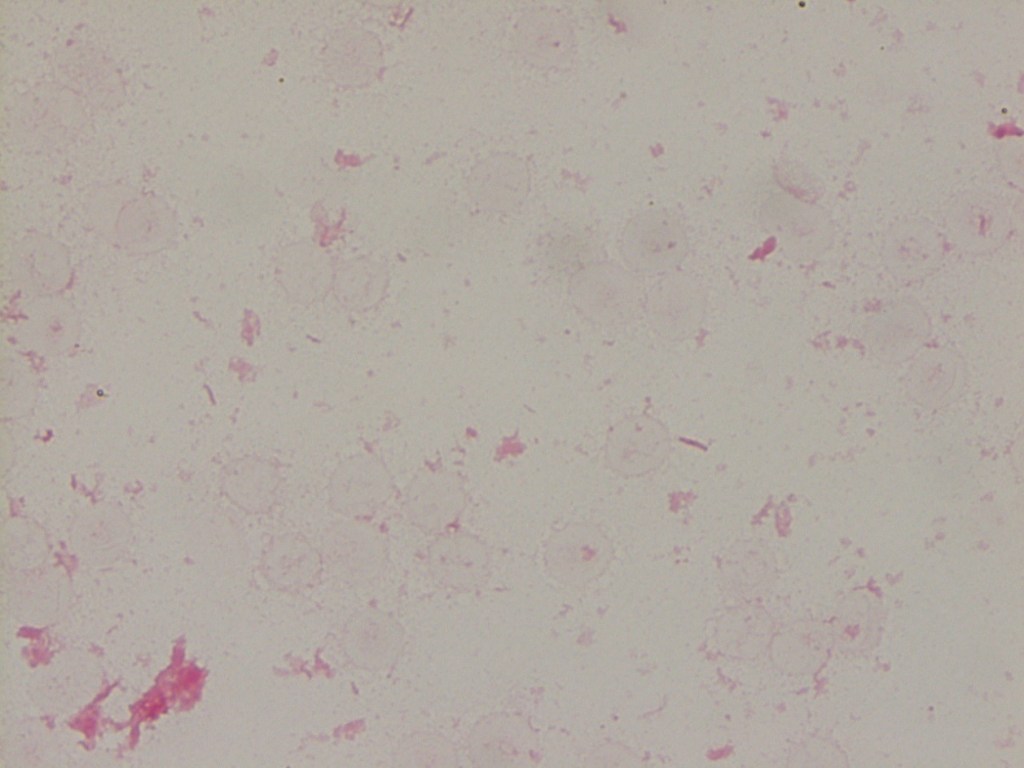
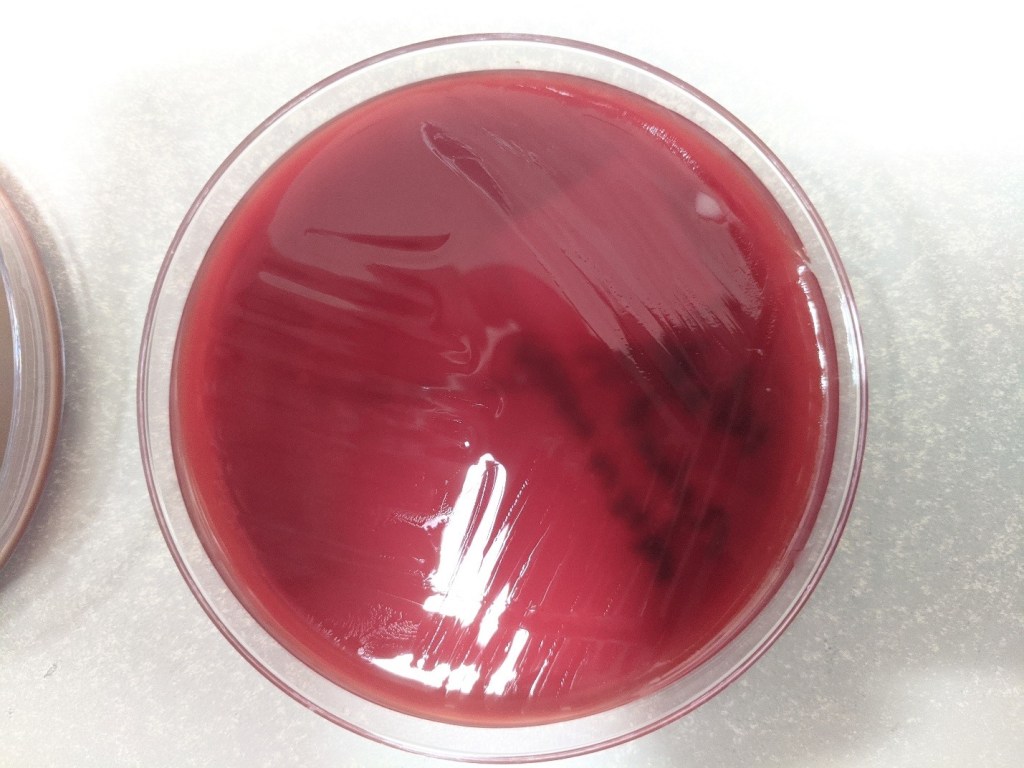
Image 1. The wound culture grew lavender-green colonies on blood agar (48 hours of incubation in CO2). Image 2. Clear, lactose-negative colonies on MacConkey agar (48 hours of incubation in CO2). Image 3. Gram stain from the blood agar plate showed gram negative rods (100x, oil immersion).
The oxidase reaction was negative. MALDI-TOF mass spectrometry identified the isolate as Stenotrophomonas maltophilia from the wound culture. Blood cultures were negative.
Discussion
Stenotrophomonas maltophilia is a common non-fermenting gram negative rod that is ubiquitous in moist environments but is not commonly a member of human flora. S. maltophilia can readily be isolated from hospital surfaces and those with traumatic injuries, prolonged hospitalizations, on mechanical ventilation, and with in-dwelling devices are more susceptible to nosocomial infections by this organism. Those who are immunocompromised or have cystic fibrosis are also at an increased risk.
In the laboratory, S. maltophilia is characterized as an aerobic, Gram-negative rod that grows as lavender-green colonies on blood agar (Image 1) and has an ammonia-like odor. This organism is catalase and oxidase negative and DNase positive. S. maltophilia is motile and is able to utilize glucose and maltose by oxidative fermentation. Current automated identification systems and MALDI-TOF mass spectrometry are able to accurately identify S. maltophilia.
S. maltophilia is intrinsically resistant to many broad-spectrum antibiotics, including carbapenems and aminoglycosides. Beta-lactam resistance is due to two beta-lactamases and renders beta-lactam inhibitors ineffective. Trimethoprim-sulfamethoxazole (TMP-SMX) is the antibiotic of choice to treat S. maltophilia infections; however, resistance can develop. In the case TMP-SMX resistance, ceftazidime, minocycline, ticarcillin-clavulanate, ciprofloxacin, and levofloxacin can be tested.
In the case of our patient, susceptibility testing was performed on the Vitek2 instrument and the isolate was susceptible to TMP-SMX. He was switched to TMP-SMX and underwent additional surgical procedures to wash out the infected area.
-Karla Perrizo, MD, is a Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD is the System Director of Clinical Pathology at University Hospitals Cleveland Medical Center in Cleveland, Ohio. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Her interests include infectious disease histology, process and quality improvement, and resident education.
A 50 year old male patient receiving chemotherapy for treatment of gastric cancer presented to ER. Labs reported:
WBC = 5.4 x 103/μL
Hgb = 8.9 g/dL
PLT (impedance) = 26 x 103/μL
PLT-F (fluorescent) = 9 x 103/μL
IPF = 21%
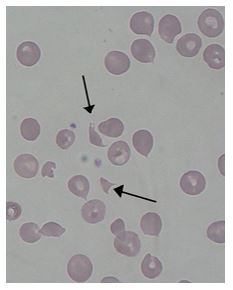
The hemoglobin was consistent with the patient history. Flags on the original impedance platelet count included thrombocytopenia, platelet clumps and platelet abnormal distribution. The sample was checked for clots, with no clots found. A fluorescent platelet count (PLT-F) was reflexed and the critical platelet count was called to the ER physician. The high immature platelet fraction (IPF%) indicates increased platelet production. Despite the increased production, the patient still had a severe thrombocytopenia. This would suggest thrombocytopenia caused by platelet destruction or consumption. Examination of the blood smear showed the presence of moderate numbers of schistocytes.
Image 1. Schistocytes seen on peripheral blood smear
Additional labs were ordered. BUN and Creatinine were slightly elevated. PTINR and APTT were within normal range. LDH was markedly increased. The physician was able to use this information, along with the clinical presentation and history, to diagnose Thrombotic Thrombocytopenic Purpura (TTP). Plasma exchanges were initiated. The patient expired 3 days later.
The difference between the impedance platelet count and the fluorescent platelet count in this patient is actually related to the presence of schistocytes. With thrombocytopenia, platelet counts can be less reliable than with normal counts. Automated platelet counts were originally performed by impedance methods, then better accuracy and precision was obtained with optical platelet counts. Physicians rely on precision with very low platelet counts to make informed decisions about treatment. The problem with the impedance counts at the low end is that RBC fragments, schistocytes and microcytic RBCs can be counted as platelets, giving a falsely high count, as we see in this case. On the other hand, measuring platelets by size (optical) can miss large platelets leading to a falsely low count. The PLT-F is more reliable because it uses a platelet specific dye which eliminates these interferences. The fluorescent dye labels the RNA. Forward scatter is used to determine size while fluorescence is used to measure RNA content. With gating set based on cell volume and RNA content, the PLT-F can be measured. When there is an abnormal scattergram or a low platelet count, the PLT-F is reflexed and the IPF% is also reported.
The Immature platelet fraction (IPF) can also be used to help understand the etiology and aid in diagnosis. Historically, the MPV has been used as an indirect marker for platelet production. However, an inherent problem with the MPV is that, similarly to the impedance platelet count, this count can be unreliable because any RBC fragments or particles may interfere with the measurement. Reticulated or immature platelets are the youngest platelets, within 24 hours of being released from the bone marrow. Measurement of these is a concept that first emerged in the late 1960s, before automated hematology analyzers performed platelet counts. Thus, the original method was staining with new methylene blue and manually counting, much like a manual reticulocyte count. These manual methods tend to be tedious and imprecise. In the last 20 yeas we have developed flow cytometry methods for performing a reticulated platelet count. Reticulocytes are stained with Thiazole Orange and passed through a flow cytometer. Unfortunately, there is no standardization for the procedure as there are variations in dye concertation, timing and gate settings. As well, this method is also time consuming, labor intensive, costly, and requires highly trained technologists to perform.
Newer flow cytometry methods to count these youngest platelets are available on Sysmex and Abbott CELL-DYN analyzers. The IPF (Sysmex) or RetPLT(Abbott) can be performed along with the routine CBC with no additional sample or time required. Knowing the reticulated or immature platelet fraction can help physicians to differentiate pathogenesis. A decreased percent of newly formed platelets may indicate that thrombocytopenia is caused by deficient platelet production, as seen in bone marrow failure. Increased circulating immature platelets with a low platelet count may suggest that the bone marrow is making adequate platelets and the thrombocytopenia is caused by platelet destruction or consumption. Treatment for these scenarios is different, and the physician must determine the etiology in order to determine treatment
Thrombotic thrombocytopenic purpura (TTP) is a microangiopathic hemolytic anemia with thrombocytopenia and organ failure caused by microvascular thrombosis. Platelets clump in the small blood vessels and cause the low platelet count. The hemolytic anemia causes schistocytes which can be seen on the peripheral blood smear. In this case, the low platelet count and high IPF, schistocytes on the smear and the patient presentation were all important factors that led to a speedy diagnosis and start of therapy.
Plasma exchange is the treatment of choice for TTP. With the advent of therapeutic plasma exchange, mortality from TTP has decreased from about 90% to 10-20%. In patients who have relapses or become refractory, vincristine has been used successfully as an adjunct to plasma exchange.4 The exact etiology of TTP is unknown. It can be secondary TTP, often triggered by chemotherapy drugs, or can be sporadic. Sporadic, or idiopathic, TTP is now thought to be associated with an acquired autoimmune deficiency of a plasma metalloprotease named ADAMTS13. The ADAMTS13 gene controls this enzyme, which is involved in blood clotting. In acquired TTP, the ADAMTS13 gene isn’t faulty. Instead, the body makes antibodies that block the activity of the ADAMTS13 enzyme. In these cases, a lack of activity in the ADAMTS13 leads to TTP. Almost all cases of recurrent TTP have severe ADAMTS13 deficiency. These patients benefit from immunosuppressive therapy with vincristine along with plasma exchange.
However, despite the decreased mortality seen with plasma exchange, patients with cancer, infections, transplant patients, or those receiving certain drug therapy have a much worse prognosis.4 In this case study, this was this patient’s first episode of TTP and he was undergoing chemotherapy for gastric cancer. The patient’s unfortunate outcome is most likely linked to this finding.
References
Arshi Naz et al. Importance of Immature platelet Fraction as a predictor of immune thrombocytopenic purpura. Pak J Med Sci 2016 Vol 32 No 3:575-579
Johannes J. M. L. Hoffmann, Nicole M. A. van den Broek, and Joyce Curvers (2013) Reference Intervals of Reticulated Platelets and Other Platelet Parameters and Their Associations. Archives of Pathology & Laboratory Medicine: November 2013, Vol. 137, No. 11, pp. 1635-1640.
M Meintker, Lisa & Haimerl, Maria & Ringwald, Juergen & Krause, Stefan. (2013). Measurement of immature platelets with Abbott CD-Sapphire and Sysmex XE-5000 in haematology and oncology patients.
J. Evan Sadler, Joel L. Moake, Toshiyuki Miyata, James N. George Clinical chemistry and laboratory medicine : CCLM / FESCC. 51. 1-7. 10.1515/cclm-2013-0252.; Recent Advances in Thrombotic Thrombocytopenic Purpura. Hematology Am Soc Hematol Educ Program 2004; 2004 (1): 407–423. doi: https://doi.org/10.1182/asheducation-2004.1.407
Sysmex White Paper. The role of the Immature Platelet Fraction(IPF) in the differential diagnosis of thrombocytopenia. www.sysmex.com/us
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
A 60 year old patient with a past medical history of type II diabetes mellitus, right Charcot foot, and cirrhosis presented to the emergency department with altered mental status and several days of subjective fevers, as well as a 2 month history of right lateral malleolar non-healing ulcer which had subacutely increased in size and volume of drainage.
The patient’s spouse reported the wound had been showing purulent discharge for 3 weeks. Nine days before presentation, the patient had seen a foot and ankle specialist for evaluation of his Charcot foot and the ulcer. Radiographs were taken at this time, but no treatment was initiated. Worsening of the wound was associated with an episode of long travel, after which the patient reported being able to see bone.
Infectious disease noted that the patient had a pet corgi.
On exam, the patient was febrile with dry mucous membranes and oriented only to person. MRI showed evidence of possible osteomyelitis. The patient subsequently underwent a right below the knee amputation.
Laboratory findings
Gram smear of a sample taken from the patient’s ankle wound in the emergency department showed many neutrophils, moderate gram positive cocci and moderate gram negative bacilli, with intraleukocytic organisms seen. Growth was observed on blood and chocolate agar plates, but there was no growth on the MacConkey plate. The organisms were identified as few Pasteurella multocida, few vancomycin resistant Enterococcus faecalis, and few usual skin flora.
Image 1. Gram stain of the sample taken from the patient’s ankle wound.
Blood cultures drawn in the emergency department were positive at 10 hours in both bottles, and again on planting showed growth on blood and chocolate agar, but no growth on MacConkey. The organism was identified as P. multocida, consistent with that which grew from the ankle wound culture.
The patient underwent a right below the knee amputation, and anaerobic cultures taken from the right foot again grew P. multocida.
Discussion
Pasteurella multocida is a nonmotile gram negative bacillus which is part of the normal oropharyngeal flora in domestic dogs and cats. It is a facultative anaerobe, positive for oxidase, catalase, and indole. It grows on chocolate and blood agar, forming small, gray, non-hemolytic colonies. It does not typically grow on MacConkey agar.
P. multocida is classically associated with a zoonotic soft tissue infection in humans who suffer bite wounds from a pet, as well as licking of any broken skin by a pet. These infections have a characteristic rapid onset and intense inflammatory response, and can progress to necrotizing fasciitis. Cases of Pasteurella osteomyelitis can be associated with significant wound infections. Conditions such as diabetes, liver dysfunction, and organ transplantation can predispose patients to Pasteurella bacteremia.
Pasteurella spp. are susceptible to beta-lactam antibiotics in most cases, and since Pasteurella wound infections are usually polymicrobial, recommended treatment is broad-spectrum such as amoxicillin-clavulanate. In isolated Pasteurella infections, first line treatment is penicillin, although there are some that favor testing isolates from sterile sites for the presence of beta-lactamase production, and treating those infections with ampicillin-sulbactam, pipercillin-tazobactam, or ceftriaxone. (Weber)
-Tom Koster, DO is a 1st year Anatomic and Clinical Pathology Resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
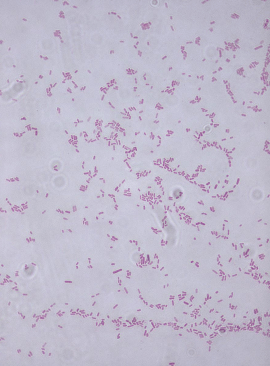
A 42 year old male with past medical history of diabetes mellitus and essential hypertension presented to the emergency department with high fever and chills which developed two days prior. His examination revealed a painful ulcer on the planter aspect of his right toe with surrounding erythema. According to patient, the exact duration of the ulcer is unclear as it was on planter aspect of his foot and he does not inspect his feet regularly. However, the ulcer grew in size and symptoms over the past week. He denies any cough, diarrhea or abdominal pain. He is on oral anti-diabetics with well-controlled blood sugar. Complete blood count revealed leukocytosis. Blood was collected and sent to microbiology laboratory for gram stain and culture.
Laboratory identification
Cultures signaled positive after 32 hours of incubation and gram negative rods were identified on Gram stain (Image 1). The organism grew after 24 hours of incubation on 5% sheep blood, chocolate, and MacConkey agars (Images 2 & 3). MALDI-TOF mass spectrometry identified the isolate as Salmonella spp. The isolate was sent to the public health department for additional testing by molecular typing where it was identified as Salmonella enterica subsp. enterica serovar Brandenburg (Salmonella Brandenburg). Later, MRI revealed osteomyelitis of right third toe which was considered as the likely source of patient’s bacteremia.
Image 1. Gram stain of positive blood culture broth showing gram negative rodsImage 2. Non-lactose fermenting colonies growing on MacConkey agarImage 3. Colonies producing hydrogen sulfide making them appear black on Hektoen enteric agar
Discussion
Salmonella is a genus of the family Enterobacteriaceae in the order Enterobacterales. They are non-spore forming gram negative facultative anaerobes. Salmonella spp. are lactose non-fermenters and usually produce H2S on triple sugar iron and Hektoen enteric agar.
The genus has only two species: Salmonella enterica, divided into 6 subspecies and containing over 2500 serovars, and Salmonella bongori. Subspecies and serotype determination is necessary for epidemiological investigations. Serotyping is used to classify Salmonella based on bacterial surface antigens; the thermostable polysaccharide cell wall or somatic (“O”) antigens and the thermo-labile flagella proteins or “H” antigens. It is also possible to identify Salmonella serotypes on the basis of phage typing, plasmid profiling, ribotyping and pulsed field gel electrophoresis (PFGE) of DNA fragments generated from restriction enzyme digestion.
Salmonella are zoonotic bacteria that can cause abortion, metritis, and systemic illness in ewes and does. Natural reservoirs of Salmonella are domestic and wild animals, including poultry, swine, cattle, birds, dogs, rodents, tortoises, turtles and cats. Humans also serve as a natural host. The most common source of transmission of Salmonella is the consumption of contaminated poultry and meat products. Person-to-person, fecal–oral transmission does occur and has been a problem in health care facilities traced to inadequate hand washing.
Salmonella brandenburg ranked 16th among the serovars responsible for human infections. It causes acute diarrhea and severe illness in a variety of animals and was first isolated in New Zealand in 1986. Since 1996 Salmonella Brandenburg has been associated with an emerging epidemic of abortions and deaths in sheep in the southern regions of the South Island. Subsequently, the same strain was reported to cause disease in horses, goats, deer, pigs and humans. The disease is known to have high morbidity and mortality within a flock or herd, rapid local spread and an occupational, health and safety risk to farm workers and their families.
There are three clinically distinguishable forms of salmonellosis in humans. These include gastroenteritis, enteric fever and septicemia. Established Salmonella bacteremia requires aggressive antimicrobial treatment with ciprofloxacin, ceftriaxone, or less frequently trimethoprim-sulfamethoxazole. A careful search for focal metastatic disease should be undertaken, especially when relapse follows cessation of treatment. Surgical drainage of metastatic abscesses may be required, with surgical intervention. Resistance to any of the drugs used to treat invasive infection may occur, so treatment should be supported by susceptibility testing.
In the case of our patient, he was treated with ceftriaxone and underwent toe amputation. The patient had an uncomplicated hospital course and made a complete recovery.
Alvseike O., Skjerve E. (2000). Probability of detection of Salmonella using different analytical procedures, with emphasis on subspecies diarizonae serovar 61:k:1,5,(7) [S. IIIb 61:k:1,5,(7)]. International Journal of Food Microbiology, 58, 49-58.
Clark G, Swanney S, Nicol C, and and Fenwick S. Salmonella Brandenburg – the 1999 Season. Proceedings of the Sheep and Beef Cattle Society of the New Zealand Veterinary Association, 151-156, 2000
Baumler A.J., Tsolis R.M., Heffron F. (2000). Virulence Mechanisms of Salmonella and their Genetic Basis. In “Salmonella in Domestic Animals” (Ed. C. Wray and A. Wray). CAB International 2000, pp. 57-72
-Ansa Mehreen, MD. 1st year AP/CP resident at University of Chicago hospital program based at Evanston Hospital. Her academic interests include gastrointestinal pathology.
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.
A 55 year old patient with past medical history of stage IV non-Hodgkin’s lymphoma on rituximab and Campylobacter jejuni bacteremia 1 year prior presented to the Emergency Department on the orders of their primary care provider, after outpatient blood cultures grew gram negative bacilli resembling Campylobacter species. Their symptoms included a 1-2 month history of fatigue and weakness and a 3 week history of intermittent fevers and chills with developing productive cough, sinus pressure, sore throat, progressive dyspnea on exertion, nausea, and decreased appetite.
Laboratory Findings
Initial (outpatient) blood culture was positive in the aerobic bottle at 60.1 hours, with the initial gram stain showing no organisms. The bottle was placed back in the analyzer and flagged positive again, at which point a second gram stain was performed, which again showed no organisms. An acridine orange stain was performed (Image 1), revealing multiple spiral/”gull shaped” rods. A third gram stain (Image 2) with more time allowed for safranin staining revealed faint gram negative rods. MALDI-TOF MS was attempted with no identification. The culture growth was sent to a reference laboratory and was identified via sequencing as Helicobacter species. The organism was not viable for susceptibility testing.
Image 1. Acridine orange stain of blood culture sample: this stain causes the nucleic acids to fluoresce orange, highlighting the bacteria against the background of blood.Image 2. Gram stain after allowing extra time for safranin staining, showing few gram negative rods.Image 3. A replating on blood agar showed difficult to discern, thin spreading colonies.
Two sets of subsequent blood cultures also grew gram negative bacilli at 65 and 67 hours. The blood culture broth from one of these cultures was also sent to the reference lab, but again did not have viable growth for susceptibility testing.
Discussion
The genus Helicobacter includes 35 species, consisting of gram negative spiral bacilli, previously considered to be part of the Campylobacter genus. Pathogenic species are classically associated with the gastrointestinal tract as they are able to survive in the harsh acidic conditions of the human stomach. The most common clinically relevant species is H. pylori, which is associated with gastric ulcers as well as other inflammatory processes in the stomach and duodenum. In prior reports, bacteremia caused by Helicobacter species is typically associated with some other underlying disease process, such as malignancy, immunocompromised state, or disruption of the GI mucosal barrier (1, 2, 3, 4, 5, 6).
Helicobacterspp. are similar in morphology to Campylobacterspp. on a gram stain; given the patient’s prior history of C. jejuni bacteremia, it was not unreasonable for the gram smear to initially be called consistent with Campylobacterspp. However, the clinical course and antibiotic susceptibility profiles of Helicobacter and Campylobacter bacteremia cases can differ in important ways. Further, susceptibilities can differ between different species of Helicobacter. There are no established guidelines for the treatment of Helicobacter spp. bacteremia and breakpoints for antibiotic susceptibility testing for some Helicobacter species have not been established. (7)
The patient in this case was discharged on a course of azithromycin with clinical improvement: at that time, the sequencing result revealing Helicobacter had not yet been received, and the clinical team was acting on the belief that the organism in the patient’s blood was a recurrence of the previous Campylobacter infection. On a follow up outpatient appointment with Infectious Disease, wherein sequencing results were available, tetracycline was prescribed due to concern about the possibility of resistance or relapsing infection.
References
Abidi, Maheen Z., et al. “Helicobacter Canis Bacteremia in a Patient with Fever of Unknown Origin.” Journal of Clinical Microbiology, vol. 51, no. 3, 2013, pp. 1046–1048.
Araoka, Hideki, et al. “Clinical Characteristics of Bacteremia Caused by Helicobacter Cinaedi and Time Required for Blood Cultures To Become Positive.” Journal of Clinical Microbiology, vol. 52, no. 7, 2014, pp. 2745–2745.
De Luca, et al. “Helicobacter Pylori Bacteremia: An Unusual Finding.” Infectious Disease Reports, vol. 8, no. 3, 2016, pp. 74–75.
Han, Xiang Y., et al. “Helicobacter Pylori Bacteremia with Sepsis Syndrome.” Journal of Clinical Microbiology, vol. 48, no. 12, 2010, pp. 4661–4663.
Imataki, Osamu, et al. “Enteral Malakoplakia Prior to Helicobacter Cinaedi Bacteremia.” American Journal of Gastroenterology, vol. 112, no. 1, 2017, pp. 187–188.
Saito, Sho, et al. “Helicobacter Fennelliae Bacteremia: Three Case Reports and Literature Review.” Medicine, vol. 95, no. 18, 2016, p. e3556.
Yamamoto, Kei, et al. “Comparison of the Clinical and Microbiological Characteristics of Campylobacter and Helicobacter Bacteremia: the Importance of Time to Blood Culture Positivity Using the BACTEC Blood Culture Systems.” BMC Research Notes, vol. 10, no. 1, 2017, pp. 1–6.
-Tom Koster, DO is a 1st year Anatomic and Clinical Pathology Resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 60 year old male with a past medical history of ulcerative colitis requiring total proctocolectomy and immunomodulatory therapy followed by an anti-Tumor Necrosis Factor α blocker for the last two years and primary sclerosing cholangitis with subsequent decompensated cirrhosis that ultimately required an orthotopic liver transplant on tacrolimus and prednisone for immunosuppression presents 17 days post-transplant with worsening headache for two weeks with associated word finding difficulty and expressive aphasia.
Laboratory and Diagnostic Findings
Brain magnetic resonance imaging demonstrated, a “Heterogeneous, partially hemorrhagic and centrally necrotic mass within the posterior left temporal lobe…infectious etiologies such as pyogenic/non-pyogenic abscesses to include fungal organisms, are highest on the differential” (Image 1). At the time of admission, his complete blood count demonstrated a leukocytosis (16.48×109 cells/L), anemia (hemoglobin of 7.8 g/dL, hematocrit of 24.8%) and a normal platelet count (367×109 cells/L). The automated differential showed 82% neutrophils, 10% lymphocytes, 6% monocytes, 1% eosinophils, and 1% basophils. A lumbar puncture was performed to obtain cerebral spinal fluid (CSF) and the analysis showed a glucose of 60 mg/dL, protein of 34 mg/dL, nucleated cell count of <1, and 6 red blood cells (completely normal CSF indices). Broad spectrum antimicrobials (Vancomycin, Piperacillin/Tazobactam, Metronidazole and Micafungin) were initiated. A 1,3-β-D-glucan test had a result of >500 pg/mL in both serum and CSF. Galactomannan, Histoplasma urine antigen, Cryptococcus antigen and other fungal testing were negative. Antifungal therapy was changed to voriconazole. Craniotomy was determined to be the best course of action and the patient was taken to surgery for debridement and pathologic evaluation.
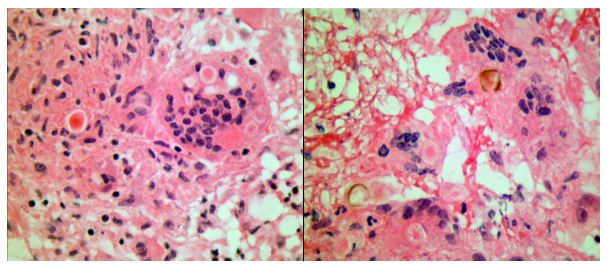
Frozen section evaluation during the time of surgery showed granulomatous inflammation. Septate hyphae were observed on the fungal smear. Following surgery, amphotericin was added. Histologic evaluation of the tissue submitted from surgery showed pyogranulomatous inflammation with pigmented, spore-like structures present in multinucleated giant cells on hematoxylin and eosin (H&E) stain (Image 2). Grocott’s methenamine silver (GMS) stain also highlighted short segments of septate hyphae (Image 3).
Cultures from the surgical debridement grew a mould with central pigmentation (Image 4). Direct microscopic examination of the mould revealed thick-walled, oblong conidia with 3-5 cells, and uniformly pigmented hyphae (Image 5). A germ tube test showed germ tubes originating from both ends of the conidia consistent with Bipolaris species.
Image 1. T1-weighted (left) and T2-weighted (right) magnetic resonance imaging of the brain demonstrating a left temporal lobe mass. Image 2. Hematoxylin and Eosin stained photomicrographs showing pyogranulomatous inflammation with giant cell formation and circular structures within them (left) (40x objective magnification). The right shows gold-brown pigmented structures within granulomatous inflammation (40x objective magnification). Image 3. Grocott’s methenamine silver stain highlighting short segments of irregular septate hyphae in the brain debridement specimen (10x objective magnification).Image 4. Mature wooly brown-black colony on potato dextrose agar. Image 5. Photomicrograph of a lactophenol blue tape prep of the mature fungal colony. Pigmented hyphae and short 3-4 cell conidia are readily identified (40x objective magnification). This specimen also tested germ tube positive (not shown), indicating that this dematiaceous fungus is Bipolaris spp.
The patient’s mental status significantly improved following surgical debridement, 2 weeks of liposomal Amphotericin B, as well as long term treatment with voriconazole. The voriconazole was later switched to posaconazole due to concerns for fluoride toxicity. He completed a year of posaconazole with significant improvement of the abscess observed on imaging and resolution of headaches with no other visual problems. He continued to recover cognitive function with some residual difficulty with reading, comprehension and speech that eventually resolved.
Discussion
Phaeohyphomycosis refers to infections caused by dematiaceous fungi that exist in a variety of forms when seen in tissues and commonly involves skin, soft tissue and nasal sinuses.1 In rare cases, central nervous system (CNS) involvement has been reported. CNS phaeohyphomycosis is predominantly seen in immunosuppressed patients; however, cases involving immunocompetent individuals do exist.2 In one case series from Houston, Texas, five of seven cases of cerebral mycosis were caused by a dematiaceous mould.3 Interestingly, the patient presented in this case came to medical attention around the Dallas-Fort Worth area of Texas.
Cladophialophora bantiana is the most common dematiaceous fungus associated with CNS phaeohyphomycosis, but rare cases of Bipolaris species have been reported previously in literature.4-6
We report a case of CNS phaeohyphomycosis by Bipolaris species following orthotopic liver transplant with an excellent patient outcome. This case is unusual, in part, because the typical hospital course of a patient with phaeohyphomycosis is generally dismal.7 The stories of successful treatment often involve complete debridement of discrete lesions.7-8 In our case, the patient underwent surgical debridement and treatment initially with liposomal Amphotericin B and later transitioned to long term therapy with newer azole antifungals.
References
Revankar SG, Sutton DA, & Rinaldi MG, (2004). Primary Central Nervous System Phaeohyphomycosis: A Review of 101 cases. CID, 38, 206-2016
Filizzola MJ, Martinez F, & Rauf SJ, (2003). Phaeohyphomycosis of the central nervous system in immunocompetent hosts: report of a case and review of the literature. Int J Infec Dis, 7, 282-286
Raparia K, Powell SZ, Cernoch P, Takei H, (2010). Cerebral mycosis: 7-year retrospective series in a tertiary center. Neuropathology, Jun; 30(3): 218-223.
Frank T, Esquenazi Y, Nigo M, Wanger A, Portnoy B, & Shepard S, (2016). Disseminated Phaeohyphomycosis with Brain Abscess and Biliary Invasion Due to Bipolarisspp. In an Immunocompetent Patient. Annals of Clinical & Laboratory Science, 46(4).
McGinnis MR, Campbell G, Gourley WK, & Lucia HL, (1992). Phaeohyphomycosis Caused by Bipolaris spicifera, An Informative Case. Eur. J. Epidemiol, 8(3), 383-386
Rosow L, Jiang JX, Deuel T, Lechpammer M, Zamani AA, Milner DA, Folkerth R, Marty FM, & Kesari S, (2011). Cerebral phaeohyphomycosis caused by Bipolaris spiciferaafter heart transplantation. Transpl Infect Dis, 13, 419-423.
Gadgil N, Kupfermen M, Smitherman S, Fuller GN, Rao G, (2013). Curvularia brain abscess. J Clin Neurosci, Jan;20(1): 172-175.
-John Markantonis, DO is a second year Clinical Pathology resident at UT Southwestern in Dallas. He has interests in Medical Microbiology and Transfusion Medicine.
-Dominick Cavuoti, DO is a Professor at UT Southwestern in the Department of Pathology. He is multifaceted and splits his time as the Medical Director of the Parkland Hospital Clinical Microbiology Laboratory and Parkland Cytology attending among other administrative and educational activities.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
A 18
year old male with no significant past medical history presented with 2-3
month cough, hemoptysis, fevers, night sweats and 15 pound unintentional weight
loss. He originally started to feel mild shortness of breath with activity
following his return from the Pacific Northwest. He was diagnosed with
pneumonia and given antibiotics. He denied vaping, hookah use or any smoking. Of
note, his maternal grandmother had pulmonary tuberculosis two years ago, but at
that time he had a negative interferon-gamma release assay (IGRA). Since that
time he had traveled extensively including Europe and Asia.
Upon
admission, physical examination showed decreased breath sounds and coarse
crackles in the right lower lung field. His blood test results were
unremarkable. Chest X-ray and
CT scan showed diffuse reticular pattern and a 4 cm cavitary lesion in his
right lower lobe (Image 1). Brochoalveolar lavage fluid, sputum as well as
blood were submitted to microbiology lab for bacterial, fungal and
mycobacterial culture.
Image1. Chest X-ray and CT showed diffuse reticular pattern with a 4cm cavitary lesion in his right lower lobe.
Laboratory results and
management
The
patient’s Quanti FERON®-TB Gold test (an IGRA) was positive.Laboratory studies including fungal
culture to look for endemic fungi and HIV were negative. Auramine-rhodamine (acid
fast) staining of sputum smear showed 4+ acid fast bacilli (AFB). Mycobacteriumtuberculosis was confirmed by both our laboratory developed TB-PCR assay and a commercial TB-PCR assay (Xpert MTB/RIF). DNA sequencing
was performed by the Centers for Disease Control and Prevention (CDC) in order to predict antibiotic
susceptibility profiles for first-line anti-tuberculosis drugs including Ethambutol,
Isoniazid, Pyrazinamide, and Rifampin.
Because the result showed drug-susceptible tuberculosis, the patient started the first-line
anti-tuberculosis drugs. Four days after admission, the patient discharged home
with follow up with the department of health. After six weeks incubation, the
sputum culture grew Mycobacteriumtuberculosis with a pan-susceptible antibiotic
profile.
Image 2. Ziehl-Neelsen stain of acid fast bacilli (AFB) on sputum smear. Image from the CDC website.
Discussion
Mycobacterium tuberculosis
(MTB) remains a global
health problem. The continuing spread of drug-resistant tuberculosis is one of
the most difficult challenges for MTB control. The CDC recommends rapid
laboratory confirmation of MTB with using a nucleic acid amplification test
(NAAT), followed early drug susceptibility testing. Our case is consistent with
the previous reports that NAAT can identify MTB and DNA sequencing can
determine the drug susceptibility within a few days. Our case can be summarized
into two points.
First,
early NAAT provided diagnosis MTB within 2 days after patient admission,
enabling the timely initialization of infection control measures. Although
culture remains the gold standard for laboratory confirmation of active TB
infection, it can take 6-8 weeks to grow in a culture media since MTB is slow
growing pathogen. Early laboratory confirmation of MTB with NAAT led rapid
initiation of the patient treatment and transmission interruption.
Second,
DNA sequencing guided us to start an optimal anti-tuberculosis treatment within
3 days because of the accurate prediction of susceptibility profiles for
first-line anti-tuberculosis drugs. In comparison, the conventional
susceptibility testing with the drug-containing medium requires 1 month to
complete beyond initial growth and identification of the organism. Recent
studies demonstrated high accuracy of genotypic predictions (>91.3 %
sensitivity; >93.6% specificity). Our case supports a theory that DNA
sequencing can help to determine which anti-tuberculosis drugs should be used
for treatment.
Despite
the notable advantage, NAAT has limitations. There is a relatively low positive
predictive value in smear-negative pulmonary MTB. Recent meta-analysis found
that overall sensitivity of NAAT to be 90.4% for diagnosis of pulmonary MTB.
The sensitivity of the NAAT further defined to be lower in smear negative (75%)
compared to smear positive (98%) pulmonary MTB. Additionally, cost effectiveness
of NAAT and DNA sequencing is another concern. Further assessments of the
benefit of NAAT and DNA sequencing utilization for smear negative MTB are
needed.
In
conclusion, our case demonstrated that NAAT and DNA sequencing was beneficial
to reduce the time to initiation of an optimal MTB management.
References
Prediction of Susceptibility to First-Line
Tuberculosis Drugs by DNA Sequencing. N Engl J Med 2018; 379: 1403-15.
Use of Nucleic Acid Amplification Tests
in Tuberculosis Patients in California, 2010-2013. Open Forum Infect Dis. 2016
Oct; 3(4): ofw230.
Assessment by Meta-Analysis of PCR for
Diagnosis of Smear-Negative Pulmonary Tuberculosis. J Clin Microbiol. 2003 Jul;
41(7): 3233-3240.
-Sachie Ikegami MD, PhD is a 1st year anatomic and clinical pathology resident at University of Chicago (NorthShore). Sachie’s academic interests include neuropathology and molecular pathology. She is passionate about understanding how pathology informatics improving clinical practice. Outside of the lab, she enjoys jogging.
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.
An elementary school age child presented to the pediatric emergency department with an acute onset of abdominal pain. According to the parents, the patient recently had an ear infection and completed a course of amoxicillin. They noted the patient was more tired than usual, but did not have a fever. They reported no recent sick contacts or travel. Past medical history was significant for constipation, but normal bowel movements were noted over the past few days. On physical exam, the abdomen was soft and non-distended with diffuse mild tenderness noted on the right side. No masses were noted. Laboratory testing was unremarkable and the WBC count, liver & pancreas enzymes, and alpha fetal protein were within normal limits. An abdominal CT scan revealed a mass with central necrosis in the liver concerning for an abscess. The patient was started on ceftriaxone & metronidazole and underwent a surgical procedure to drain the lesion.
Laboratory Identification
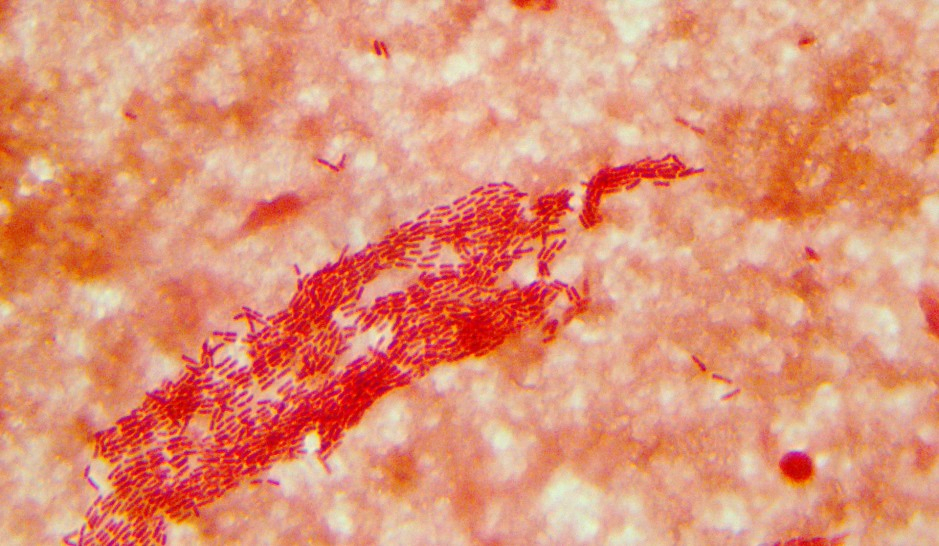
Image 1. Gram stain of the direct liver aspirate showed many gram positive cocci in pairs & chains and numerous white blood cells (oil immersion). Image 2. Rare small, white non-hemolytic colonies grew on CDC agar after 42 hours of incubation at 35°C under anaerobic conditions.
No bacterial growth was observed on blood or chocolate agars incubated at 35°C in CO2. MALDI-TOF mass spectrometry identified the isolate as a viridans groups streptococci, Streptococcus intermedius. The organism was susceptible to penicillin, ceftriaxone, and vancomycin by broth microdilution. Blood cultures were not collected for this patient.
Discussion
Streptococcus intermedius is a viridans group streptococci that belongs to the S. anginosus group. The S. anginosus group also includes S. anginosus and S. constellatus. This group of viridans streptococci composes the normal flora of the oropharynx, urogenital, and gastrointestinal tracts. These organisms are known for causing peritonitis and abscesses, particularly in the brain, breast, liver, and oral cavity.
Similar to other streptococci, S. intermedius is a gram positive cocci that grows in chains and is catalase negative. The anginosus group are facultative anaerobes and grow as pinpoint colonies (<0.5 mm) on blood agar. This is in contrast to pyogenic, beta-hemolytic streptococci which are greater than 0.5 mm in size after the same incubation period. The anginosus group streptococci can exhibit a variety of hemolysis patterns, including alpha, beta, or gamma hemolysis. A distinct butterscotch or caramel odor is noted on examination. The anginosus group can possess Lancefield antigens A, C, F, G, or be non-groupable, so it is important not to misidentify them as other streptococci that also have these antigens.
Historically, further identification of viridans group streptococci was challenging; however, the advent of automated systems and MALDI-TOF mass spectrometry has been useful in providing species level identifications for more common isolates. Molecular sequencing methods using sodA gene can be helpful as well for the most reliable results. While penicillin resistance is becoming more frequent in viridians group streptococci, it is still rare in the S. anginosus group.
In the case of our patient, an echocardiogram was performed and found to be negative for endocarditis. The patient’s symptoms improved and they were discharged home on ceftriaxone and metronidazole. A follow up CT scan to confirm resolution of the abscess was scheduled.
-Lisa Stempak, MD is the System Director of Clinical Pathology at University Hospitals Cleveland Medical Center in Cleveland, Ohio. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Her interests include infectious disease histology, process and quality improvement, and resident education.
A 73 year old patient with a medical history significant for diabetes and diabetic foot ulcers presented to an outpatient orthopedic clinic complaining of right foot pain and fevers. Physical exam findings were significant for a right metatarsal ulceration that extended to the bone which prompted admission to a local hospital. Tissue from debridement of this ulcer was sent for routine bacterial culture and blood cultures were also collected. The patient was started on empiric antibiotics.
Laboratory Findings
The tissue culture gram stain showed mixed gram negative and gram positive bacteria. Two days after admission, an anaerobic blood culture bottle flagged positive with gram negative rods which could not be identified by Verigene nucleic acid detection test. It was plated on routine anaerobic and aerobic culture plates for further identification. Four days after admission, another blood culture set flagged positive with staphylococci which was identified on the Verigene as methicillin susceptible Staphylococcus aureus in the aerobic bottle. Seven days after admission, the gram negative organism grew and was identified by MALDI-TOF mass spectrometry as Campylobacter ureolyticus. The tissue culture grew mixed gram positive and negative bacteria including Staphylococcus aureus, Bacterodies fragilis group, and Trueperella bernardiae. The patient’s antibiotic therapy was tailored to cover the MSSA and Campylobacter and they were successfully discharged.
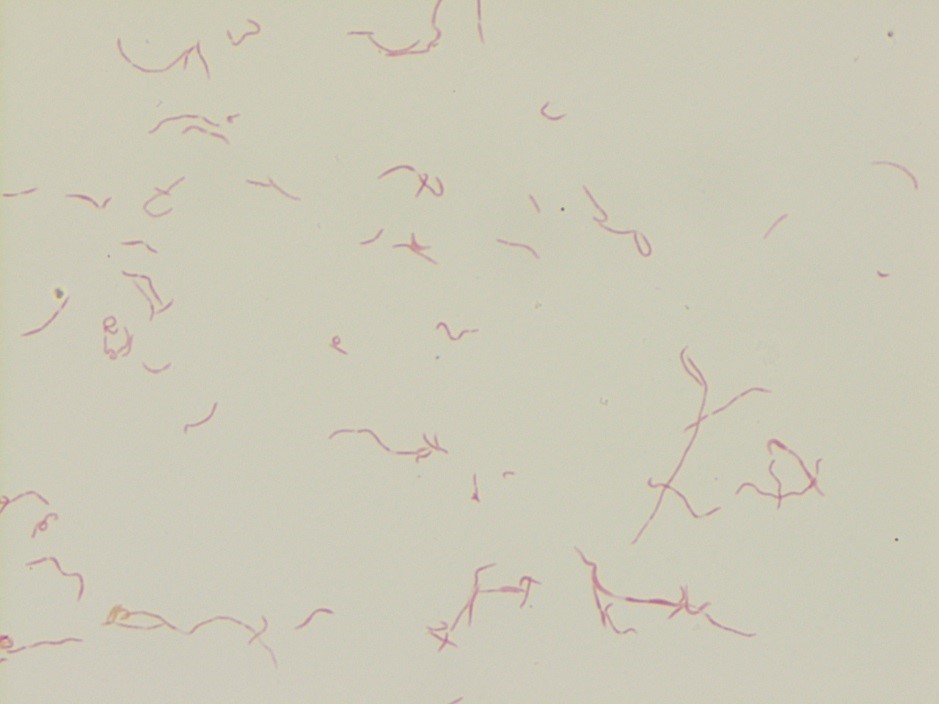
Image 1. Colony gram stain of Campylobacter ureolyticus isolated from the patient’s blood culture. The bacteria appear as thin S-shaped gram negative rods.
Discussion
The Campylobacter
genus has 24 species of bacteria including C.
jejuni and C. coli which are the
most frequent cases of campylobacteriosis, a diarrheal illness which is described
below. Other less frequent pathogenic species include C. fetus, C. upsaliensis,
C. lari, and C. ureolyticus. Campylobacter
species appear as a curved S-shaped spiral rods and are gram negative on gram
stain, are nonspore forming, and motile, with the exception of C. ureolyticus, which is aflagellate.
Because Campylobacter is difficult to
culture, rapid detection tests have been developed including antigen detection
tests, however, these lack specificity. Several FDA approved nucleic acid amplification tests for Campylobacter exist, such as the BD MAX enteric bacterial panel
that can detect C jejuni/C coli (speciation
requires a reference lab).
Campylobacter
grows best under microaerophilic conditions and at 42o C (closer to
the body temperature of chickens). C.
ureolyticus is unique as it grow anaerobically. Media that is selective and
differential for Campylobacter,
including charcoal cefoperazone deoxycholate agar (CCD) and charcoal based
selective medium (CSM), is often used for stool specimens. Campylobacter appears as flat grey colonies that tend to spread
along streak lines. Identification of Campylobacter
includes a characteristic gram morphology, growth microaerophilically (expect
for C. ureolyticus), and oxidase
positivity. C. jejuni are hippurate hydrolysis positive. C. coli are hippurate hydrolysis negative, however, there are C. jejuni that are hippurate hydrolysis
negative, making this test non-specific.
Clinical and Laboratory Standards Institute (CLSI)
recommends antibiotic susceptibility testing for C. jejuni and C. coli and
includes testing for ciprofloxacin, erythromycin, and tetracycline resistance which
requires microaerophilic conditions.
Campylobacter is
mainly a zoonotic disease acquired from poultry, cattle, sheep, pigs, and
domestic pets. C. ureolyticus, is
thought to be transmitted most frequently form cattle, however, more research
is needed in this area. A common cause of Campylobacter
is consumption of undercooked meat, especially poultry due to the high
prevalence of Campylobacter in US
retail poultry. In 2015, 5,000 US retail poultry samples were tested for Campylobacter with 12% of samples testing
positive; 24% of chicken breast samples tested positive and 0.2 % of ground
turkey samples tested positive. The majority of isolates were C. jejuni and C. coli (65% and 34% respectively). In 2004, 60% of chicken samples
tested positive in the US (1). Campylobacter
most frequently infects young children ages 1-5 as well as adolescents and
young adults and is most frequently seen between the months on June and August
(1).
C. ureolyticus is
a less studied species of Campylobacter,
however there is evidence that this species can cause diarrheal disease and
extra –intestinal infections. Some studies of fecal specimens from patients
presenting with diarrhea illness in Ireland revealed 24% of Campylobacter positive stools were C. ureolyticus species (4). C. ureolyticus has also been isolated
skin and soft tissue abscesses, however, C.
ureolyticus is rarely the sole bacteria isolated, raising the questions of
whether it a true soft tissue pathogen. The most frequent soft tissue site of infection
is the perianal region (4).
Campylobacter
usually presents as a diarrheal illness, causing fever, diarrhea (can be bloody
or non-bloody), and abdominal cramping with symptoms lasting days to weeks. The
disease is usually self- limited, but in 10-15% of cases patients are admitted
to hospitals (1). Generally, patients will clear campylobacter enteritis
without the need for antibiotics. Indications for antibiotics include severe
bloody diarrhea, relapsed cases, high fever, greater than 1 week course, and
extraintestinal infections or immunocompromised status. Interestingly, presentations
of C. jejuni/C. coli can mimic appendicitis and lead to unnecessary
appendectomies. Extra-intestinal infections include bacteremia, septic
arthritis, abscess formation, meningitis, peritonitis, prostatitis, urinary
tract infections, and neonatal sepsis. Guilian-barre syndrome can be seen after
C. jejuni infections, especially the
heat stable serotypes HS19 and HS41, which is medicated by antibodies that
develop against ganglioside-like epitopes in the bacterial cell wall LPS region
which cross react with peripheral nerve gangliosides. C. jejuni/C. coli can
also induce reactive arthritis and rarely have been implicated in inciting
inflammatory bowel disease exacerbations and celiac disease (1-2).
In severe infections or extraintestinal infections, azithromycin
is the preferred antibiotic as fluoroquinolone resistance is rising in the US. In
2014, 27% of C. jejuni and 36% of C. coli isolates were resistant to ciprofloxacin,
and 2% of C. jejuni and 10% of C. coli isolates were resistant to
azithromycin (1-2). In an Italian cohort of patients, greater than 60% of Campylobacter strains were ciprofloxacin
or tetracycline resistant, while 29% of C.
coli isolates were resistant to tetracycline, fluoroquinolones, and
macrolides (3). Interestingly, use of these antibiotics in animal feed has been
directly associated with the occurrence of antibiotic resistant Campylobacter
stains (1-3). Antibiotic resistance and guidelines for the management of C.ureolyticus
infections is largely unknown.
Overall, Campylobacter
usually presents as a self-limiting diarrheal illness, however, less frequently
extra-intestinal infections can occur such as in this patient’s case. The most
common pathogenic species include C.
jejuni and C. coli, while other Campylobacter species are seen less
frequently. In this patient’s case, C.
ureolyticus was isolated from the
blood after the patient developed a right metatarsal ulcer. While we were
unable to culture Campylobacter from
the patient’s wound culture, this is the most likely source of their blood
stream infection.
References
Whitehouse CA, Young S, Li C, Hsu CH, Martin G,
Zhao S. Use of whole-genome sequencing for Campylobacter surveillance from
NARMS retail poultry in the United States in 2015. Food Microbiol.
2018;73:122-128.
Tack DM, Marder EP, Griffin PM, et al.
Preliminary incidence and trends of infections with pathogens transmitted
commonly through food – Foodborne Diseases Active Surveillance Network, 10 U.S.
sites, 2015-2018. Am J Transplant. 2019;19(6):1859-1863.
Garcia-Fernandez A, Dilonisi AM, Arena S,
Iglesias-Torrens Y, et al. Human Campylobacteriosis in Italy: Emergence of
Multi-Drug Resistance to Ciprofloxacin, Tetracycline, and Erythromycin. Front
Microbiol. 2018 Aug 22;9:1906. doi: 10.3389/fmicb.2018.01906. eCollection 2018.
O’donovan D, Corcoran GD, Lucey B, Sleator RD.
Campylobacter ureolyticus: a portrait of the pathogen. Virulence.
2014;5(4):498-506.
-Liam Donnelly, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
A 54 year old male former smoker and alcohol user presented
to the Emergency Department with a five day history of nausea, vomiting,
diarrhea, weakness, fever with chills, breaking out in sweats, and abdominal
discomfort. He denied recent sick contacts, travel or exposure to potentially
contaminated foods. He had a past medical history that was significant for
Chronic Obstructive Pulmonary Disease (COPD), mitral valve regurgitation and ST
elevation myocardial infarction (STEMI). Some of his medications are inhaled
Fluticasone, Advair Diskus, Furosemide and Spironolactone. He has also had a
mitral valve replacement.
His initial laboratory tests revealed leukocytosis with
neutrophilia, non-specific electrolyte derangements and negative stool tests
for enteric bacterial pathogens. His symptoms progressed within the first 24
hours of admission, with a decrease in oxygen saturation (SPO2) and
dyspnea so further investigations were carried out. Subsequently, a chest X-Ray
was done, which showed pneumonia. The patient had a bronchoscopy and bronchoalveolar
lavage (BAL) fluid was sent to the laboratory for aerobic, fungal, and acid fast
bacilli culture, as well as Legionella
spp. and Pneumocystis jiroveci direct
fluorescent antigen testing.
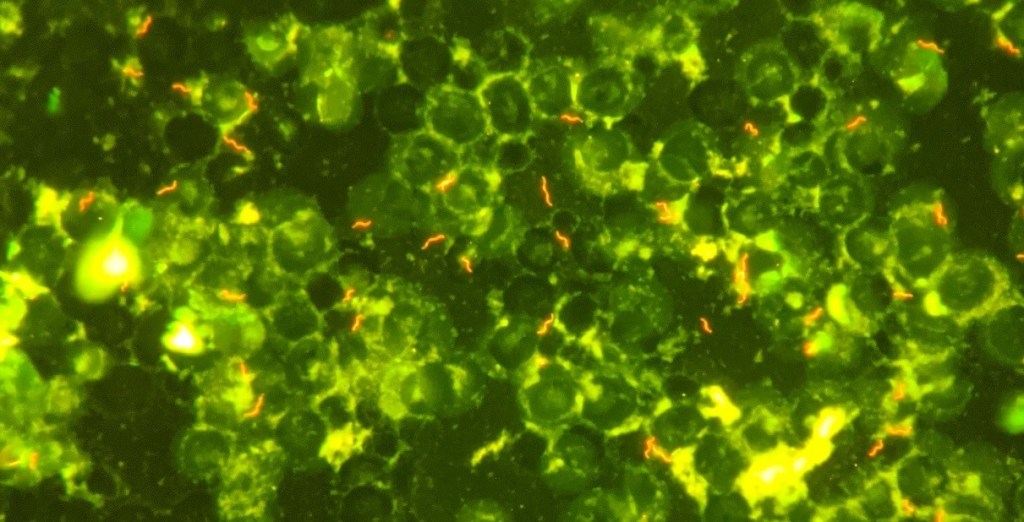
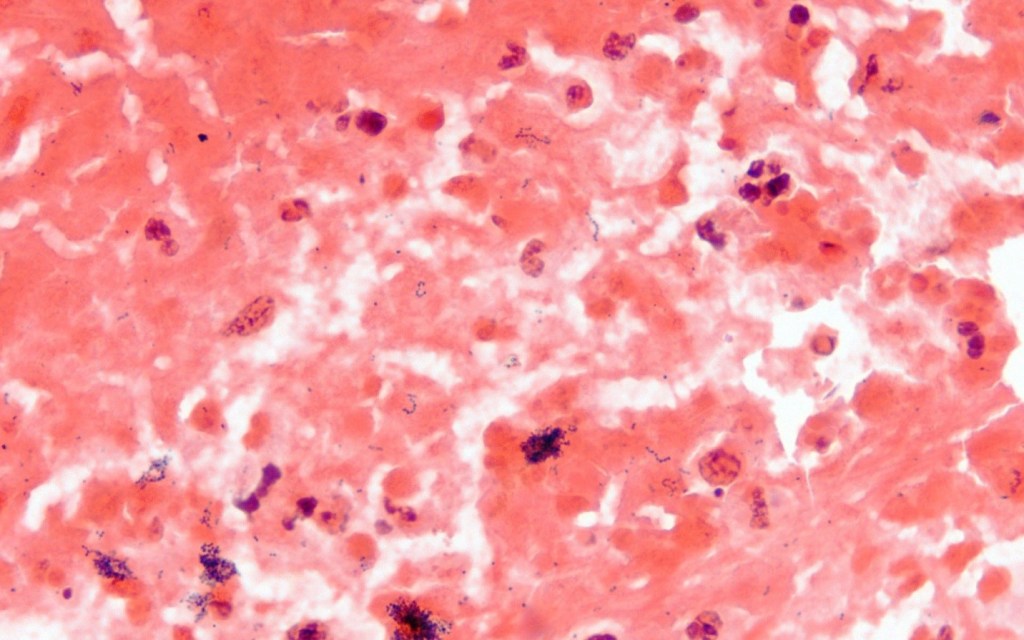
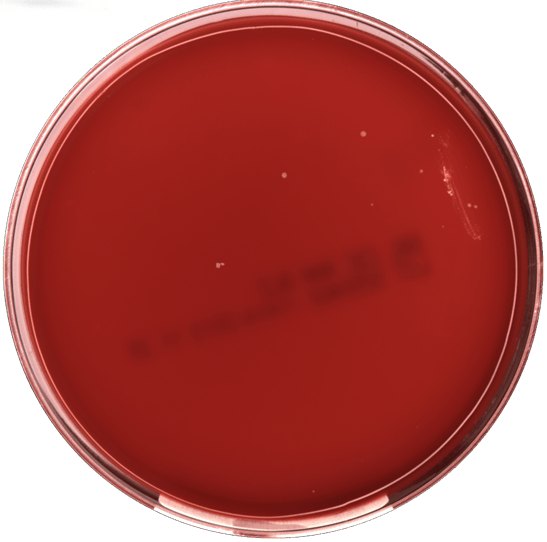
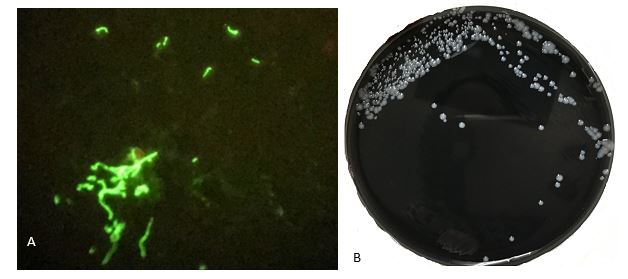
Image 1. Results of Bronchoalveolar Lavage. A. Direct Fluorescence Antibody to Legionella antigens; B. Legionella pneumophilia colonies on Buffered Yeast Charcoal Extract agar plate (BCYE), showing convex, round colonies with entire edges.
Discussion
The presence of pneumonia and diarrhea in the patient raised
suspicion for Legionnaires’ Disease, so the patient’s specimens including BAL
fluid and bronchial washings were tested by direct fluorescent antigen (Image
1A) which confirmed Legionnaires’ Disease as the diagnosis.
Legionnaires’ Disease (LD), is a form of pneumonia caused by
Legionella species, most commonly Legionellapneumophilia. Legionella spp.are motile, obligate aerobic,
facultative intracellular and weakly gram negative rods. They are also
nutritionally fastidious, requiring specific nutrients such as L-cysteine, and iron.
They live in amoebas or in biofilms all over the world and are seen in high
concentrations in warm waters plumbing systems, water heaters, warm water spas
and cooling towers, and in very low concentrations in freely flowing cold water
and biocide-treated waters.1 They are disseminated by devices that
aerosolize water such as cooling units, hot tubs, water fountains and showers
and cause disease when this contaminated aerosolized water is inhaled. The
inhaled bacteria then enter the bacteria-killing macrophages in the lungs. Once
in, they hijack the intracellular mechanism of the macrophages, feed off them, multiply
within them, and then kill the macrophages, releasing more bacteria into the
surrounding tissues.1
The incubation period of Legionella infections is 2 to 14
days, with a median of 4 days. In humans, Legionellaspp. causes Legionellosis which comprises
two separate diseases. These are Pontiac fever, a mild, self-limited flu-like
illness, and LD, an atypical form of pneumonia which affects multiple organs.
LD can range from mild to fatal in severity and about 12% of patients die from
the disease.1 In most cases, LD begins with fever and symptoms of
gastrointestinal infection including diarrhea and vomiting before patients
develop respiratory symptoms such as cough and difficulty in breathing. However,
LD also involves other organs/systems, causing renal failure and cardiogenic shock.
LD occurs world-wide and all-year round but most cases occur between late fall
and early spring.1
Although LD is relatively rare in the US, it is believed to
be underdiagnosed due to failure to test for Legionella infection, poor
sensitivity of test methods used to detect the disease, and failure to report all
diagnosed cases.1 However, the rate of reported cases in the US has
increased by about 5.5 times in the past 20 years to 7,500 reported cases in
20172, which may be partially attributed to increased and improved
testing.
LD is more likely to occur in people with a suppressed
immune system – particularly those on high-dose corticosteroids like
Fluticasone, people with chronic lung, heart or kidney diseases, people who
smoke or smoked in the past, people who travel, especially overnight travel,
people who have received solid organ transplants, and people who use certain
medications such as anti-tumor necrosis factor drugs.1 LD is often
fatal and survival depends on how severe the pneumonia when treatment starts,
the presence or absence of other serious comorbidities, and how early specific
treatment for the disease is commenced.1 Therefore, prompt diagnosis
is very important to survive LD.
Unfortunately, LD patients often present with nonspecific symptoms
as well as chest X-ray, biochemical and hematological laboratory tests results.
Therefore microbiological investigations which identify Legionella spp. are crucial in the management of these cases. The
most commonly used test method is the Urinary Antigen test which detects the most
common cause of Legionnaires’ disease, L.
pneumophila serogroup 1. But, it does not detect other potentially
pathogenic Legionella species and serogroups. Legionella spp. can also be cultured and identified, but this requires
the use of Buffered Charcoal Yeast Extract [BCYE] agar which provides the
specific growth requirements of Legionella
spp.Common specimens for culture
include lower respiratory secretions such as BAL and bronchial washings, lung
tissue and pleural fluid. Other methods used to diagnose LD include polymerase
chain reaction (PCR), direct fluorescence antibody (DFA), and paired serology.
However, the Centers for Disease Prevention and Control, CDC recommends testing
with culture and urinary antigen test in combination.2
LD is treated with Azithromycin or Levofloxacin. 95 to 99%
of cases can be cured if they are otherwise healthy but treatment is started
early.1
References
Edelstein, Paul H. and
Lück, Christian. “Legionella.” In Manual of Clinical Microbiology,
Eleventh Edition, pp. 887-904. American Society of Microbiology, 2015.
–Adesola Akinyemi, M.D., MPH, is a first year anatomic and clinical pathology resident at University of Chicago (NorthShore). He is interested in most areas of pathology including surgical pathology, cytopathology and neuropathology–and is enjoying it all. He is also passionate about health outcomes improvement through systems thinking and design, and other aspects of healthcare management. Find him on Twitter: @AkinyemiDesola
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical
Microbiology NorthShore University Health System in Evanston, Illinois.
Follow Dr. McElvania on twitter @E-McElvania.