Case History
A 42 year old male with past medical history of diabetes mellitus and essential hypertension presented to the emergency department with high fever and chills which developed two days prior. His examination revealed a painful ulcer on the planter aspect of his right toe with surrounding erythema. According to patient, the exact duration of the ulcer is unclear as it was on planter aspect of his foot and he does not inspect his feet regularly. However, the ulcer grew in size and symptoms over the past week. He denies any cough, diarrhea or abdominal pain. He is on oral anti-diabetics with well-controlled blood sugar. Complete blood count revealed leukocytosis. Blood was collected and sent to microbiology laboratory for gram stain and culture.
Laboratory identification
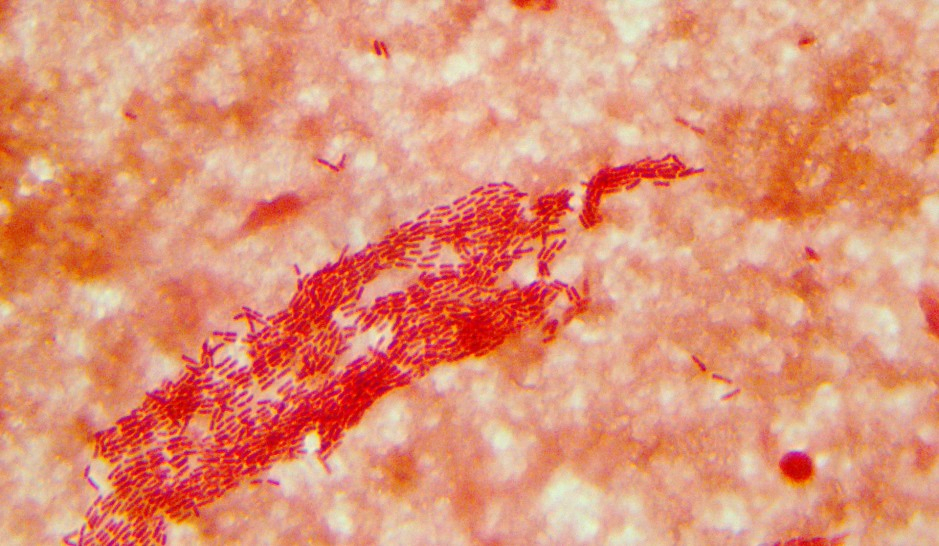
Cultures signaled positive after 32 hours of incubation and gram negative rods were identified on Gram stain (Image 1). The organism grew after 24 hours of incubation on 5% sheep blood, chocolate, and MacConkey agars (Images 2 & 3). MALDI-TOF mass spectrometry identified the isolate as Salmonella spp. The isolate was sent to the public health department for additional testing by molecular typing where it was identified as Salmonella enterica subsp. enterica serovar Brandenburg (Salmonella Brandenburg). Later, MRI revealed osteomyelitis of right third toe which was considered as the likely source of patient’s bacteremia.


Discussion
Salmonella is a genus of the family Enterobacteriaceae in the order Enterobacterales. They are non-spore forming gram negative facultative anaerobes. Salmonella spp. are lactose non-fermenters and usually produce H2S on triple sugar iron and Hektoen enteric agar.
The genus has only two species: Salmonella enterica, divided into 6 subspecies and containing over 2500 serovars, and Salmonella bongori. Subspecies and serotype determination is necessary for epidemiological investigations. Serotyping is used to classify Salmonella based on bacterial surface antigens; the thermostable polysaccharide cell wall or somatic (“O”) antigens and the thermo-labile flagella proteins or “H” antigens. It is also possible to identify Salmonella serotypes on the basis of phage typing, plasmid profiling, ribotyping and pulsed field gel electrophoresis (PFGE) of DNA fragments generated from restriction enzyme digestion.
Salmonella are zoonotic bacteria that can cause abortion, metritis, and systemic illness in ewes and does. Natural reservoirs of Salmonella are domestic and wild animals, including poultry, swine, cattle, birds, dogs, rodents, tortoises, turtles and cats. Humans also serve as a natural host. The most common source of transmission of Salmonella is the consumption of contaminated poultry and meat products. Person-to-person, fecal–oral transmission does occur and has been a problem in health care facilities traced to inadequate hand washing.
Salmonella brandenburg ranked 16th among the serovars responsible for human infections. It causes acute diarrhea and severe illness in a variety of animals and was first isolated in New Zealand in 1986. Since 1996 Salmonella Brandenburg has been associated with an emerging epidemic of abortions and deaths in sheep in the southern regions of the South Island. Subsequently, the same strain was reported to cause disease in horses, goats, deer, pigs and humans. The disease is known to have high morbidity and mortality within a flock or herd, rapid local spread and an occupational, health and safety risk to farm workers and their families.
There are three clinically distinguishable forms of salmonellosis in humans. These include gastroenteritis, enteric fever and septicemia. Established Salmonella bacteremia requires aggressive antimicrobial treatment with ciprofloxacin, ceftriaxone, or less frequently trimethoprim-sulfamethoxazole. A careful search for focal metastatic disease should be undertaken, especially when relapse follows cessation of treatment. Surgical drainage of metastatic abscesses may be required, with surgical intervention. Resistance to any of the drugs used to treat invasive infection may occur, so treatment should be supported by susceptibility testing.
In the case of our patient, he was treated with ceftriaxone and underwent toe amputation. The patient had an uncomplicated hospital course and made a complete recovery.
- Alvseike O., Skjerve E. (2000). Probability of detection of Salmonella using different analytical procedures, with emphasis on subspecies diarizonae serovar 61:k:1,5,(7) [S. IIIb 61:k:1,5,(7)]. International Journal of Food Microbiology, 58, 49-58.
- Clark G, Swanney S, Nicol C, and and Fenwick S. Salmonella Brandenburg – the 1999 Season. Proceedings of the Sheep and Beef Cattle Society of the New Zealand Veterinary Association, 151-156, 2000
- Bailey K.M. (1997). Sheep abortion outbreak associated with Salmonella Brandenburg. Surveillance, 24(4), 10-11
- Baumler A.J., Tsolis R.M., Heffron F. (2000). Virulence Mechanisms of Salmonella and their Genetic Basis. In “Salmonella in Domestic Animals” (Ed. C. Wray and A. Wray). CAB International 2000, pp. 57-72

-Ansa Mehreen, MD. 1st year AP/CP resident at University of Chicago hospital program based at Evanston Hospital. Her academic interests include gastrointestinal pathology.

-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.

Was there any evidence of the patient being in contact with infected animals, or ingesting food contaminated with salmonella spp.? The source of bacteraemia in the patient was not clear and it’s link to the toe’s abscess (I assumed that this was an overall picture of the general state of health of the patient).
Image 2 appears to be HE agar.
Thank you for the catch! We’ve updated the caption accordingly.