Case History
A male teenager presented to the emergency department following a 4 wheeler accident. He sustained extensive trauma to his right lower leg with a large, dirty laceration and grossly exposed muscle. His pulses were intact and motor & sensory nerve function were preserved. The wound was irrigated at the bedside and the patient was admitted with a plastic surgery consult for wound coverage. Cefepime was empirically started. After 10 days in the hospital and multiple surgeries to care for the wound, the patient developed a fever and increased pain, erythema, and swelling at surrounding the wound. The trauma service ordered blood and wound cultures.
Laboratory Identification


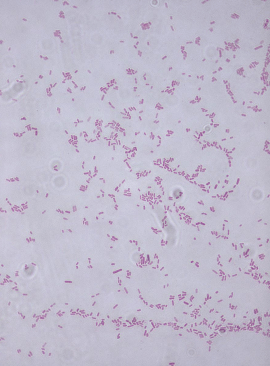
The oxidase reaction was negative. MALDI-TOF mass spectrometry identified the isolate as Stenotrophomonas maltophilia from the wound culture. Blood cultures were negative.
Discussion
Stenotrophomonas maltophilia is a common non-fermenting gram negative rod that is ubiquitous in moist environments but is not commonly a member of human flora. S. maltophilia can readily be isolated from hospital surfaces and those with traumatic injuries, prolonged hospitalizations, on mechanical ventilation, and with in-dwelling devices are more susceptible to nosocomial infections by this organism. Those who are immunocompromised or have cystic fibrosis are also at an increased risk.
In the laboratory, S. maltophilia is characterized as an aerobic, Gram-negative rod that grows as lavender-green colonies on blood agar (Image 1) and has an ammonia-like odor. This organism is catalase and oxidase negative and DNase positive. S. maltophilia is motile and is able to utilize glucose and maltose by oxidative fermentation. Current automated identification systems and MALDI-TOF mass spectrometry are able to accurately identify S. maltophilia.
S. maltophilia is intrinsically resistant to many broad-spectrum antibiotics, including carbapenems and aminoglycosides. Beta-lactam resistance is due to two beta-lactamases and renders beta-lactam inhibitors ineffective. Trimethoprim-sulfamethoxazole (TMP-SMX) is the antibiotic of choice to treat S. maltophilia infections; however, resistance can develop. In the case TMP-SMX resistance, ceftazidime, minocycline, ticarcillin-clavulanate, ciprofloxacin, and levofloxacin can be tested.
In the case of our patient, susceptibility testing was performed on the Vitek2 instrument and the isolate was susceptible to TMP-SMX. He was switched to TMP-SMX and underwent additional surgical procedures to wash out the infected area.

-Karla Perrizo, MD, is a Clinical Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD is the System Director of Clinical Pathology at University Hospitals Cleveland Medical Center in Cleveland, Ohio. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Her interests include infectious disease histology, process and quality improvement, and resident education.
