One of my favorite scary movies is the original Fright Night, a campy horror film from the 1980s. In it, the main character, Charlie, discovers he is living next door to a vampire. He realizes there is danger, so the first thing he does is research. He asks his friend “Evil Ed” about vampire knowledge and tries to get as much information as possible. He performs a risk assessment in his home and then puts into place some engineering controls (crosses, wooden stakes, windows nailed shut), some PPE (a garlic necklace), and even work practice controls (do not invite a vampire into your home). Charlie also utilizes help in the form of an out-of-work actor who starred in cheesy vampire flicks. These actions taken by Charlie make sense: he takes the time to learn about the danger, and then he prepares to deal with it safely.
As a lab safety professional, I often wonder why people who work in the laboratory do not follow the same pathway. They are educated in school and in training about the multiple dangers in the department, but many work throughout their lab careers utilizing unsafe practices. For example, it is common for staff in a histology lab to work with or near sharp blades in cryostats and microtomes without using any implements or safety guards. The number of reported cuts that repeatedly occur in these labs is shockingly high, and the number of unreported injuries is likely much higher. What is interesting is that when having conversations with those laboratorians, they are fine with accepting the risk and accepting the injuries or exposures when they occur.
The concept is the same, isn’t it? Vampire teeth can kill you, so you protect yourself. Bloodborne pathogens and sharps can also be deadly, but why isn’t there concern about the use of safe lab practices with blades? There may be a few reasons.
The use of large, sharp blades is, of course, common in histology labs. They are a part of the everyday job. Hands go near them when tissue is cut, when tissue blocks are changed, when moving the blade, and when changing the blade. In some busy cutting labs, a microtome blade can be changed up to twenty times a shift. This ubiquitousness of this item tends to create a sense of complacency about it. Yes, people have been injured, some badly, some amputations have even occurred, but in comparison to the number of tissue blocks cut, those reported injuries may seem like small numbers…unless it happened to you.
Another reason for complacency is that often, when blade injuries occur, the blade has been used with fixed (and essentially harmless) embedded tissue or when they haven’t been used at all. Many cuts are “clean” and minor, so there is no true perception of danger.
A third reason I have often heard about why blades are handled with no safety measures in place is that productivity in the lab is key. There are standards about how many tissue sections should be made during a standard shift, and using implements to move or change the blade would hinder those goals. Read that again- productivity, in the minds of some, is more important than staff safety – and that is an acceptable stance for them.
As a lab safety professional, one of my goals is to change that unsafe mindset. It does not matter in which section of the laboratory work is performed, staff should be made aware of the risks, and they should be taught how to utilize engineering controls, administrative controls, and PPE to avoid the hazards in the department. Then there should be ongoing management of the safety program which includes risk assessments, safety audits, and follow up when injuries or exposures do occur.
Train those who work with blades in the department. Show them how to work with and handle them safely by using magnet-tipped brushes and rubber-tipped forceps to change and move them. Teach them to always engage the blade guards when hands go anywhere near the blade. Talk about serious cuts and amputations that can occur when unsafe practices are utilized. Review work practices regularly to ensure staff remain safe each time they use the equipment associated with the blades. With sharp blades, the danger has already been invited into the lab. Take the next best precautions you need to make sure your blade doesn’t bite and become a “fright knife.”
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
A recent report from the Centers for Disease Control and Prevention (CDC) revealed that after the emergence of the COVID-19 pandemic, antibiotic resistance has increased by at least 15%. In particularly, the extended spectrum beta-lactamase (ESBLs) producing Enterobacterales have gone up to 32%. This group includes E. coli, K. pneumoniae, K. oxytoca and P. mirabilis.1
ESBLs are β-lactamases capable of conferring resistance to β-lactam antibiotics such as penicillins, first, second and third generation cephalosporins and aztreonam (but not cephamycins or carbapenems) (Table 1). A key characteristic is that these enzymes hydrolyze the antibiotics but are inhibited by β -lactamase inhibitors such as clavulanic acid, tazobactam and sulbactam. Thus, diagnostic assays utilize this key characteristic to develop tools to screen for ESBL producers as discussed below.1-3
Figure 1. Disk diffusion test for ESBL detection. (A) A >5mm difference between the cefotaxime (CTX) and cefotaxime/clavulanic acid (CTX/CLA) disks, and ceftazidime (CAZ) and ceftazidime/clavulanic acid (CAZ/CLA) disks suggest a ESBL producer (top). (B) A <5 mm difference between CTX and CTX/CLA disks, and CAZ and CAZ/CLA does not suggest an ESBL-producer.
The genes encoding ESBLs are found on plasmids which enable rapid and easy transfer between Enterobacterales and some non-Enterobacterales as well. TEM-1, one of the first plasmid encoded β-lactamase enzymes, was identified in E. coli. Another one, SHV1 was subsequently discovered in Klebsiella.2 These original β-lactamases were narrow spectrum, but mutations have led to enzymes with broad spectrum activity, hydrolyzing many of the commonly used antibiotics. Today, there are over 100 variations of these enzymes that have spread resistance worldwide. The most dominant ESBL today is CTX-M, an enzyme that originated from Kluyvera species. CTX-M encoded resistance has now been reported among Enterobacterales as well as P. aeruginosa and Acinetobacter sp.2 Other ESBL families include IRT, CMT, GES, PER, VEB, BEL, TLA, SFO, and OXY.4
Detection of ESBL producers
The most common method for ESBL screening is the disk diffusion assay with clavulanic acid and cefotaxime and/or ceftazidime also called the double disc synergy test5 (Figure 1). ESBL producers are resistant to cefotaxime and ceftazidime. However, presence of clavulanic acid recovers the activity of cefotaxime and ceftazidime making the organism susceptible. If the activity of either one of these 3rd generation cephalosporin is recovered by clavulanic acid, then the presence of an ESBL is confirmed. A positive ESBL interpretation is resulted when there is ≥5 mm increase in zone diameter for either agent tested in combination with clavulanate versus the zone diameter of the agent tested alone. A broth microdilution approach is also possible. A positive ESBL interpretation would be a ≥3 ‘2-fold’ concentration decreases in an MIC for either agent tested in combination with clavulanate versus the MIC of the agent tested alone. Clinical Laboratory and Standards Institute (CLSI) guidance does not require ESBL testing for Enterobacterales but testing is recommended for infection prevention or specific institutional practices. For reporting of cephalosporin results, if current breakpoints are used for one or more cephalosporins, it is advised that the MICs are reported per usual. However, if obsolete cephalosporin breakpoints are used, then all penicillins, cephalosporins and aztreonam should be reported as resistant.6 It should be noted that there may be trivial differences between CLSI and European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines and it is up to the individual institution to decide which guidelines to follow.
Table 1. Breakdown of the different generations of cephalosporins.
Other phenotypic based methods to detect for ESBLs include commercially available testing systems that have built in phenotypic ESBL screening. Performance varies depending on the manufacturer and ranges from 84-99% and 52-78% for sensitivity and specificity, respectively.7 Other commercially available assays include the colorimetric tests such as the Rapid ESBL Screen Kit (Rosco Diagnostica) that detects ESBL producers without differentiating between the various enzymes.5,8 This test has sensitivity of >90% when tested with cultured isolates or various specimens (blood, urine or respiratory) but variable specificity. There is also a lateral flow test (NG-Test CTX-M MULTI assay, NG Biotech, Guipry, France) developed to detect for CTX-M enzymes with reported sensitivity and specificity of >98%.9
Advancements in molecular testing have included ESBL genes as targets on commercially available diagnostic panels. As CTX-M is the most common and wide-spread ESBL gene, commercial, FDA-approved platforms including blood culture identification panels and pneumonia panels include the CTX-M marker as a target. Sensitivity ranging from 85-95% have been reported with variable specificity.10-12 Recently, the Acuitas AMR gene panel became the first FDA-cleared diagnostic test that includes a wide panel of 28 AMR markers including ESBL-related family of genes such as TEM and SHV with reported positive predictive agreement of 98.5% and 100%, respectively.13
Overall, there are various methods to detect for ESBL producers and detection for ESBL producers may not be a straightforward matter as there are many ESBL families of genes and in general, antibiotic resistance mechanisms in gram negative organisms are heterogeneous. However, given the rise in antimicrobial resistance, identification of ESBL producers is vital both in treatment of patients as well as surveillance.
REFERENCES
1. CDC. 2022. Special report – Covid-19 U.S. Impact on antimicrobioal resistance.
2. Castanheira M, Simner PJ, Bradford PA.2021. Extended-spectrum beta-lactamases: an update on their characteristics, epidemiology and detection. JAC Antimicrob Resist 3:dlab092.
4. Castanheira M, Simner PJ, Bradford PA.2021. Extended-spectrum β-lactamases: an update on their characteristics, epidemiology and detection. JAC Antimicrob Resist 3:dlab092.
5. Dortet L, Poirel L, Nordmann P.2015. Rapid detection of ESBL-producing Enterobacteriaceae in blood cultures. Emerg Infect Dis 21:504-7.
6. Fay D, Oldfather JE.1979. Standardization of direct susceptibility test for blood cultures. J Clin Microbiol 9:347-50.
7. Wiegand I, Geiss HK, Mack D, Stürenburg E, Seifert H.2007. Detection of extended-spectrum beta-lactamases among Enterobacteriaceae by use of semiautomated microbiology systems and manual detection procedures. J Clin Microbiol 45:1167-74.
8. Rood IGH, Li Q.2017. Review: Molecular detection of extended spectrum-beta-lactamase- and carbapenemase-producing Enterobacteriaceae in a clinical setting. Diagn Microbiol Infect Dis 89:245-250.
9. Bernabeu S, Ratnam KC, Boutal H, Gonzalez C, Vogel A, Devilliers K, Plaisance M, Oueslati S, Malhotra-Kumar S, Dortet L, Fortineau N, Simon S, Volland H, Naas T.2020. A Lateral Flow Immunoassay for the Rapid Identification of CTX-M-Producing Enterobacterales from Culture Plates and Positive Blood Cultures. Diagnostics (Basel) 10.
10. Murphy CN, Fowler R, Balada-Llasat JM, Carroll A, Stone H, Akerele O, Buchan B, Windham S, Hopp A, Ronen S, Relich RF, Buckner R, Warren DA, Humphries R, Campeau S, Huse H, Chandrasekaran S, Leber A, Everhart K, Harrington A, Kwong C, Bonwit A, Dien Bard J, Naccache S, Zimmerman C, Jones B, Rindlisbacher C, Buccambuso M, Clark A, Rogatcheva M, Graue C, Bourzac KM.2020. Multicenter Evaluation of the BioFire FilmArray Pneumonia/Pneumonia Plus Panel for Detection and Quantification of Agents of Lower Respiratory Tract Infection. J Clin Microbiol 58.
11. Peri AM, Ling W, Furuya-Kanamori L, Harris PNA, Paterson DL.2022. Performance of BioFire Blood Culture Identification 2 Panel (BCID2) for the detection of bloodstream pathogens and their associated resistance markers: a systematic review and meta-analysis of diagnostic test accuracy studies. BMC Infect Dis 22:794.
12. Klein M, Bacher J, Barth S, Atrzadeh F, Siebenhaller K, Ferreira I, Beisken S, Posch AE, Carroll KC, Wunderink RG, Qi C, Wu F, Hardy DJ, Patel R, Sims MD.2021. Multicenter Evaluation of the Unyvero Platform for Testing Bronchoalveolar Lavage Fluid. J Clin Microbiol 59.
13. Simner PJ, Musser KA, Mitchell K, Wise MG, Lewis S, Yee R, Bergman Y, Good CE, Abdelhamed AM, Li H, Laseman EM, Sahm D, Pitzer K, Quan J, Walker GT, Jacobs MR, Rhoads DD.2022. Multicenter Evaluation of the Acuitas AMR Gene Panel for Detection of an Extended Panel of Antimicrobial Resistance Genes among Bacterial Isolates. J Clin Microbiol 60:e0209821.
-Athulaprabha Murthi PhD is currently a Fellow at the NYC Public Health Laboratory. She is interested in antibiotic resistance and hopes to work towards better diagnostic testing and surveillance methods for monitoring resistance. She also enjoys writing and teaching whenever opportunity presents.
-Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.
Working in Hematology, I have learned that things aren’t always black and white. With about 80-85% of our CBC’s autovalidating, it’s those other “problem child” specimens that can give us a challenge. When we get one of these tricky specimens, it’s time to put on our detective hats and investigate what is going on.
This patient was a 65-year-old female with Chronic Lymphocytic Leukemia (CLL). WBC and RBCs are counted on our analyzer by impedance, which sorts cells by size. When we ran this sample, we noticed a few things right away. See results below in Figure 1.
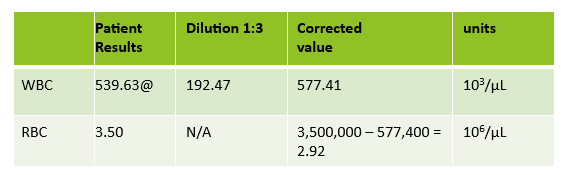
Figure 1. Original CBC results with Instrument Flags
The first thing I notice on this specimen is the @ next to the WBC. This indicates that the count is over linearity and was confirmed by dilution. The corrected WBC was 577 x 103/mL. See Figure 2.
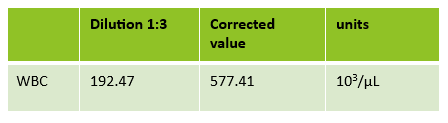
Figure 2. 1:3 dilution results for WBC. 192.47 x 3 = 577.41 x 103/μL
Extreme leukocytosis may interfere with the RBC, HGB, HCT and MCV determinations. The degree of RBC interference depends on the number and size of WBCs present. WBC and RBC are counted using impedance technology. In impedance counting, the RBC count is done first by passing the sample though the aperture in the RBC/platelet channel. This count is actually the sum of both RBC and WBC counts. Then, the RBCS are lysed and the WBCs are counted in the WBC channel. Normally, the WBC count has very little, if any, effect on the reported RBC count. Normal RBC counts are 4-6 million/μL. Normal WBC counts are a fraction of this, at about 5-10,000/μL. If the the RBC count is 3.50 x 106/μL and the analyzer includes 10,000 WBCs in the count, this only changes the RBC to 3.51 x 106/μL. (3,500,000 + 10,000 = 3,510,000). Because WBC counts are so much lower than RBC counts, even if a WBC count is 100,000, the effect on the RBC count is clinically insignificant. (3,500,000 + 100,000= 3,600,000 = 3.60 x 106/μL) However, in this patient, the WBC count was 577,000/μL. After reviewing the smear and confirming the WBC count with a WBC estimate, we corrected the RBC count, by subtracting the WBC from the RBC. As you can see in figure 3 below, the extreme leukocytosis did affect the RBC count.
Figure 3. Corrected RBC count. Subtract the WBC count from the RBC count. Corrected RBC (cRBC) = RBC (x 106/μL) – WBC (x 103/μL)
So, how does this affect the hematocrit? The next thing noticed right away is that the Hgb and Hct don’t follow the “rules of 3”. Now, we know that these rules really only hold true for normocytic, normochromic RBCS, but extreme leukocytosis can interfere with Hct determination. A Hgb of 9.2 g/dL and Hct 39.4% doesn’t look ‘right’. We have just corrected the RBC count, and now we need to ask ourselves how this can affect the Hct. The hematocrit is the packed cell volume, or the % of red blood cells per total volume of the sample. Since we now know that the RBC count is 2.92 x 106/μL, not 3.50 x 106/μL, we can correct the hematocrit. If you have a hematocrit centrifuge in your laboratory, a spun hematocrit can be used to determine the corrected hematocrit. After correcting the Hct, you must also correct the MCV using the following formula.
Corrected MCV (cMCV) = HCT(%) x 10/cRBC
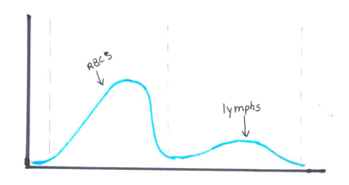
Another option for resolving interferences and correcting the Hct for extreme leukocytosis is using the clues that the RBC histogram gives us. We know the RBC count needed correcting, and we subtracted the WBC to get the corrected RBC. This sample had multiple flags. One of them was “Dimorphic population”. This indicates two populations of RBCs in the sample. Since we know a considerable number of WBCs were counted in the RBC chamber, this would account for the dimorphic population. A dimorphic population on histogram looks like what I call a ‘double humped camel’. In this case, the patient’s RBCs are the first, smaller population and the lymphocytes of this CLL patient are the 2nd larger population. See Figure 4.
Figure 4. Example of a dimorphic RBC histogram.
Another option for recalculating the MCV is using the information in the service tab of your analyzer. Note that the results from the service tab are not FDA approved, and therefore not directly reportable, so must be confirmed first. If using values from the service tab, the spun hematocrit and calculations can be used as a check. The service tab displays the MCV of these 2 populations. These are listed as the MCV of the small population, S-MCV, and the MCV of the large cell population, L-MCV. Using the small MCV (sMCV) value and the corrected RBC (cRBC), we can back calculate the Hct using the following formula.
Corrected Hct (cHct) (%) = (sMCV x cRBC)/10
For this sample:
S-MCV = 105.1
L-MCV= 215.4
(cHct) (%) = 105.1 x 2.92/10 = 30.7 %
Hgb is another parameter that may be affected by extreme leukocytosis. Turbidity may be present in the diluted and lysed sample when reading the Hgb. This sample did not give us a Hgb turbidity flag, but because of the high WBC, the Hgb was confirmed using a diluted sample. The sample was diluted 1:3 with the analyzer diluent. Results were multiplied by the dilution factor. Lastly, when performing Hgb corrections (and in this case, also the RBC corrections) you must also recalculate the MCH and MCHC using the corrected values. Figure 5 shows these corrected values.
MCH (pg)= (cHgb/cRBC) x 10
MCHC (g/dL) =(cHgb/cHct) x 100
Figure 5. Corrected CBC results
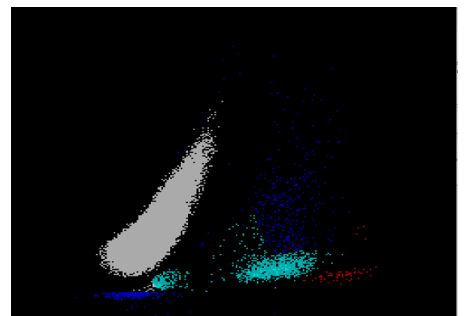
We can breathe a sigh of relief that we finally have accurate and reliable results for the CBC. But what about the differential? This big ugly grey mess seen in Figure 6 on the differential scattergram indicates a very abnormal scattergram. This is telling us that there is no separation between the types of cells. There were multiple flags for WBC abnormal scattergram, leukocytosis, lymphocytosis, and a flag for dimorphic RBC populations. These flags are all telling us not to accept the instrument results. In these cases, we want to review the smear, do a WBC estimate, and perform a manual differential, examining the differential carefully to look for any abnormalities. The differential had many lymphocytes and smudge cells. An albumin smear was made to resolve the smudge cells and a manual differential was performed.
Figure 6. WDF Scattergram
I’ll admit that this type of specimen is not something we encounter every day (thankfully). But I thought it a very interesting example of a spurious results on many levels. These challenges are some of my favorite things about working in Hematology. Using autovalidation is a great tool in the laboratory to help workflow. With about 85% of specimens autovalidating, this allows us to spend time on these tricky specimens. And this tricky specimen was an epic one! We had CBCs on this patient several days in a row. Unfortunately, some of her results were simply repeated and reported. Some WBC results over linearity were reported without dilution. Other parameters were not corrected. This gives inconsistent and confusing results to the physicians and is not beneficial to the patient. Because of the inconsistencies, we issued a couple corrected reports which can be very time consuming. Sometimes we may not have the answers and can’t resolve a problem. If a specimen cannot be resolved, it is always better to report what you can and use ‘not reported’ or ‘not measured’ for any results that are not available. It’s better to report the good results that you have than to report junk that physicians can’t rely on. I often say that simply repeating a sample and reporting results if they match is not sufficient. We need to investigate spurious results so that we may report the best quality results possible for every patient.
References
Gulati G, Uppal G, Gong J. Unreliable Automated Complete Blood Count Results: Causes, Recognition, and Resolution. Ann Lab Med. 2022 Sep 1;42(5):515-530. doi: 10.3343/alm.2022.42.5.515. PMID: 35470271; PMCID: PMC9057813.
Sysmex USA. XN-Series Flagging Interpretation Guide. Document Number: 1166-LSS, Rev. 6, March 2021
Zandcki, M. et al. Spurious counts and spurious results on haematology analysers: a review. Part II: white blood cells, red blood cells, haemoglobin, red cell indicies and reticulocytes. International Journal of Laboratory Hematology. 09January 2007.
-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
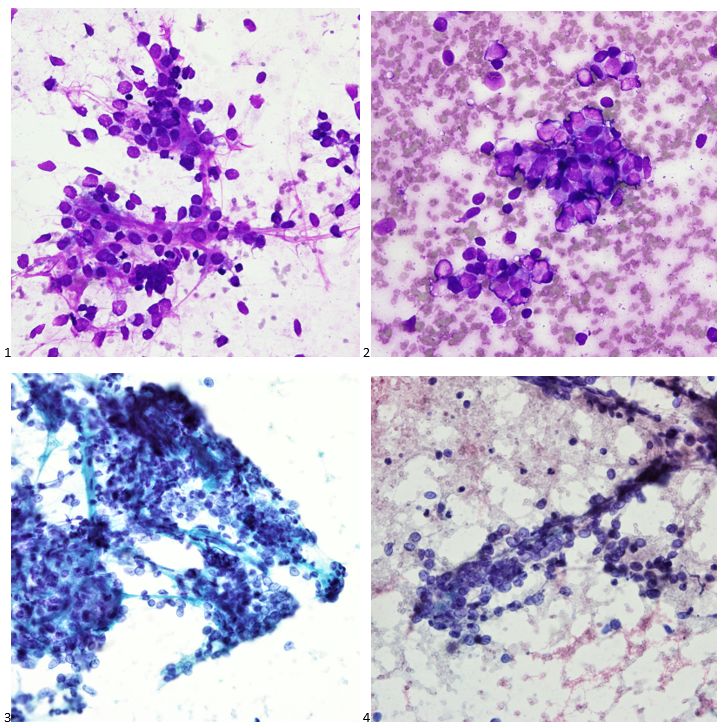
A 36 year old male was referred to gastroenterology after presenting to the emergency room for hematemesis and severe fatigue. He was pale and tachycardic, and the CBC showed a hemoglobin of 4.5. An esophagastroduodenoscopy (EGD) at the time demonstrated erosive esophagitis with a visible vessel and was treated with a PPI. A repeat scope the following month no longer demonstrated a vessel but identified a 10 cm ulcerative gastric cardia mass at the GE junction. Forcep biopsies showed a gastric ulcer with granulation tissue, and the stains performed yielded results that were not consistent with carcinoma or lymphoma; however, the biopsy material was limited, and the patient was referred to our GI clinic for further workup.
The interventional gastroenterologist requested cytology be present for the patient’s endoscopic ultrasound to ensure an adequate specimen was obtained for a definitive diagnosis. During the rapid onsite evaluation (ROSE), we determined the Diff-Quik smear was adequate, and the pathologist could confidently suggest that tumor cells were present. We collected additional FNA passes in our cell block tube to run ancillary studies.
The following morning, all we could make of the case was that it was a poorly-differentiated malignant neoplasm with spindle and epithelioid features. The cytoplasm was minimal and fairly wispy while the nuclei were hypochromatic and fragile with nuclear grooves and nucleoli. On the Diff-Quik smears, the cytoplasm looked blue, which pointed us in the direction of possibly lymphoma or neuroendocrine, but the clustering made me favor neuroendocrine. With the pap-stained smears, were torn between carcinoma and a neuroendocrine tumor, maybe even an epithelioid GIST, albeit an odd location. And of course, there’s always the differential of melanoma, the great mimicker. Off to IHC we go!
When our immunostains were delivered later that afternoon, our pathologist came up to me and said, “I got it! I know what it is!” Ecstatic, I replied, “What is it? Lymphoma? Carcinoma? GIST? MELANOMA?” “No, it’s a WEIRDOMA! Nothing is staining positive. No epithelial markers, no definitive lymphoid markers… nothing. It’s a weird case. I have to run additional stains.”
Back to the drawing board and 20 additional recut sections later, more immunostains were ordered and a mixed profile led us down a more confusing path. The tumor cells show positive staining for vimentin, CD56, and CD10 (focal), and negative staining for AE1/AE3, Cam5.2, CK7, desmin, SMA, HHF35, CD34, CD117, DOG-1, S100, SOX-10, synaptophysin, SALL4, CD45, CD68, and CD21. Proliferative index by Ki-67 was approximately 35%. The morphology and immunoprofile of the tumor were highly unusual, suggesting a mesenchymal neoplasm, possibly a sarcoma.
The concurrent forcep biopsies demonstrated rare atypical cells that were difficult to classify due to the limited number of cells, the non-specific morphology, and the following non-specific immunophenotype: positive staining for CD99, partial positive staining for D2-40 and NSE, and focal or weak positive staining for Cam5.2, while negative for AE1/AE3, CK7, EMA, S100, CD31, desmin, PAX8, BCL2, and myogen. The biopsy tissue consisted of predominantly ulcerative tissue and a fragment of squamous mucosa with a lamina propria infiltrate of atypical cells with spindle and epithelioid morphology.
Due to the FNA cell block consisting of 80% tumor compared to the limited forcep biopsy tissue, we sent FFPE cell block sections for RNA fusion studies to help us further classify the tumor. An EWSR1::ERG (in-frame) rsa(22;21)(q12.2;q22.2) gene fusion was detected in the tissue sample, which has been reported in extraskeletal Ewing sarcoma.
Stomach, GE Junction, EUS-FNA Final Diagnosis: Ewing Sarcoma
Fortunately, the patient’s PET scan did not demonstrate any evidence of metastatic disease, and the patient along with his care team decided to pursue systemic therapy as these tumors tend to be chemosensitive. The need for radiation therapy will be reviewed depending on the tumor’s response to systemic therapy. A strange presentation, this visceral Ewing sarcoma, and a reason why immunostains and molecular profiling are so important to rendering a definitive diagnosis. In our study set files, however, it will forever be dubbed my favorite weirdoma.
-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
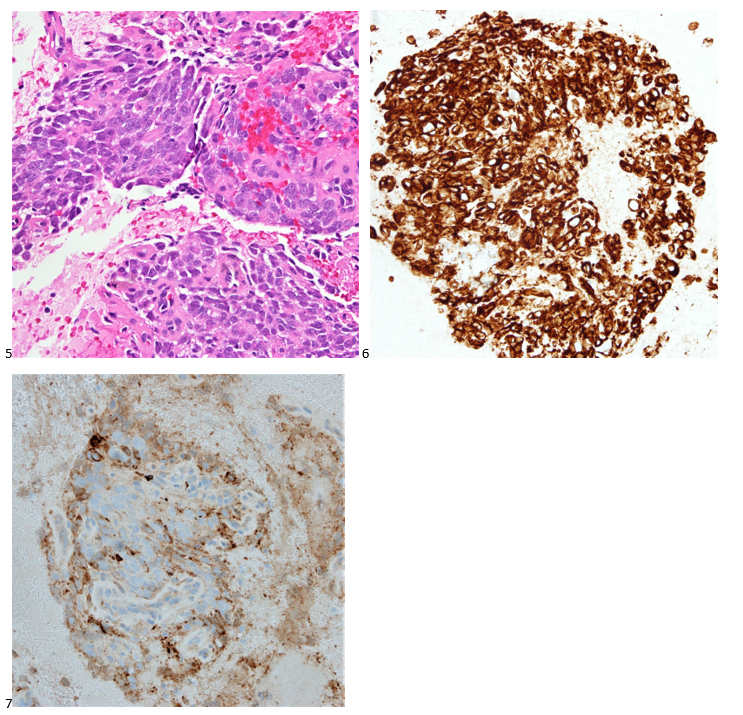
What is the data regarding the number of physicians- and pathologists-in-training who self-identify as Native American, Alaska Native, Hispanic/Latinx, or Native Hawaiian/Pacific Islander?
Among all resident physicians in ACGME-accredited and in combined specialty training programs on duty as of December 2022, there were a total of 154,231 individuals. The number of physicians in training in Pathology and its subspecialties totaled 2261 individuals. Looking at the demographic data as self-identified, the following data are striking:
Reference: Data was derived from Table 8 from Brotherton SE, Etzel SI, Graduate Medical Education, 2022-2023, Appendix to JAMA 2023: 330(10):988-1011.
Clearly there is an enormous gap in training of people from Indigenous and Hispanic/LatinX background in both medical training generally and in pathology specifically. The COVID19 pandemic disproportionately affected people from groups who are considered Under-Represented in Medicine (URIM), which include these groups, as well as individuals who self-identify as African American/Black, and who are also significantly under-represented in pathology and laboratory medicine.
What about the numbers for the laboratory professions?
With respect to laboratory professionals in practice and in training, I searched unsuccessfully for rigorous data to compare to the data available for physicians in training; however, even from the numbers available, under-representation is a challenge in the laboratory professions.
Please also note that Asian heritage comprises over 50 different language and ethnic groups. Within the United States, some of these groups are disproportionately affected by poverty and adverse social determinants of health. Therefore, for strategies to improve representation, future analyses should avoid simply lumping individuals into large buckets of self-identified demographic categories.
To address the adverse health impacts of the social determinants of health for patients from ALL demographic backgrounds, it will be essential to recruit actively from groups who have been both URIM and also from communities grappling with the impact of low income; lack of access to health insurance; lack of access to clean water; lack of access to sanitation services; lack of access to high, quality fresh food; residence in historically redlined neighborhoods that have been zoned for hazardous industries; lack of access to air-conditioning and shade from trees; and over-representation in hazardous work conditions.
Even without addressing these subtleties within ethnic/demographic groups, the data presented in the table convey the obvious fact that we have work to do to increase the numbers of trainees in Pathology (and, by extension, in the laboratory professions) from populations who have been historically under-represented in our training programs and workplaces. ASCP has a great opportunity for focused efforts by our Career Ambassadors, our Pathology Ambassadors, and all members to increase awareness of career opportunities in laboratory medicine and pathology. Recruitment is an important piece. Equally important is building and sustaining climates in our training programs and workplaces where people feel welcomed, recognized, invited to participate in transforming our practices to serve our patients better and considered for opportunities to advance and to be considered for leadership positions. Being hired is not enough. We all need to participate in continuous quality improvement, which means continuous engagement and active participation in decisions that will transform the ways we provide care so that we meet the needs of all our patients, now and in the future.
-Melissa P. Upton, MD. Past-President of ASCP and Chair of the ASCP Diversity, Equity, and Inclusion Committee; Emeritus Professor of Pathology, Department of Laboratory Medicine and Pathology, University of Washington, Seattle, WA.
A 74 year old male presented to UVMMC for a routine sputum culture at the adult cystic fibrosis (CF) clinic. At this visit, there were no pulmonary complaints, but chest imaging indicated scarring and atelectasis of the right upper lung and left mid lung. The imaging did not show signs of pulmonary infection.
The patient’s initial diagnosis of CF occurred at age 69 after a history of recurrent respiratory infections, bronchiectasis, and infertility. An elevated sweat chloride confirmed a CF diagnosis and subsequent genetic testing showed heterozygosity for 2 disease-causing CFTR mutations: p. Leu206Trp and p. Phe508del. Additional relevant medical history includes a history of smoking and ongoing pancreatic issues likely related to CF. The patient has been prescribed elexacaftor/texacaftor/ivacaftor which seems to be improving his pulmonary symptoms, as well as supplemental pancreatic enzymes which have moderately improved his pancreatic symptoms. Routine sputum cultures are often performed in CF patients to monitor treatment and disease progression, as well as detect any possible latent infections.6 A culture from this same patient in 2022 indicated an infection with Pseudomonas fluorescens, highlighting the importance of routine disease monitoring in CF patients.
Laboratory Workup
The sputum sample taken from the patient was routinely processed and planted to blood, chocolate, MacConkey, CNA, and Burkholderia cepacian agars. Growth from both the blood agar plate and the chocolate agar plate contained an organism with mucoid morphology, in addition to normal oropharyngeal flora. After subbing out these mucoid colonies, organism growth was observed on both a blood agar plate and a MacConkey medium plate. Growth from the MacConkey agar plate indicated the organism was a non-lactose fermenter, as observed in the un-pigmented colonies and the agar itself remaining a pink color.3 The mucoid organism was determined to be a mucoid strain of Pseudomonas aeruginosa from MALDI-ToF.
Figure 1. A blood agar plate. This plate shows growth of normal oropharyngeal flora, while also containing a bacterium of mucoid morphology. There are numerous colors, colony morphologies, and organisms present on the plate.Figure 2. A chocolate agar plate displaying mixed microbial growth. Some colonies are yellow in color with poorly defined margins, while other colonies are white with clearly defined margins. It was determined that the majority of the colonies present on this plate are normal oropharyngeal flora.Figure 3. Blood agar plate with mucoid morphological growth which was isolated from the plate shown in Figure 1.Figure 4. MacConkey medium growing bacteria with mucoid morphology. The bacteria itself remains an un-pigmented, brownish color while the agar itself had stayed pink. Both the colony color and agar color are indicative that the organism is not a lactose fermenter.3
Discussion
Cystic fibrosis (CF) is an autosomal recessive disease with the potential to affect multiple organ systems including the respiratory, digestive, and reproductive systems.7 The primary cause for this disease stems from mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene, of which more than two thousand different mutations have been described.1 In healthy individuals, this gene is responsible for the production of a protein that transports salts across different bodily tissues, yet mutated versions of this gene produce proteins that are absent or dysfunctional, and thus cannot promote salt transport and water movement as efficiently.2 The various mutations of the CFTR gene can result in numerous types of clinical presentations, but these mutations are most often observed to impact mucus viscosity with thick, sticky mucous along with chronic respiratory infections considered a hallmark of this disease.7 Further, decades of research have described additional manifestations of CF, including infertility, chronic sinusitis, and pancreatic damage, as well as an increased risk for dehydration.2
The most commonly performed diagnostic test for CF patients includes a sweat chloride test, for which a sweat chloride concentration above 60 mmol/L is indicative of a CF diagnosis and results directly from the loss of function of the CFTR proteins.1 Since the first descriptions of CF in 1935,1 newborn screening programs have been implemented with the hopes of catching potential cases early and improving prognoses. The newborn test screenings are often focused on the detection of immunoreactive trypsinogen in the blood, as the levels of this chemical are often elevated in patients with CF.1
Further, DNA analysis has proven to be an extremely useful tool in the diagnosis of CF patients, but these analyses are limited to the detection of only the most common mutations and can misdiagnose some of the rare variants of the disease.7 Additionally, because there is a wide range of disease-causing genotypes resulting in CF, some patients may exhibit a late onset of symptoms while still having two CFTR mutations, accounting for the increase of diagnoses made during adulthood.1 This would explain why the patient, in this case, may have been diagnosed so late in life; with two separate gene mutations, the patient may not have exhibited the classical symptoms of CF earlier in life.
Pseudomonas aeruginosa is a common pathogen found in CF patients and contributes significantly to patient morbidity and mortality.4P. aeruginosa, upon infection of the lung, promotes the accelerated decline of pulmonary function in CF patients and has been shown to exhibit significant resistance to both the innate immune system and antibiotics through the expression of specific virulence factors.5 Because CF patients are susceptible to chronic lung infections, repeat treatment with antibiotics has also been shown to promote adaptive mutations to P. aeruginosa, making this pathogen a particularly dangerous organism for CF patients.5 The versatility of the organism makes it capable of causing both acute and chronic infections, and the persistence of P. aeruginosa within CF patient airways into adulthood can be explained by the complex relationship between the organism’s pathogen traits and various host factors.4
Because P. aeruginosa has a reputation for being especially resistant to antibiotics, it is especially difficult to treat in CF patients who are routinely treated for chronic infections. The best treatment course would be to conduct an antibiotic resistance panel from the sputum culture sample to determine which of the available antibiotics might have the greatest treatment response against the bacteria.
References
1 De Boeck K. (2020). Cystic fibrosis in the year 2020: A disease with a new face. Acta paediatrica (Oslo, Norway : 1992), 109(5), 893–899. https://doi.org/10.1111/apa.15155
3 Jung, B., Hoilat, G.J., (2022, September) MacConkey Medium. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Accessed on September 26th, 2023, from: https://www.ncbi.nlm.nih.gov/books/NBK557394/
4 Jurado-Martín, I., Sainz-Mejías, M., & McClean, S. (2021). Pseudomonas aeruginosa: An Audacious Pathogen with an Adaptable Arsenal of Virulence Factors. International journal of molecular sciences, 22(6), 3128. https://doi.org/10.3390/ijms22063128
5 Malhotra, S., Hayes, D., Jr, & Wozniak, D. J. (2019). Cystic Fibrosis and Pseudomonas aeruginosa: the Host-Microbe Interface. Clinical microbiology reviews, 32(3), e00138-18. https://doi.org/10.1128/CMR.00138-18
6 National Guideline Alliance (UK). Cystic Fibrosis: Diagnosis and management. London: National Institute for Health and Care Excellence (NICE); 2017 Oct 25. (NICE Guideline, No. 78.) 9, Pulmonary monitoring, assessment and management. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535669/
7 Radlović N. (2012). Cystic fibrosis. Srpski arhiv za celokupno lekarstvo, 140(3-4), 244–249. Accessed on September 28th, 2023, from: https://pubmed.ncbi.nlm.nih.gov/22650116/
-Maggie King is a Masters Student in the Department of Pathology and Laboratory Medicine at the University of Vermont Larner College of Medicine.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
In the United States, victims of gunshot wounds represent a significant majority of all homicides (and a high proportion of suicides). There’s a propensity among other medical specialties to think of forensic pathologists as “bullet pullers,” just collecting the used projectiles and moving on to the next case. However, autopsies of multiple gunshot wound victims can be some of the most detailed examinations we perform. Even though the cause of death isn’t a mystery, thorough observation and documentation is crucial for other questions which may arise – was the victim immediately incapacitated? Did the shooter reload during the assault? How close to the victim were the shots fired? To address these questions, it’s first helpful to understand the basics of gunshot wounds.
Gunshot wounds can be penetrating (entering the body without exiting) or perforating (entering and exiting the body). Full body x-rays are taken in all gunshot wounds to identify retained projectiles, all of which must be recovered as evidence. It’s important to not use metal tools (like forceps or scissors) when removing a projectile, which may scratch metal and interfere with ballistics comparison.
Under typical circumstances, distinguishing entrance from exit wounds is straightforward. Classic entrance wounds are circular, as the bullet hasn’t yet been deformed, and there is a surrounding rim of abrasion where the edges of the bullet scrape against the skin. In contrast, exit wounds have a stellate or slit-like appearance, but the wound edges can typically be reassembled and are not abraded. As with any area of medicine, though, real life doesn’t always follow the rules. An entrance wound can be atypical if the bullet has passed through an ‘intermediary target’ before striking the victim (say a piece of furniture or a car door). If the area of exit is pressed against a firm object (even a tight pants waistband), the skin edges will be abraded (or “shored”). Sometimes, the entrance and exit truly cannot be distinguished – this is more likely with superimposed decomposition, insect activity, or superficial wounds.
Range of fire is another important feature to note and is the reason we always take photographs of a wound before cleaning the body. When a gun is fired, smoke, soot, and unburnt particles of gunpowder exit the barrel as well as the bullet. The smoke creates “fouling,” dark discoloration which easily wipes away and can be seen if the end of the barrel is within approximately one foot of the victim. Stippling, caused by unburnt grains of gunpowder, are actual abrasions and can be seen when the projectile fired within 18” of the victim. These are gross generalizations, though, and in each individual circumstance the weapon itself must be tested to identify the distances. If soot or gunpowder particles aren’t visible on the skin surface, they may have been deposited on the victim’s clothing. ‘‘Bullet wipe’ is slightly different from fouling, in that it is dirt and residue on the actual bullet which gets ‘wiped’ off around the entrance wound on clothing – so it doesn’t tell you range of fire, but it can be helpful to identify tricky entrance wounds.
Now, for some of the common misconceptions around gunshot wounds …
Can you tell the caliber of the gun from the size of the wound? The answer is an emphatic “no.” Much of the injury caused by a bullet comes from the temporary wound cavity created by dissipation of kinetic energy; so no matter the size of the bullet, tissue will stretch and distort around it.
Can you tell the order in which gunshot wounds were sustained? Most often, no. In some autopsies, the first wounds cause so much blood loss that the later wounds lack hemorrhage, but this is the exception rather than the rule.
Can I tell what position the victim was in when they were shot? Again, usually not. In isolation, an autopsy can only tell you the trajectory of the bullet through the body; to determine the position of the victim when they were shot requires knowledge of either where the gun was when it was fired or where the bullet landed–two factors which are often not available.
These are just a few of the complexities faced by a pathologist when working with gunshot wounds, and we haven’t even covered different types of ammunition or firearms. Stay tuned for more in the future!
This is an example of a classic entrance gunshot wound – nearly circular, with a thin rim of abraded (or scraped) skin.In contrast, this exit wound is slit shaped, and the wound edges can be neatly reapproximated.This entrance wound has stippling on the surrounding skin; occasionally gunpowder particles are still visible embedded in the abrasions.
-Alison Krywanczyk, MD, FASCP, is currently a Deputy Medical Examiner at the Cuyahoga County Medical Examiner’s Office.
A delivery truck is backing up to the loading dock of an empty warehouse. You are about to receive the first ever delivery from your supplier, and soon this new lab will be up and running. Are you going to unload the truck and stash the new chemicals in the corner? I hope not. Getting started with chemical management can be a little overwhelming, but it certainly can be done. Benjamin Franklin said, “By failing to prepare, you are preparing to fail.” It is best to start with a plan, preferably a chemical hygiene plan (CHP). So, let’s take a dip into a few important sections of the CHP.
The creation of a great CHP begins by listing the chemicals you have onsite and their associated hazards, and this will be your chemical inventory. Categorizing your chemicals by hazard type helps you to determine where and how they should be stored and handled once in the lab. It’s important to determine the compatibility of your chemicals before you place them on the shelves. Storing your inventory in alphabetical order may make it easier for staff to locate a particular item, but not all chemicals play nice with each other when they are neighbors. A bottle of chloric acid stored next to calcium hydroxide could be an accident waiting to happen. Make sure incompatible chemicals are kept apart, stored on separate shelves, or kept in separate bins. Do you store ethanol onsite? What about xylene? Both are flammable chemicals, so you may be able to store them in the same flammable safety cabinet. Separate corrosive storage cabinets may also be needed for your strong acids and bases.
Now that we have the chemicals separated, what do you do when it is time to use them? Your CHP should outline training and personal protective equipment (PPE) requirements for the different hazards as well as any engineering controls required to ensure work can be performed safely. Do you have a biological safety cabinet (BSC) in your lab? Be careful, not all BSCs can or should be used as a chemical fume hood (CFH). A CFH is designed with specialized filters and/or ducting to eliminate hazardous vapors that BSCs lack. Only a few classes of BSCs can provide protection from volatile chemical fumes. Check with the manufacturer to determine if it is safe to handle volatile chemicals in your BSC.
Next, you decide how you are going to dispose of the chemical waste you may generate in the lab. Never assume that liquid chemical waste is allowed to be poured down the drain. Some acids and bases that are poured down the drain will alter the pH of your wastewater. The Environmental Protection Agency (EPA) and the local wastewater authority will not be fans of that practice. Hazardous waste disposal requirements vary from state-to-state, so be sure to know the laws in your area for your place of business (see website: EPA Hazardous Waste Programs).
So now your chemicals stored properly, you know how to use them safely, but what is the plan when something unexpected happens? The accidental release of chemicals can be quite dangerous, and so can a poor response. A well written spill response procedure and periodic training can make clean-up a much less risky operation. The first and most important step is to correctly identify the chemical that spilled. Make sure staff know the location of your Safety Data Sheets (SDS), know how to access them, and that they are up to date. You may use an online database to access the SDS, and some services will even automatically update the SDSs to ensure you are viewing the most current version.
Make sure there is a spill kit in the lab that can effectively handle the accidental release of the different types of hazardous materials in your area. The kit should include the materials for a biohazardous spill as well. Ensure you have a well written procedure that describes the steps to safely and effectively clean up the spill. Your procedure should outline actions such as securing and surveying the site, donning the required PPE, laying down barriers to prevent spreading, and applying absorbents. Also include information about extraction of the clean-up material and proper disposal. Remember, the waste created from a chemical spill is considered a hazardous waste and must be treated as such. Absorbed chemical waste should be placed in a bag specially designated for hazardous waste (and segregated for offsite removal by your waste vendor.
The drafting of a CHP does take time and attention, but you cannot stop there. Your CHP is a living document that requires attention, and once it is created, you never want to let it go stale. It is important to keep your CHP fresh by updating it often. In fact, OSHA and most accrediting agencies require laboratories to review their CHP annually and assess its effectiveness. Keep staff knowledge about your CHP crisp. When staff know how to locate and use their CHP, they are more prepared to work safely with hazardous materials.
-Jason P. Nagy, PhD, MLS(ASCP)CM is a Lab Safety Coordinator for Sentara Healthcare, a hospital system with laboratories throughout Virginia and North Carolina. He is an experienced Technical Specialist with a background in biotechnology, molecular biology, clinical labs, and most recently, a focus in laboratory safety.
On May 11, 2023, the FDA’s Center for Biologics Evaluation and Research (CBER) issued guidance updating the blood donor history questionnaire (DHQ). Also known as the DHQ v4.0. The hope was that creating a gender-neutral questionnaire would increase the number of people eligible to donate, improving the nation’s blood supply.
After 3 months, has it made a difference?
The DHQ v4.0 is a series of questions asking potential donors about their lifestyle activities and travel to assess whether they are eligible to donate blood. The questionnaire is a risk-based model and is a critical step in ensuring the safety and potency of the nation’s blood supply.
As knowledge and understanding about disease increases along with the ongoing need to maintain an adequate blood supply, the FDA, in conjunction with the Association for the Advancement of Blood and Biotherapies (AABB), reviewed the restrictions or limitations on groups or individuals who may be allowed to donate with the goal of increasing the pool of eligible donors.
The DHQ v3.0 contains gender-specific questions impacting the eligibility of LGBTQ members. The new DHQ v4.0 was developed to be gender-neutral. There was concern that the new questions (especially the follow-up if any were answered yes) would be uncomfortable, but they were necessary to assess every potential donor the same.
“Some of the follow-up questions can seem to be a bit personal,” states Marvin Opulencia, Donor Operation Trainer at Inova Blood Donor Services (IBDS).
But Marvin thinks the change was a good thing because the questionnaire is no longer gender-specific and makes the process easier. “Some of my friends are members of the LGBTQ community, and now they are able to donate. I’m happy about that.”
Recognizing the difficulty and sensitivity inherent in the impacted topics, the FDA did not issue a deadline for implementation but has allowed blood donation centers to integrate the new guidance at their own pace. However, there were some blood donor centers that were ready to move forward with the recommendations. Their experience tells us that it is still too early to evaluate the effect of the change.
Nicholas Lilly, Interim Director of IBDS in Northern Virginia, believes we still don’t know the overall impact of the DHQ v4.0. “Inova Health System welcomes and supports initiatives improving the diversity, inclusiveness, and equity of our services. That’s why we were one of the first to implement the DHQ v4.0 in June. We serve the DMV area (D.C., Maryland, and Virginia), which is a highly diverse community, and so we saw the new guidance as a continuation of our vision and goals.”
With three months of data to evaluate, Director Lilly still doesn’t know what impact the change has on the blood supply. “Though we have received no negative feedback from our clients, we still haven’t seen a net increase in the number of donors. We have seen more non-binary people donate, but overall, there has not been a noticeable increase in donations. But it’s still early.”
It was expected that changing the Individual Donor Assessment to a more gender-neutral questionnaire would generate a bit of consternation and questions regarding whether it was in the nation’s best interest. However, so far, it was just one more step toward allowing everyone to make a difference.
Stated simply, Blood Saves Lives and is desperately needed. Now everyone has the opportunity to donate. Limitations or restrictions should be determined by science-backed non-judgmental research. That’s what the DHQ v4.0 is… that’s the difference it makes.
–Darryl Elzie is a Quality Consultant for Inova Blood Donor Services. He has been an ASCP Medical Technologist for over 25 years, performing CAP inspections for 15+ years. He has held the roles of laboratory generalist and chemistry senior technologist. He has a Master’s in Healthcare Administration from Ashford University, a Doctorate of Psychology from The University of the Rockies, and is a Certified Quality Auditor (ASQ). Inova Blood Donor Services is the largest hospital-based blood center in the nation. Dr. Elzie is also a Counselor and Life Coach at issueslifecoaching.com.
In television and movies, you’ll sometimes see a scene where the pathologist describes to a detective the specific dimensions of a knife used in an attack, all based on the autopsy findings. While this is no doubt extremely helpful to an investigation (and the limits of a 60-minute run time) it’s also impossible to provide this level of detail from an autopsy. Unfortunately the pervasiveness of such creative liberties in pop culture creates unrealistic expectations from juries, lawyers, and law enforcement, which we often need to gently correct. There are certain characteristics we can identify which may clarify what kind of blade was used, but conversely may not match the dimensions of the weapon at all.
While any object with a pointed or edged tip can be used to inflict sharp force injuries, we will focus on knives as the stereotypical ‘sharp force’ weapon. As a reminder, sharp force injuries have clean, neat edges and no tissue bridging in the wound depths. These are the features that are used to distinguish sharp force from lacerations, which are skin tears due to blunt force injury (see last month’s blog post for a refresher!). The most important first step for any instance of sharp force injury is to fully x-ray the body; this allows for identification of potential evidence to discover (such as a broken knife tip), and identifies potential sharp hazards for the prosector.
The first issue when interpreting sharp force injuries at autopsy is distortion of wounds by skin elasticity. Depending on the location and orientation of the wound, the edges may be pulled by tension along Langer’s lines. If this is the case, re- approximating the wound edges is needed before measuring for better accuracy. The ends of a stab wound may reflect whether a blade has one or two edges, depending on whether both ends are tapered (two-edged) or if one end is blunt and the other tapered (single-edged). The morphology isn’t always clear, though. Occasionally a double-edged blade will have a blunt-edged segment known as the “ricasso” just before the crossguard or handle. If the blade is fully inserted, the impression of the ricasso may make the wound appear to have two blunt edges.
The second difficulty faced is that knife wounds are rarely inflicted on a stationary body – there is typically (at least initially) a struggle involving motion of both the victim and the blade. This can result in wounds which are distorted from the dimensions of the weapon. These kinds of wounds also don’t necessarily imply that the person holding the knife was ‘torturing’ the victim – it just means that there was motion between the body and the blade. For example, a ‘dovetail’ or “V”-shaped wound can be created if the knife is inserted and removed at different angles – this could happen if either the victim is moving, if the assailant moves the angle of the knife, or both.
Another relatively frequent source of confusion is depth of wound relative to the length of the blade. All soft tissues are compressible, but certain parts of the body have a little more give. For example, the relatively soft abdominal pannus and viscera are easily compressed, whereas the chest is held in a rigid position by the rib cage. Therefore it’s very possible for a 5” blade to leave a wound 8” in depth if inflicted in a soft location like the abdomen. Additionally, if a blade isn’t inserted to the full length, the wound depth could also be shorter than the weapon.
One concerning trope on television is the immediate reconstruction of a crime based on autopsy findings. As one example, much emphasis is placed in the media on identifying ‘defensive wounds’. However, there is no way to tell at autopsy if a wound was sustained defensively or aggressively (and to be fair, even if the incident was caught on camera there could be differing interpretations). There are characteristics which are more commonly seen in ‘defensive’ wounds, such as locations on the hands and forearms as the victim attempts to block or grab the weapon. Hand wounds can also be seen on the assailant, though, as blood can make their hand slip onto the cutting blade during thrusts. Similarly, it is never possible to ascertain the “handedness” of an assailant from the wound pattern.
Serrated knives may leave a characteristic pattern of abrasions on the body but may leave no mark depending on the angle of the wound. So, if such marks are present, it’s distinctive of a serrated weapon – but if they’re absent, the weapon could be either a serrated or straight edged blade.
Contrary to what is shown on TV, there is no way to definitively ‘match’ one specific knife to a particular wound. The closest we could get would be finding a broken segment of the blade within the body – and even then, one must imagine there is more than one knife in the world that has a broken tip. While the world would be a much simpler place if such answers were possible, it’s our duty as scientists and physicians to be honest about the limitations of science and avoid speculation.
This is a stab wound inflicted by a knife with a single-edged blade, characterized by a squared-off, blunt end at the top of the photo and a tapered, “sharp” end at the bottom of the photo.This stab wound initially has very unclear morphology (on the left) due to tension placed on the wound by skin elasticity and nearby sutures. Once the wound is reapproximated (on the right), there are clearly two tapered edges which may be consistent with a double-edged blade.
-Alison Krywanczyk, MD, FASCP, is currently a Deputy Medical Examiner at the Cuyahoga County Medical Examiner’s Office.