Body identification is one of the core responsibilities of a forensic pathologist yet is also probably the most common one to be overlooked. Most of the deceased people who come to our office are visually identifiable, and the identity may already have been confirmed if they were transported to the hospital. In some situations, though, the body may be disfigured by fire, decomposition, injury, or there may only be partial remains recovered. In incidents with multiple fatalities, we need to be sure the correct remains are returned to the correct family. Particularly when foul play is involved, there may be intentional attempts to conceal the decedent’s identity or disguise them as another person.
There are two different levels of identification: “positive” identification (the gold standard) and “presumptive” identification.
The three generally accepted forms of “positive” identification are DNA comparison, fingerprint comparison, and radiograph comparison. While television shows have DNA “matches” coming back in the time it takes for a commercial break, DNA identification can pose challenges. A pre-existing specimen from the decedent or close family members is needed for comparison, which means you need to already have some suspicion of who they are. If they’ve been previously arrested or charged with a felony (the laws vary slightly by state), their DNA may have been uploaded to the Combined DNA Index System (CODIS), and a match may potentially be obtained blindly by uploading the decedent’s sample. By comparison, one can collect fingerprints from a decedent and submit them to the Automated Fingerprint Identification System (AFIS) for relatively rapid identification. Many people have been fingerprinted in their lifetime, whether for relatively minor arrests, employment, or background checks. However, there are still limitations. The hands (or at least fingertips) need to be intact, with printable skin. For mummified remains, the tissue can be rehydrated by soaking in sodium carbonate or sodium hydroxide to obtain legible prints. “Degloved” remains, where the skin has sloughed from the hands due to decomposition, can be fingerprinted by inserting one’s gloved hand into the sloughed skin.
Radiographs, like DNA, are limited by the need to have a pre-existing sample from the decedent (meaning you need to know who they might be). Radiographs are invaluable when trying to identify someone with no usable fingerprints, or no fingerprints on file. A variety of locations can be used for comparison, including the dentition, frontal sinuses, vertebral processes, healed fractures, or orthopedic implants. Serial numbers on implanted devices can also be traced back to the decedent, although not all implantable devices have such markings.
“Presumptive” identifications are based on many other common sense factors including context, visual identification, tattoos, belongings, and clothing. Depending on the context of the case, a presumptive identification may suffice. For a decomposed body in a secure apartment occupied by a single, elderly person the neighbors haven’t seen in days, monogrammed dentures within the mouth may be sufficient. But in a fire with three charred female victims, aged 20-25, it’s much more important to confirm the identifications by a positive method. As I mentioned earlier any situation involving foul play may provide motivation for to conceal a victim’s identity, and so all homicide victims must be positively identified. It’s often taken for granted that the tag on our patient’s toe is accurate, but we need to approach our autopsies with the same level of diligence a laboratorian has when evaluating the label on a blood tube. Knowing who your patient is, and who your sample comes from, is the first critical step for any pathologist.
The mummified remains of a young adult were found in an abandoned house; while the fingertips were initially too dessicated to yield fingerprints, rehydration revealed excellent ridge details. Fingerprints were then uploaded to AFIS, and the decedent was identified within an hour.For skeletal remains with intact teeth, dental radiographs of the remains can be used for identification; however, for edentulous patients, a different strategy must be used.
-Alison Krywanczyk, MD, FASCP, is currently a Deputy Medical Examiner at the Cuyahoga County Medical Examiner’s Office.
A 47 year old male presented to the emergency department with a two-week history of progressively worsening left-sided flank and abdominal pain with radiation to his back. He also endorsed associated nausea, vomiting, dizziness, lack of appetite, and a 1-month history of intermittent fever, chills, night sweats, cough, and chest pain. Patient history was also notable for travel throughout the Amazon basin in Peru and Colombia, then to Panama where he felt ill while hiking in the rainforest. He also had sustained injuries to his left flank and head while traveling.
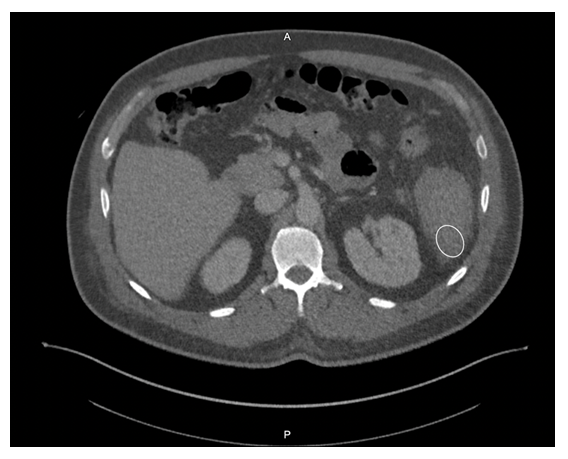
Given his symptomology, further evaluation and management were undertaken. CBC showed a drop in hemoglobin from 10.3 g/dL to 8.5 g/dL, and imaging revealed splenomegaly with a caudally located subcapsular hematoma (Figure 1). Small hemoperitoneum on the pelvis with small non-loculated fluid along the bilateral paracolic gutters was also observed. The patient received two units of packed red blood cells to stabilize his hemoglobin levels.
Laboratory Diagnosis
Malaria smears were ordered given his history travel and evidence of anemia. Plasmodium vivax was identified on thin smear at a parasitemia of 0.1%. The Infectious Disease service was consulted and the patient received IV artesunate followed by oral artemether/lumefantrine and was also started on primaquine for hypnozoite eradication as he was not G6PD deficient. The malaria-associated splenic rupture was well managed with conservative treatment, and no surgical intervention was needed.
Figure 1. Computer Tomography scan of the abdomen reveals a caudally located subcapsular hematoma (white circle).Figure 2. Peripheral blood smears (Giemsa stain, 1000x magnification, oil immersion) from the presented patient. A) An enlarged red blood cell with an irregular membrane containing a ring form (black arrowhead) and a mature trophozoite (white arrowhead) of P. vivax. B) An enlarged red blood cell with dot-like staining and a ring form, consistent with P. vivax (black arrowhead). C) P. vivax gametocyte (black arrowhead) and mature trophozoite (white arrowhead). Infected cells are enlarged and the mature trophozoite expands to nearly fill the red blood cell.
Discussion
Malaria is a severe and sometimes fatal tropical disease caused by Plasmodium sp.The World Health Organization (WHO) estimates 300-500 million humans suffer from malaria each year, of whom >1 million die.1 Five species of Plasmodium cause human malaria: P. falciparum, P. malariae, P. vivax, P. ovale, and P. knowlesi. Patients with malaria initially present with a combination of non-specific symptoms such as fever, chills, headache, and general malaise. Moreover, it can cause various complications, including severe anemia, neurologic defects, nephrotic syndrome, hepatosplenomegaly, and even splenic rupture.
Splenic rupture is an infrequent but life-threatening complication of malaria. Due to a paucity of reported cases, the incidence of pathological splenic rupture in natural vector-transmitted malaria is poorly defined. Additionally, cases of splenic rupture in the setting of malaria are likely to be underreported due to a lack of diagnostic methods, especially in endemic regions.2 One case series determined splenic rupture during malaria was fatal 22% of the collected cases, and it was likely to be the most frequent life-threatening issue of Plasmodium vivax infection reported worldwide.3 Similarly, P. vivax tends to cause more pronounced splenomegaly and a higher incidence of splenic rupture when compared to other Plasmodium species as noted in experimental and clinical studies.2.4 However, the underlying mechanism is incompletely established.
The cause of splenic rupture in malaria infections is thought to be a complication of the macroscopic consequences of different microscopic infiltrative phenomena. Specificities of clotting regulation in the spleen red pulp and acute spleen-specific pooling/unpooling of platelets may lead to increase in intrasplenic tension, making the spleen prone to rupture.3 Although malaria-related splenic rupture is essentially a ‘pathological rupture’ in the absence of overt trauma, minor trauma can also be a triggering event, which possibly contributed to the splenic rupture in this case.
Malaria patients with splenic rupture may present with abdominal pain, hypotension, tachycardia, nausea, and vomiting, which can be difficult to distinguish from signs and symptoms of malaria. Referred left shoulder pain (Kehr sign) caused by diaphragmatic irritation from peri-splenic effusion may also occur. The physical examination can show left upper quadrant or diffuse abdominal tenderness, abdominal rigidity or guarding, and splenomegaly. Radiological studies (i.e., ultrasound or CT scan) play a critical role in diagnosing malaria-associated splenic rupture, and the main findings may include splenic enlargement, splenic tear, subcapsular/intrasplenic hematoma, peri-splenic effusion, and hemoperitoneum. Non-radiological workup by contrast (e.g., decreased hemoglobin/hematocrit level) is generally non-specific.
Management of malaria-associated splenic rupture generally follows the same principles as traumatic injuries. Early diagnosis and appropriate management are essential for a favorable prognosis. It is suggested that conservative treatment can be considered in patients with stable hemodynamics. However, the risk of delayed hemorrhage still exists, which makes strict monitoring crucial. Some data suggest surgical intervention should be considered a first-line treatment if tears involve the splenic hilum.5 Although it may be challenging to decide on surgery versus conservative strategy in clinical practice, there are several definitive surgical indications including signs of peritonitis and unstable hemodynamic status despite aggressive resuscitation. Of note, splenectomy may increase the risk of severe infection caused by encapsulated bacteria and complicatedmalaria; therefore, spleen-preserving procedures should be attempted in selected patients, such as frequent travelers to malarious regions.6
References
Guerra, C.A., et al., The limits and intensity of Plasmodium falciparum transmission: implications for malaria control and elimination worldwide. PLoS Med, 2008. 5(2): p. e38.
Zingman, B.S. and B.L. Viner, Splenic complications in malaria: case report and review. Clin Infect Dis, 1993. 16(2): p. 223-32.
Imbert, P., C. Rapp, and PA Buffet, Pathological rupture of the spleen in malaria: analysis of 55 cases (1958-2008). Travel Med Infect Dis, 2009. 7(3): p. 147-59.
Schmidt, L.H., Plasmodium falciparum and Plasmodium vivax infections in the owl monkey (Aotus trivirgatus). I. The courses of untreated infections. Am J Trop Med Hyg, 1978. 27(4): p. 671-702.
Fuks, D., et al., Spontaneous splenic rupture during a febrile crisis of Plasmodium falciparum malaria. J Chir (Paris), 2005. 142(6): p. 403-5.
Jimenez, B.C., et al., Spontaneous splenic rupture due to Plasmodium vivax in a traveler: case report and review. J Travel Med, 2007. 14(3): p. 188-91.
-Bo Zhang, MD is an AP/CP resident at UT Southwestern Medical Center in Dallas, Texas. He is a first year resident interested in different aspects of surgical pathology.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
Recently our lab was asked by physicians to start reporting band counts of ≧10% as critical values. While we have always reported bands when a manual differential is performed, we have also heard for years about other labs that have stopped reporting bands. Mayo Clinic stopped reporting bands in the 1990’s- other nationally and internationally known hospitals and community hospitals alike have followed suit. CAP proficiency surveys for cell ID do not separate segmented neutrophils and band neutrophils for cell IDs. Our hematology analyzer reports Immature granulocytes (IG) and we have learned about the benefits of IG over the band count. Thus, when our pathologists asked us to add a critical value for bandemia, we wondered if we were moving ‘backwards’.
Bandemia is defined as elevated band neutrophils in the peripheral blood. Neutrophils are produced to help fight infection. With infection, there is an increase in WBCs being released by the bone marrow into the peripheral blood. Bands are considered mature neutrophils and can fight infection, and in an effort to keep up with demand, some of these infection fighting cells which are released are bands. However, we are reminded that this is a nonspecific clinical finding. Bands can be elevated in many situations including inflammation, autoimmune disease, metabolic abnormalities, pregnancy, and treatment with granulocyte colony stimulating factors. Band counts of ≧10% have been used clinically as an indicator of serious bacterial illness. A finding of bandemia can help providers decide what steps need to be taken in evaluation of a patient, and in conjunction with clinical findings, can help in making a differential diagnosis.
The trouble with bands is that they are notoriously difficult to measure accurately and precisely. Bands are somewhat controversial and there are conflicting opinions on the utility of bands. Should bands be reported or included with neutrophils? A left shift reflects bone marrow response to bacterial infection, and this has been quantified as band count or immature granulocyte count. Is the IG a better parameter than the band count?
If your Hematology analyzer reports the absolute neutrophil count (ANC) with an automated differential, this includes all mature neutrophils. The theory that supports this is that neutrophilic bands and segmented neutrophils are both mature cells, and both fight infection. A true left shift would therefore be the presence of immature granulocytes (metamyelocytes, myelocytes and promyelocytes). Yet, we also now have analyzers that offer a 6-part differential that includes the immature granulocyte (IG) count. And we know that an automated differential is based on counting thousands of cells, and a manual differential is based on counting 100 cells. So, which is better? We can theorize that the IG is a better indicator of left shift because the automated diff count looks at more cells than a 100-cell manual diff.
Let’s say that we have a patient with a WBC of 20 x 103/μL. Left shift is defined as an absolute IG count >0.1 x 103/μL. Automated diffs can count >30,000 cells depending on the WBC count. If the auto diff counts 32,000 cells and finds 1% IG, this means that the analyzer identified 320 IG. Absolute counts are calculated as % x the WBC, in this case 0.01 x 20,000=.2 x 103/μL. This meets the definition of a left shift. If we do a manual diff and count 100 cells and see 1 meta, the absolute IG would be .2 x 103/μL, again meeting the criteria for a left shift. However, if we did not see any metas or other IG on the manual diff, the absolute IG would be 0. Thus, performing a manual diff, the difference in seeing 1 cell or 0 would make the difference of reporting a suspected infection versus no suspicion of infection.
Table 1: Left shift? comparison of absolute IG when 1 or no IGs are seen on manual diff
With the advent of the IG count on automated differentials, labs have moved away from reporting bands. I have attended conferences and heard presentations about “banning” bands. A few years ago, I wrote a blog called “Beyond Bands: The Immature Granulocyte Count”, describing the benefits of using the IG count over bands in manual diffs. The above example would support “Ban the bands” arguments. Using the IG count from analyzers can take advantage of analyzing many more cells and give us statistically more precise values.
Results from auto diff can get to patients’ chart faster than a manual diff result, leading to faster treatment. To report bands, a manual differential must be done. We must wait for a slide to be made, dry, and a diff to be analyzed either under the microscope or on CellaVision. Bands are subjective, relying on technologist interpretation.
So, why are we suddenly being asked to make bandemia a critical value?
Physicians asked for this change and have cited cases where patients were seen in the emergency department (ED) and subsequently released, later to return, or experiencing negative outcomes. These patients had bands reported on differentials. Other area hospitals are reporting bands and have critical values for bandemia. Because patients often are seen at more than one area hospital, and doctors may have privileges at more than one of these, for consistency, this makes sense. But is also makes sense clinically.
Recent data has drawn renewed attention to bands as a reliable predictor of severity of patient condition. A number of research papers have been published that indicate that bands may indeed be important for patient care. A 2012 study investigated bandemia in patients with normal white blood cell counts. This cohort study found that patients with normal WBC counts with moderate (11%-18%) or high (>20%) band counts had increased odds of having positive blood cultures and in-hospital mortality. (Drees, 2012)
In 2019 a study showed that there was an “increasing risk for death with increasing bandemia, irrespective of leukocyte count. (Davis, 2019) A 2021 study done at Rhode Island Hospital showed a strong correlation between increasing percentages of bands on an initial emergency room CBC and the likelihood of significant positive blood cultures and in-hospital mortality. This was noted even at band levels below 10%. (Hseuh, 2021) S. Davis, MD, from the Department of Emergency Medicine, George Washington University School of Medicine and Health Sciences, in Washington, DC wrote that “While emergency physicians may find reassurance in a normal leukocyte count, the balance of evidence strongly suggests a more prudent approach would be to wait for the bands.” (S. Davis, 2021) In other words, wait for that manual differential. He stated that emergency room physicians get results from automated CBCs before the manual diff and do not see or are aware of any internal laboratory flags on these specimens. Physicians should be aware of reporting processes to avoid early discharge of otherwise well-appearing patients before band counts are reported. Last year, trends in bandemia and clinical trajectory among patients was reviewed in a retrospective chart review at George Washington University Hospital. They noted that “Bandemia clearance and trending, in conjunction with other existing clinical tools, may be of use as a marker of improvement in sepsis. Conversely, worsening bandemia may be predictive of a deteriorating clinical status and possibly a higher mortality.” They also noted that following trends of band levels in patients with sepsis or septic shock may help to predict a clinical course and overall prognosis. (Prasanna, 2022) Additionally, a band count greater than 10% is one of the American College of Chest Physicians/Society of Critical Care Medicine’s systemic inflammatory response syndrome (SIRS) criteria used to diagnose sepsis. (Chakraborty, 2022) These are just a few of the many articles that support a clinical utility of reporting the band count.
When we first learned that we would be reporting bandemia as a critical value, we realized that we would need to get everyone on the same page. We do most of our diffs on CellaVision, so, in theory, that should be easy, but, and a big but, is that bands are notoriously subjective. Different technologists may have been taught or have used their own definitions of bands. Variation can occur depending on slide quality, tech training, definition of bands used, and number of cells counted. So, how do we make this work? We need to be sure that all our technologists are reporting bands using the same criteria, so we are not reporting differing or confusing information to physicians. The concern lies in a physician making a significant clinical decision based on apparent changes in band counts that are not real but only reflect predictable statistical factors and unpredictable technologist variability.
In our laboratory, we approached the implementation of this new critical value as an educational opportunity. Differentials that had been performed on our CellaVision were reviewed, and it was apparent that bands were not being categorized consistently among techs. (See Figure1) We started with reviewing the definition of bands with all technologists and writing updated detailed procedures that includes these definitions. We use CAP’s definition of bands, which is the definition used in most textbooks and references for over 60 years. (See Table 1) Many examples of both bands and segmented neutrophils were added to our reference library on CellaVision. These included textbook perfect bands and some that may be more subjective. These reference cells can be used by techs to compare cells when making decisions as to in which category they belong. It was also stressed to techs that they need to look at cells carefully, and in a view that is large enough to see both detail and differentiation.
Figure1. Cells reported as segmented neutrophils on Differential. How many bands do you see?Table 2. CAP Definition of bands vs segmented neutrophilsFigure 2. Are these bands or segmented neutrophils?
Patient samples that had bands reported were located on CellaVision and multiple slides were made from these samples to be used as competency slides. In developing the differential evaluation tool, Rumke’s data showed that for a differential with a reported 12% bands, a second differential would have to have greater than 23% bands or fewer than 3% bands before the difference could be considered statistically significant. But this can be significant to our patients and patient care. In this example, diffs with <10% bands would not indicate bandemia, and diffs over 10% would initiate a critical bandemia call. And this could happen on the same slide depending on who did the diff, or on sequential samples on the same patient over a short period of time. These competency slides were assigned to techs to collect statistics on the mean and SD of the bands reported on each slide. Retraining and coaching will be provided as necessary. Follow up competency slides will be assigned, and statistics will be recalculated. The goal is to decrease variability in our band counts and to show that we have done so. This ongoing quality project has involved writing procedures, offering continuing education, assigning and reviewing competency slides, coaching technologists and reviewing slides with them and calculating statistics. Our goal is consistency and reporting meaningful results to our physicians.
As we saw in the studies cited above, % bands and trends are both important when evaluating clinical correlations. The chart below shows examples of how this might affect patient care. If a patient on presenting at the ED had a 19% band count, this would be called as a critical, and the patient would be further evaluated, and depending on clinical symptoms and medical history would likely have blood cultures drawn and be admitted to the hospital. If a second tech did the diff and reported 5% bands, the patient may be sent home without further evaluation. On subsequent CBCs, we could be giving confusing results to the physician if we are not consistent in our reporting. With multiple techs doing differentials on different shifts, it could look like this patient is getting better,
getting worse, or it could look like the patient is responding to therapy, and then the next day they had a setback. While we understand that bands will probably always be somewhat subjective, we need to narrow this down. By adhering to one definition, our goal is to report consistent and accurate results.
Table 3. Various results on differentials on the same patient over the course of 3 days, showing technologist dependent results.
ED physicians are looking for an early marker that can be used to identify septic patients as early as possible. Bandemia may be used as this marker. We therefore need to be as objective as possible when reporting bands. “Ultimately the band count is only one factor amongst several others which will be used in assessing the patient’s clinical state and in determining any subsequent medical management. Yet, identifying bands is important, and emphasizes the key role that our laboratory professionals play in identifying causes for concern” Dr Edgar Alonsozana, Mercy Medical Center, Baltimore, Md.
I welcome your comments about how your laboratories report bands and if bandemia is a critical value in your facilities!
References
P.Joanne Combleet, Clinical utility of the band count, Clinics in Laboratory Medicine, 2002;22:101-136
Al-Gwaiz, Layla A. and H H Babay. “The Diagnostic Value of Absolute Neutrophil Count, Band Count and Morphologic Changes of Neutrophils in Predicting Bacterial Infections.” Medical Principles and Practice 16 (2007)
S. Davis, R. Shesser, K. Authelet, A. Pourmand. “Bandemia” without leukocytosis: A potential Emergency Department diagnostic pitfall. The American Journal of Emergency Medicine,Volume 37, Issue 10, 2019
Harada T, Harada Y, Morinaga K, Hirosawa T, Shimizu T. Bandemia as an Early Predictive Marker of Bacteremia: A Retrospective Cohort Study. Int J Environ Res Public Health. 2022 Feb 17;19(4):2275.
Christine DeFranco DO and Terrance McGovern DO MPH St. Joseph’s Regional Medical Center, Paterson, NJ. Isolated Bandemia: What Should We Do with It? Critical Care, Oct. 2016,
Harmening, Denise. Clinical hematology and Fundamentals of Hemostasis, 4th ed. 1997
Prasanna N, DelPrete B, Ho G, et al. The utility of bandemia in prognostication and prediction of mortality in sepsis. Journal of the Intensive Care Society. 2022;0(0).
Takayuki Honda, Takeshi Uehara, Go Matsumoto, Shinpei Arai, Mitsutoshi Sugano, Neutrophil left shift and white blood cell count as markers of bacterial infection,Clinica Chimica Acta, Volume 457, 2016
Drees M, Kanapathippillai N, Zubrow MT. Bandemia with normal white blood cell counts associated with infection. Am J Med. 2012 Nov;125(11):1124.e9-1124.e15.
Leon Hsueh, Janine Molino, Leonard Mermel,
Elevated bands as a predictor of bloodstream infection and in-hospital mortality,The American Journal of Emergency Medicine,2021
-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
A middle-aged patient with a complex past medical history presented to the Emergency Department with the primary complaints of shortness of breath and cough. The patient had recently been admitted for community-acquired pneumonia and discharged with antibiotics 10 days ago. However, the patient continued to have a dry cough, a fever of 102 degrees F, and shortness of breath. On the new admission, they were noted to be hypotensive and labs showed elevated WBC (14.7), lactate of 7.3, proBNP of 852, and procalcitonin of 4.62. Bacterial blood cultures showed no growth. A chest x-ray showed worsening left lower lobe consolidation with extension to the left upper lobe, compared to the x-ray at the previous admission. A bronchoscopy was done and bronchoalveolar lavage (BAL) was submitted for Gram stain, aerobic bacterial culture, and fungal culture. The Gram stain and bacterial culture were negative. However, the fluorochrome stain showed many large budding yeast forms, most suggestive of Blastomyces dermatitidis. Lung tissue sample culture (Image 1), Gram stain (Image 2) and histopathology (Image 3) confirmed the identification as Blastomyces dermatitidis. The patient was expired before the results were released. Gross images of lungs are shown in image 4.
Image 1. Fungal growth on the Sabouraud dextrose plate observed after 2 days. Image 2. Gram stain of left lower lobe of lung tissue sample demonstrating budding yeast. Image 3. GMS and H&E stains of left lower lobe of lung sections demonstrating budding yeast. Image 4. Gross pictures of lungs showing left lower lobe hepatization and miliary pattern consolidation in the right lung.
Discussion
Blastomyces dermatitidis is a dimorphic fungus found in soil and decaying wood. Often found in areas close to a water source such as a lake, river, or stream.1 The fungus is endemic to parts of the United States, including parts of the Appalachian Mountains, the Great Lakes, and the Ohio and Mississippi River Valley.1 Human infection occurs when airborne conidia are inhaled. Blastomycosis (aka Gilchrist’s disease) may cause a broad range of clinical presentations. The most affected organs are the lungs and the skin.2 Osseous, genitourinary, central nervous system (CNS), and disseminated blastomycosis can also be seen, but at a lower frequency.2 Unlike opportunistic fungal pathogens such as H. capsulatum, C. immitis, and C. neoformans, B. dermatitidis no more likely to cause disease in immunocompromised population compared to the non-immunocompromised populatin.3 However, the disease is more severe, with higher morbidity and mortality, and more likely to be disseminated in immunocompromised patients.3
Although growth of fungi took 2 days in our case, Blastomyces is a slow growing fungi in that mycelial forms mature in 14-21 days. In suspicious cases, cultures should be hold up to 8 weeks. Furthermore, Blastomyces should be cultured as soon as possible since it does not survive well in samples. Morphologically, Blastomyces colony appears as a mold, which is white, prickly, and cottony at 25-30 °C However, at 35-37 °C, the colony appears as a yeast, which is tan, wrinkled, and waxy. Microscopically, at 37 °C, Blastomyces appear as round to oval cells with refractile and thick cell walls and measure 8 – 15 uM in diameter. Each yeast cell produces only one, broad-based (4-5 uM), bud. At 25-30 °C, septate hyphae form with short or long conidiophores. Round to pear-shaped conidia attach to the apex, resembling lollipops (Image 5).4
Image 5. Spherical, oval, or pyriform conidia rising from aerial hyphae, mold phase.
History of recent travel to the endemic areas or already living in there usually triggers the suspicion with clinical findings. There are different auxiliary diagnostic modalities for B. dermatitidis including culture, cytology smear, histopathology, urine antigen test, serum antigen test, serum antibody test, and molecular techniques. Serum antibody test exhibits high degree of cross-reactivity with other endemic mycoses.5 Serum and urine antigen testing has a sensitivity of 89 % and specificity of 79 % and it is useful in diagnosis, monitoring treatment, and detecting recurrence.5,6,7 Direct visualization of the distinctive yeast form with broad-based budding on a cytology smear of respiratory secretions or tissue samples using fluorochrome stain is considered as presumptive diagnosis and enough for initiation of antifungal therapy. However, a negative result in smear cannot exclude the diagnosis due to lack of sensitivity. Polymerase chain reaction (PCR) based assays have been developed to detect B. dermatitidis.8 However, although they are promising, utility has not been confirmed and there are no FDA approved assays.8
Only histopathology and culture can provide a definitive diagnosis. Although H&E may be enough in selected cases, periodic acid-Schiff (PAS) and Grocott’s methenamine silver (GMS) stains are useful to highlight the yeast form in tissue sections. In culture, seeing the characteristic morphologic and microscopic appearance is very useful for diagnosis. However, confirmatory testing with chemiluminescent DNA probe may still be necessary.9
Depending on the severity and site of the infection fluconazole, itraconazole, voriconazole, or amphotericin B can be used in treatment.10
References
Castillo CG, Kauffman CA, Miceli MH. Blastomycosis. Infect Dis Clin North Am. 2016;30(1):247-264.
Mazi PB, Rauseo AM, Spec A. Blastomycosis. Infect Dis Clin North Am. 2021;35(2):515-530.
McBride JA, Gauthier GM, Klein BS. Clinical Manifestations and Treatment of Blastomycosis. Clin Chest Med. 2017;38(3):435-449.
Maresca B, Kobayashi GS. Dimorphism in Histoplasma capsulatum and Blastomyces dermatitidis. Contrib Microbiol. 2000;5:201-216.
Wheat LJ. Antigen detection, serology, and molecular diagnosis of invasive mycoses in the immunocompromised host. Transpl Infect Dis. 2006;8(3):128-139.
Mongkolrattanothai K, Peev M, Wheat LJ, Marcinak J. Urine antigen detection of blastomycosis in pediatric patients. Pediatr Infect Dis J. 2006;25(11):1076-1078.
Tarr M, Marcinak J, Mongkolrattanothai K, et al. Blastomyces antigen detection for monitoring progression of blastomycosis in a pregnant adolescent. Infect Dis Obstet Gynecol. 2007;2007:89059.
Bariola JR, Hage CA, Durkin M, et al. Detection of Blastomyces dermatitidis antigen in patients with newly diagnosed blastomycosis. Diagn Microbiol Infect Dis. 2011;69(2):187-191.
Saccente M, Woods GL. Clinical and laboratory update on blastomycosis. Clin Microbiol Rev. 2010;23(2):367-381.
Chapman SW, Dismukes WE, Proia LA, et al. Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(12):1801-1812.
-Kadir Isidan, MS, MD is a pathology resident at University of Chicago (NorthShore). His academic interests include gastrointestinal pathology and cytopathology.
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
When we enter the laboratory, we know of the dangers that can be encountered. Our training tells us there could be microbes and other potential pathogens in the samples we are about to analyze. We also learned how to protect ourselves; how our behavior while in the lab has consequences. We even know how to dress properly and what engineering controls we have at our disposal to keep us safe. We put on our personal protective equipment (PPE) before we start to work and remove it before leaving the lab. For some, these behaviors are automatic, actions that are done almost without even thinking. But is this the same for all who enter the lab? Do visitors who comes into the department know what they are really walking into or how to keep themselves safe in an environment that may be foreign to them? One common question asked by lab staff regarding visitors is “do they have to adhere to the lab safety policies and if so, why?”.
On a recent safety audit, I visited a lab that happened to be getting a new chemistry analyzer installed. I noticed the vendor team, which consisted of 5 individuals, were not wearing any PPE. There were backpacks, open water bottles, and cell phones sitting on the counters and floors. The new instrument was not hidden in a back corner of the lab far away from the daily work. It was close to the area where the lab process, spins, and runs patient samples. Members of the vendor team were lying on the floor and crawling around. How does that scene make you feel?
Vendors and service representatives are regular visitors in your lab. A laboratory can have a representative on site a dozen times before you even begin to use that piece of equipment. Once it is installed, you can bet you will see them multiple times for preventative maintenance and service calls. How does your lab welcome these guests? Do you let them in and have them get right to work? If they are there to repair an analyzer you are likely eager to have them get started, but do you ask them to wear a lab coat? Did they bring one of their own that was kept in their backpack? If so, do you think that coat is clean or was it used in a different lab, packed up, and brought to your lab? Vendor compliance is a safety issue for many labs because these visitors are not lab employees, yet they are in your department and may be putting themselves and your team at risk. Often vendors are seen with drinks in labs, using cell phones or touching instruments without gloves – behaviors lab folk are told not to follow. So why is it tolerated? It shouldn’t be, and you have the right to speak up and ask them to adhere to your lab policies.
What about other potential laboratory visitors? Do pathologists come in to look at a patient slide in Hematology? Do they just sit down at your bench and look at the slide without gloves or a lab coat? Is lab staff allowed to scan a smear without PPE? Probably not, and no one else should be allowed too either. The microscope has most likely been touched with dirty gloves, and no one else should touch the same scope without gloves. Even lab doorknobs are a consideration. Staff should wash hands before leaving the department. That means no one should use contaminated gloves to open the door.
Speaking up about these safety issues to lab visitors can feel uncomfortable. A conversation with a physician about safe practices in the lab can be daunting, but the cost of not speaking up can be high. Take the opportunity to show you care about visitors and want to keep them protected. Sometimes you know who is coming to the lab, and you feel confident they have been trained and will use the best safety practices. At other times, though, those guests may be unexpected and lacking in safety knowledge. Make sure to treat them with respect, give them the safety training and tools they need so they can leave both happy and healthy.
-Jason P. Nagy, PhD, MLS(ASCP)CM is a Lab Safety Coordinator for Sentara Healthcare, a hospital system with laboratories throughout Virginia and North Carolina. He is an experienced Technical Specialist with a background in biotechnology, molecular biology, clinical labs, and most recently, a focus in laboratory safety.