Case Description
A 47 year old male presented to the emergency department with a two-week history of progressively worsening left-sided flank and abdominal pain with radiation to his back. He also endorsed associated nausea, vomiting, dizziness, lack of appetite, and a 1-month history of intermittent fever, chills, night sweats, cough, and chest pain. Patient history was also notable for travel throughout the Amazon basin in Peru and Colombia, then to Panama where he felt ill while hiking in the rainforest. He also had sustained injuries to his left flank and head while traveling.
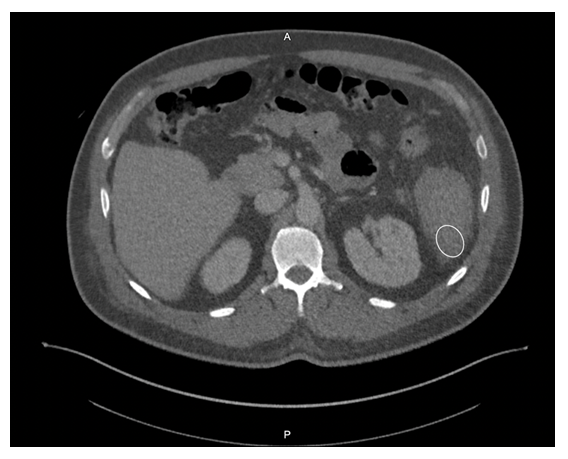
Given his symptomology, further evaluation and management were undertaken. CBC showed a drop in hemoglobin from 10.3 g/dL to 8.5 g/dL, and imaging revealed splenomegaly with a caudally located subcapsular hematoma (Figure 1). Small hemoperitoneum on the pelvis with small non-loculated fluid along the bilateral paracolic gutters was also observed. The patient received two units of packed red blood cells to stabilize his hemoglobin levels.
Laboratory Diagnosis
Malaria smears were ordered given his history travel and evidence of anemia. Plasmodium vivax was identified on thin smear at a parasitemia of 0.1%. The Infectious Disease service was consulted and the patient received IV artesunate followed by oral artemether/lumefantrine and was also started on primaquine for hypnozoite eradication as he was not G6PD deficient. The malaria-associated splenic rupture was well managed with conservative treatment, and no surgical intervention was needed.

Discussion
Malaria is a severe and sometimes fatal tropical disease caused by Plasmodium sp. The World Health Organization (WHO) estimates 300-500 million humans suffer from malaria each year, of whom >1 million die.1 Five species of Plasmodium cause human malaria: P. falciparum, P. malariae, P. vivax, P. ovale, and P. knowlesi. Patients with malaria initially present with a combination of non-specific symptoms such as fever, chills, headache, and general malaise. Moreover, it can cause various complications, including severe anemia, neurologic defects, nephrotic syndrome, hepatosplenomegaly, and even splenic rupture.
Splenic rupture is an infrequent but life-threatening complication of malaria. Due to a paucity of reported cases, the incidence of pathological splenic rupture in natural vector-transmitted malaria is poorly defined. Additionally, cases of splenic rupture in the setting of malaria are likely to be underreported due to a lack of diagnostic methods, especially in endemic regions.2 One case series determined splenic rupture during malaria was fatal 22% of the collected cases, and it was likely to be the most frequent life-threatening issue of Plasmodium vivax infection reported worldwide.3 Similarly, P. vivax tends to cause more pronounced splenomegaly and a higher incidence of splenic rupture when compared to other Plasmodium species as noted in experimental and clinical studies.2.4 However, the underlying mechanism is incompletely established.
The cause of splenic rupture in malaria infections is thought to be a complication of the macroscopic consequences of different microscopic infiltrative phenomena. Specificities of clotting regulation in the spleen red pulp and acute spleen-specific pooling/unpooling of platelets may lead to increase in intrasplenic tension, making the spleen prone to rupture.3 Although malaria-related splenic rupture is essentially a ‘pathological rupture’ in the absence of overt trauma, minor trauma can also be a triggering event, which possibly contributed to the splenic rupture in this case.
Malaria patients with splenic rupture may present with abdominal pain, hypotension, tachycardia, nausea, and vomiting, which can be difficult to distinguish from signs and symptoms of malaria. Referred left shoulder pain (Kehr sign) caused by diaphragmatic irritation from peri-splenic effusion may also occur. The physical examination can show left upper quadrant or diffuse abdominal tenderness, abdominal rigidity or guarding, and splenomegaly. Radiological studies (i.e., ultrasound or CT scan) play a critical role in diagnosing malaria-associated splenic rupture, and the main findings may include splenic enlargement, splenic tear, subcapsular/intrasplenic hematoma, peri-splenic effusion, and hemoperitoneum. Non-radiological workup by contrast (e.g., decreased hemoglobin/hematocrit level) is generally non-specific.
Management of malaria-associated splenic rupture generally follows the same principles as traumatic injuries. Early diagnosis and appropriate management are essential for a favorable prognosis. It is suggested that conservative treatment can be considered in patients with stable hemodynamics. However, the risk of delayed hemorrhage still exists, which makes strict monitoring crucial. Some data suggest surgical intervention should be considered a first-line treatment if tears involve the splenic hilum.5 Although it may be challenging to decide on surgery versus conservative strategy in clinical practice, there are several definitive surgical indications including signs of peritonitis and unstable hemodynamic status despite aggressive resuscitation. Of note, splenectomy may increase the risk of severe infection caused by encapsulated bacteria and complicated malaria; therefore, spleen-preserving procedures should be attempted in selected patients, such as frequent travelers to malarious regions.6
References
- Guerra, C.A., et al., The limits and intensity of Plasmodium falciparum transmission: implications for malaria control and elimination worldwide. PLoS Med, 2008. 5(2): p. e38.
- Zingman, B.S. and B.L. Viner, Splenic complications in malaria: case report and review. Clin Infect Dis, 1993. 16(2): p. 223-32.
- Imbert, P., C. Rapp, and PA Buffet, Pathological rupture of the spleen in malaria: analysis of 55 cases (1958-2008). Travel Med Infect Dis, 2009. 7(3): p. 147-59.
- Schmidt, L.H., Plasmodium falciparum and Plasmodium vivax infections in the owl monkey (Aotus trivirgatus). I. The courses of untreated infections. Am J Trop Med Hyg, 1978. 27(4): p. 671-702.
- Fuks, D., et al., Spontaneous splenic rupture during a febrile crisis of Plasmodium falciparum malaria. J Chir (Paris), 2005. 142(6): p. 403-5.
- Jimenez, B.C., et al., Spontaneous splenic rupture due to Plasmodium vivax in a traveler: case report and review. J Travel Med, 2007. 14(3): p. 188-91.
-Bo Zhang, MD is an AP/CP resident at UT Southwestern Medical Center in Dallas, Texas. He is a first year resident interested in different aspects of surgical pathology.

-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.

-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
