Case History
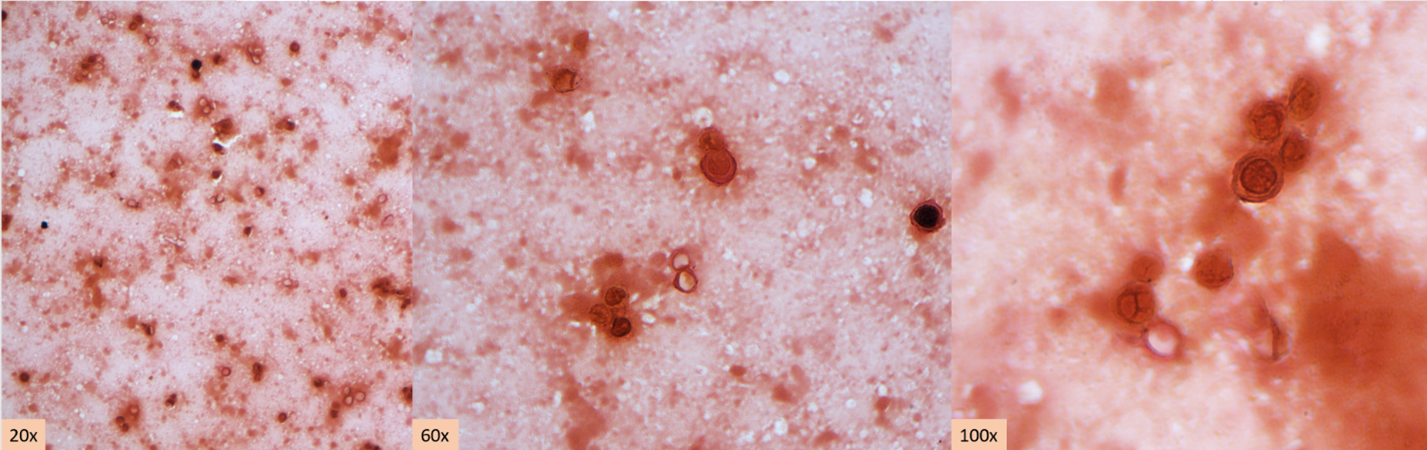
A middle-aged patient with a complex past medical history presented to the Emergency Department with the primary complaints of shortness of breath and cough. The patient had recently been admitted for community-acquired pneumonia and discharged with antibiotics 10 days ago. However, the patient continued to have a dry cough, a fever of 102 degrees F, and shortness of breath. On the new admission, they were noted to be hypotensive and labs showed elevated WBC (14.7), lactate of 7.3, proBNP of 852, and procalcitonin of 4.62. Bacterial blood cultures showed no growth. A chest x-ray showed worsening left lower lobe consolidation with extension to the left upper lobe, compared to the x-ray at the previous admission. A bronchoscopy was done and bronchoalveolar lavage (BAL) was submitted for Gram stain, aerobic bacterial culture, and fungal culture. The Gram stain and bacterial culture were negative. However, the fluorochrome stain showed many large budding yeast forms, most suggestive of Blastomyces dermatitidis. Lung tissue sample culture (Image 1), Gram stain (Image 2) and histopathology (Image 3) confirmed the identification as Blastomyces dermatitidis. The patient was expired before the results were released. Gross images of lungs are shown in image 4.



Discussion
Blastomyces dermatitidis is a dimorphic fungus found in soil and decaying wood. Often found in areas close to a water source such as a lake, river, or stream.1 The fungus is endemic to parts of the United States, including parts of the Appalachian Mountains, the Great Lakes, and the Ohio and Mississippi River Valley.1 Human infection occurs when airborne conidia are inhaled. Blastomycosis (aka Gilchrist’s disease) may cause a broad range of clinical presentations. The most affected organs are the lungs and the skin.2 Osseous, genitourinary, central nervous system (CNS), and disseminated blastomycosis can also be seen, but at a lower frequency.2 Unlike opportunistic fungal pathogens such as H. capsulatum, C. immitis, and C. neoformans, B. dermatitidis no more likely to cause disease in immunocompromised population compared to the non-immunocompromised populatin.3 However, the disease is more severe, with higher morbidity and mortality, and more likely to be disseminated in immunocompromised patients.3
Although growth of fungi took 2 days in our case, Blastomyces is a slow growing fungi in that mycelial forms mature in 14-21 days. In suspicious cases, cultures should be hold up to 8 weeks. Furthermore, Blastomyces should be cultured as soon as possible since it does not survive well in samples. Morphologically, Blastomyces colony appears as a mold, which is white, prickly, and cottony at 25-30 °C However, at 35-37 °C, the colony appears as a yeast, which is tan, wrinkled, and waxy. Microscopically, at 37 °C, Blastomyces appear as round to oval cells with refractile and thick cell walls and measure 8 – 15 uM in diameter. Each yeast cell produces only one, broad-based (4-5 uM), bud. At 25-30 °C, septate hyphae form with short or long conidiophores. Round to pear-shaped conidia attach to the apex, resembling lollipops (Image 5).4

History of recent travel to the endemic areas or already living in there usually triggers the suspicion with clinical findings. There are different auxiliary diagnostic modalities for B. dermatitidis including culture, cytology smear, histopathology, urine antigen test, serum antigen test, serum antibody test, and molecular techniques. Serum antibody test exhibits high degree of cross-reactivity with other endemic mycoses.5 Serum and urine antigen testing has a sensitivity of 89 % and specificity of 79 % and it is useful in diagnosis, monitoring treatment, and detecting recurrence.5,6,7 Direct visualization of the distinctive yeast form with broad-based budding on a cytology smear of respiratory secretions or tissue samples using fluorochrome stain is considered as presumptive diagnosis and enough for initiation of antifungal therapy. However, a negative result in smear cannot exclude the diagnosis due to lack of sensitivity. Polymerase chain reaction (PCR) based assays have been developed to detect B. dermatitidis.8 However, although they are promising, utility has not been confirmed and there are no FDA approved assays.8
Only histopathology and culture can provide a definitive diagnosis. Although H&E may be enough in selected cases, periodic acid-Schiff (PAS) and Grocott’s methenamine silver (GMS) stains are useful to highlight the yeast form in tissue sections. In culture, seeing the characteristic morphologic and microscopic appearance is very useful for diagnosis. However, confirmatory testing with chemiluminescent DNA probe may still be necessary.9
Depending on the severity and site of the infection fluconazole, itraconazole, voriconazole, or amphotericin B can be used in treatment.10
References
- Castillo CG, Kauffman CA, Miceli MH. Blastomycosis. Infect Dis Clin North Am. 2016;30(1):247-264.
- Mazi PB, Rauseo AM, Spec A. Blastomycosis. Infect Dis Clin North Am. 2021;35(2):515-530.
- McBride JA, Gauthier GM, Klein BS. Clinical Manifestations and Treatment of Blastomycosis. Clin Chest Med. 2017;38(3):435-449.
- Maresca B, Kobayashi GS. Dimorphism in Histoplasma capsulatum and Blastomyces dermatitidis. Contrib Microbiol. 2000;5:201-216.
- Wheat LJ. Antigen detection, serology, and molecular diagnosis of invasive mycoses in the immunocompromised host. Transpl Infect Dis. 2006;8(3):128-139.
- Mongkolrattanothai K, Peev M, Wheat LJ, Marcinak J. Urine antigen detection of blastomycosis in pediatric patients. Pediatr Infect Dis J. 2006;25(11):1076-1078.
- Tarr M, Marcinak J, Mongkolrattanothai K, et al. Blastomyces antigen detection for monitoring progression of blastomycosis in a pregnant adolescent. Infect Dis Obstet Gynecol. 2007;2007:89059.
- Bariola JR, Hage CA, Durkin M, et al. Detection of Blastomyces dermatitidis antigen in patients with newly diagnosed blastomycosis. Diagn Microbiol Infect Dis. 2011;69(2):187-191.
- Saccente M, Woods GL. Clinical and laboratory update on blastomycosis. Clin Microbiol Rev. 2010;23(2):367-381.
- Chapman SW, Dismukes WE, Proia LA, et al. Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(12):1801-1812.

-Kadir Isidan, MS, MD is a pathology resident at University of Chicago (NorthShore). His academic interests include gastrointestinal pathology and cytopathology.

-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
