A 62 year old male with a past medical history of CAD, CABG x 4, HTN, DMII, OSA on CPAP, and GERD was admitted for acute onset of chest pressure that radiated to his back. He also complained of nausea, vomiting. He had a similar episode of pain two weeks ago which resolved with nitroglycerin. The patient was found to have Type 1A aortic dissection on CTA. Decision was made to proceed to the OR emergently. Status post the operation, he continued to have hemodynamic instability and evidence of pneumonia. He had been intermittently febrile with leukocytosis (WBC=12.66). Blood cultures were drawn and were positive for gram negative bacilli in one bottle.
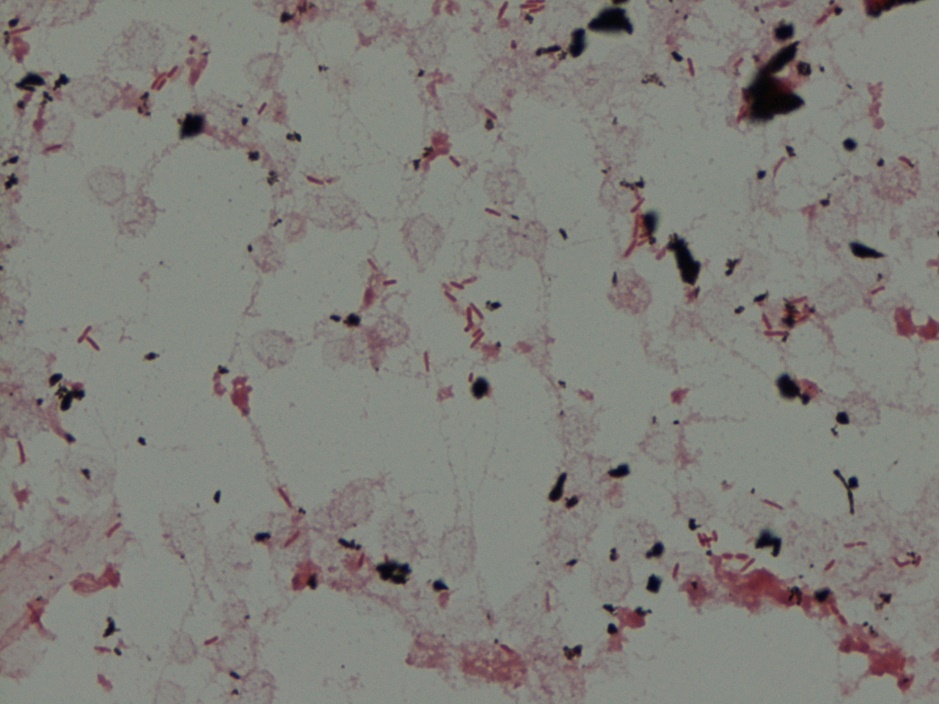
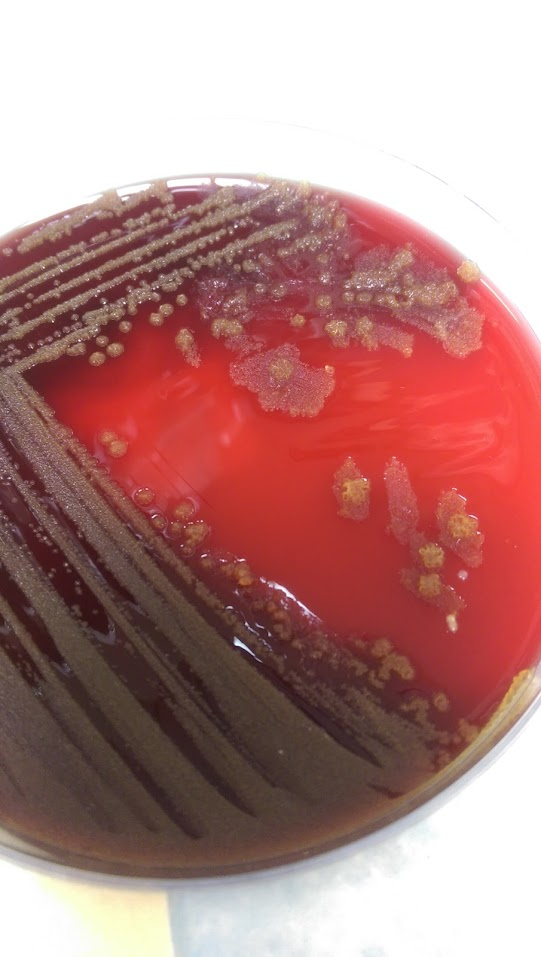
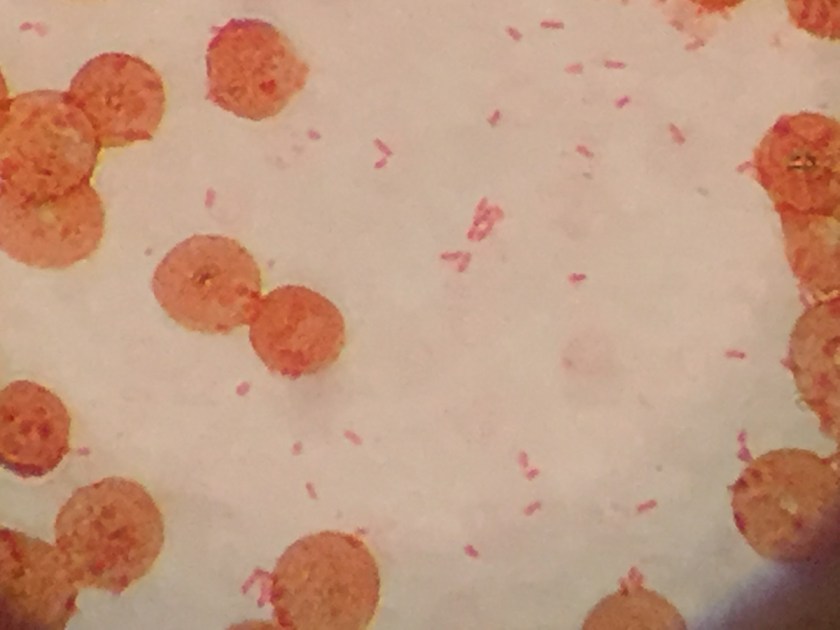
Gram stain demonstrating Gram-negative rods.Blood agar plate with dry, yellow colonies.
Identification:
Pseudomonas luteola was identified on the MALDI-TOF.
P. luteola was originally identified as Chryseomonas, but later changed to be a part of the Pseudomonas family. It is an opportunistic pathogen found in damp environments. It is a gram negative rod of 0.8 μm to 2.5 μm and is a motileaerobe. Its motility is created by multitrichous flagella. Colonies produce a yellow-orange pigment. P. luteola can be differentiated from most other motile yellow-pigmented nonfermenters by a negative oxidase reaction and from the Enterobacteriaceae by its strict aerobic growth. Optimal temperature for growth is 30°C, although it can grow at 42°C and not at 5°C. It grows best on heart infusion agar supplemented with 5% horse blood, but is also able to grow on TSA, Nutrient Agar, MacConkey or CASA Agar. The pathogenic form of P. luteola is a saprophyte and it can cause septicemia, peritonitis, endocarditis in patients with health disorders or with indwelling devices, and meningitis. Most strains are susceptible to broad-spectrum antibiotics, such as cephalosporins and ciprofloxacin.
Based on the history, the clinical team was unsure if it was a false positive/contaminant or truly a pathogen. The patient did have grafts and bioprosthetic material and due to the virulence of Pseudomonas, they decided to treat with cefepime and remove the central line. The patient clinically improved after removal of the line, which favored a line infection.
-Mustafa Mohammed, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
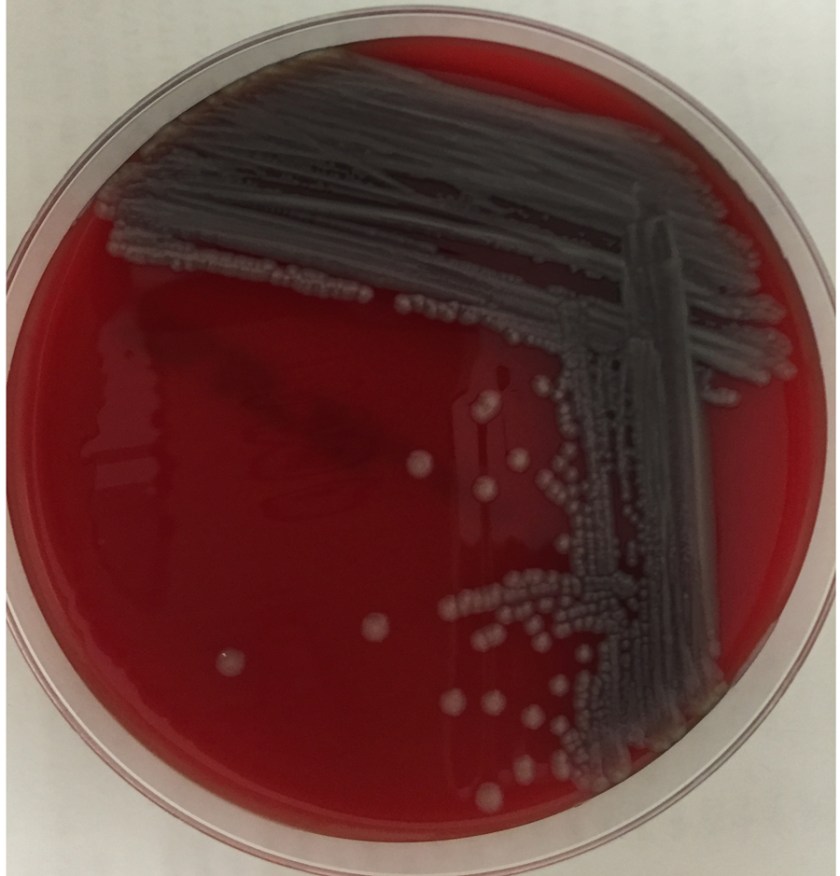
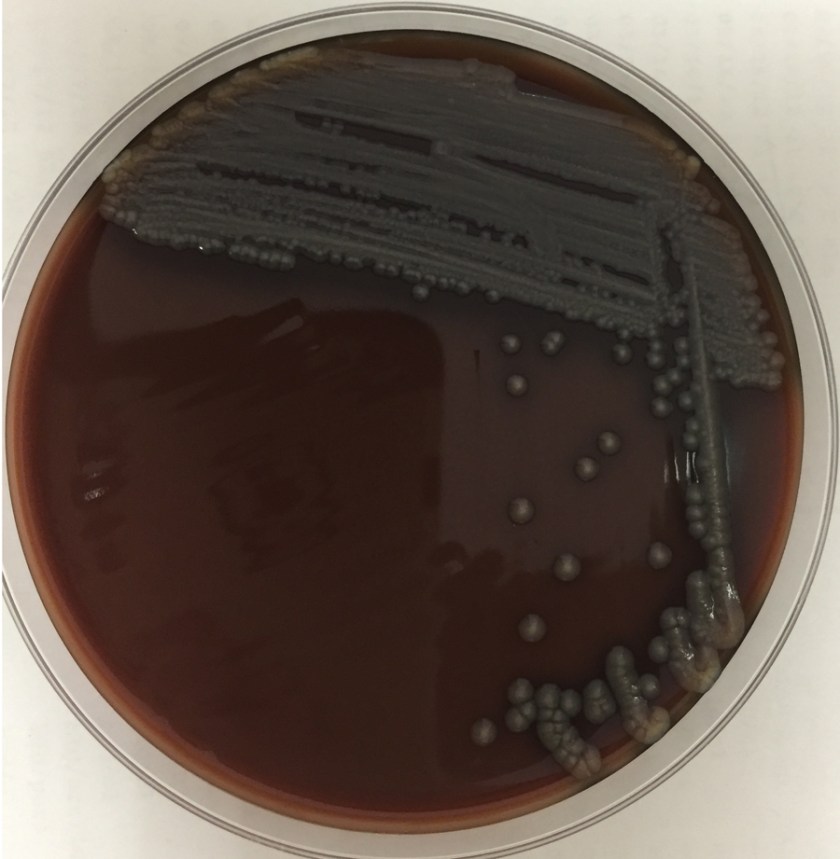
An 8-day-old baby was brought by his family to the Emergency Department. The baby had become irritable in the past 12 hours and was refusing to eat. He was born via vaginal birth at 38 weeks gestation and the pregnancy was uncomplicated besides an intrapartum fever for which mom received antibiotics during labor and baby received 48 hours of antibiotics after birth. In the ED, a lumbar puncture was performed and the resulting cerebral spinal fluid (CSF) had a protein of 353 mg/dL and glucose of <1 mg/dL. The CSF contained 2,935 nucleated cells with a differential of 76% polymorphonuclear cells, 14% macrophages, and 10% lymphocytes. Cytospin Gram stain of the CSF showed many white blood cells but no microorganisms. After 24 hours, an organism was growing on blood and chocolate agar, but not on MacConkey or Colistin Naladixic Acid (CNA) agar (Figure 1A, 1B, and 1C). Before this organism could be identified, the patient’s blood culture signaled positive with the same organism (Figure 2).
Figure 1A. Growth on blood agar.Figure 1B. Growth on chocolate agar.Figure 1C. Growth (or lack thereof) on MacConkey agar.Figure 2. Gram stain of blood culture.
Discussion:
The organism was identified by MALDI-TOF MS (Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry) as Elizabethkingia meningoseptica. This organism was previously named Chyrsiobacterium meningosepticum and before that Flavobacterium meningosepticum.
E. meningoseptica is an oxidase-positive, indole-positive, nonmotile, glucose nonfermenting, Gram-negative rod. It grows well on blood and chocolate agars after 24-48 hours of incubation, but does not grow on MacConkey agar. Colonies appear smooth and can be non-pigmented, like our isolate, or contain a slightly yellow or salmon pigment. Elizabethkingia spp. are environmental organisms which are ubiquitous in water and soil. They can also become nosocomial pathogens due to colonization of hospital sinks and other medical devices associated with water (humidifiers, ice chests, respirators, ect.).
E. meningoseptica is a rare cause of neonatal meningitis with prematurity being the greatest risk factor for infection. E. meningoseptica meningitis has a mortality rate of up to 57% and causes severe sequelae such as brain abscesses and developmental delay in those that survive the infection. Besides neonates, Elizabethkingia spp. have been associated with a variety of infections in immunocompromised patients and currently Wisconsin is in the middle of an outbreak of > 50 patients with Elizabethkingia anopheles bloodstream infections.
E. meningoseptica have a very unusual susceptibility pattern for Gram-negatives rods, which is shared by the closely related organisms Sphingomonas, Chryseobacterium, and Empedobacter spp. They produce β-lactamases making them resistant to most β-lactam antibiotics including carbapanems and aztreonam. E. meningoseptica is generally resistant to colistin and anaminoglycosides as well. They have variable resistance to vancomycin, rifampin, and fluroquinolones, making treatment options scant.
Our case patient cleared his blood and CSF of E. meningoseptica and is clinically improving. Only time will tell the extent of long term sequelae caused by this infection.
References:
Manual of Clinical Microbiology, 11th edition
Mehmet Ceyhan and Melda Celik, “Elizabethkingia meningosepticum (Chryseobacterium meningosepticum) Infections in Children,” International Journal of Pediatrics, vol. 2011, Article ID 215237, 7 pages, 2011. doi:10.1155/2011/215237
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
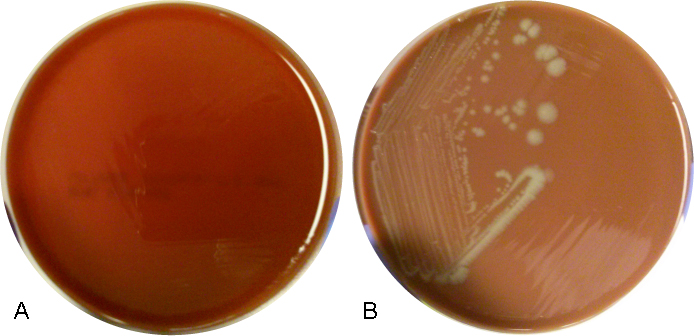
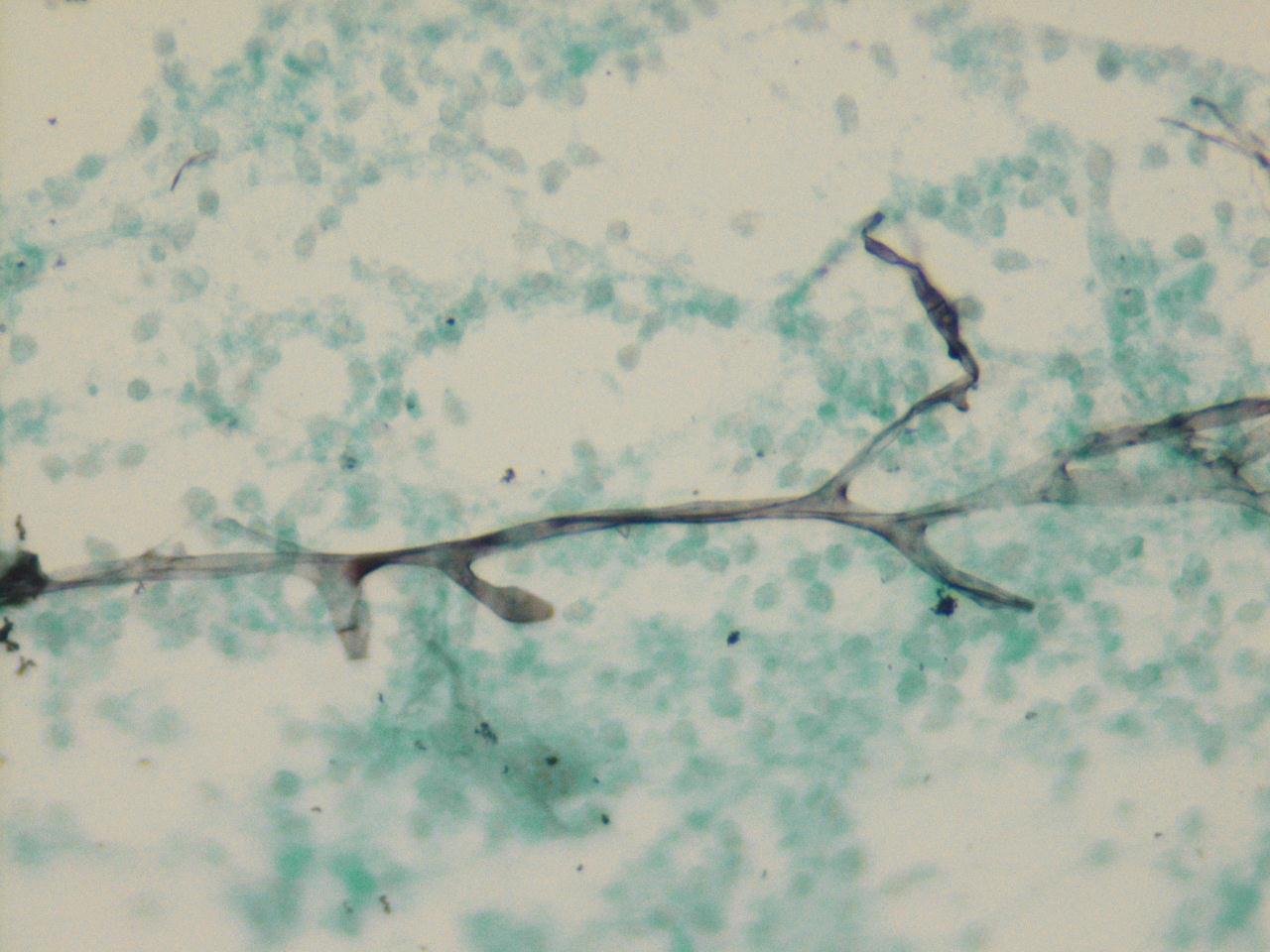
A 7 year old Congolese male presented with pruritic, erythematous, non-flaky rash on top of his scalp for the past 3 weeks. The rash in non-painful, but continues to spread. His mother has been applying hydrocortisone cream nightly, with no improvements.
Colony morphology on fungal media.Organism morphology on lactophenol analine blue scotch tape prep.
Laboratory Identification
A hair sample was obtained for fungal culture. Colonies were yellow and waxy with feet-like projections. Microscopic morphology on lactophenol analine blue scotch tape prep revealed broad hyphae with tortuous branches. The hyphae lacked obvious micro and macro conidia, raising the suspicion for Trichophyton violaceum.
Discussion
Trichophyton violaceum is an anthropophilic fungus seen predominantly in North Africa, East Asia and parts of the Middle East. It forms slow growing with glabrous colonies. Microscopically, broad tortuous hyphae are seen. Microconidia and Macroconidia are notably absent. T. violaceum causes Tinea Capitis, which can be acquired through scalp contact with the dermatophyte, either with direct contact with an infected individual or an object. It can also affect skin, nails and beards. It manifests clinically as pruritic scaly patches with alopecia, often producing black dots. Affected hairs demonstrate an endothrix infection.
-Mustafa Mohammed, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 39 year old African American male presents to the Emergency Department with a three day history of headaches and fatigue. The patient describes his headache as a sharp, constant pain that is exacerbated by movement. He also has been experiencing blurred vision and feeling unstable on his feet. His past medical history is significant for HIV diagnosed 8 years ago. On admission, his absolute CD4 count is 104 with a viral load of 150 vc/ml. He is compliant with his anti-retroviral therapy and Bactrim prophylaxis. Physical exam is unremarkable except for oral thrush. Imaging reveals multifocal areas of enhancement throughout the brain and cerebellum with associated vasogenic edema, which was thought to most likely represent an infectious process. The patient was taken to the operating room for a brain biopsy. Tissue was sent to surgical pathology and the microbiology laboratory for evaluation.
Laboratory identification:
Figure 1. Brain tissue with pyogranulomatous inflammation and a budding yeast form (H&E 400x).Figure 2. Brain tissue with many yeast forms present exhibiting broad based budding (GMS 400x).Figure 3. Growth of a white-tan mold on Sabouraud dextrose, SAB with chloramphenicol and Mycosel agar slants (left to right).Figure 4. Narrow septate hyphae with fine conidiophores giving rise to round shaped conidia (Lactophenol cotton blue, 400x)
The histology results were reviewed first and the H&E stain showed a pyogranulomatous inflammatory response with budding yeast forms. These findings were better visualized on the GMS stain which illustrated numerous yeast forms ranging in size with frequent broad based budding. In the microbiology laboratory, a white-tan mold grew on Sabouraud dextrose, SAB with chloramphenicol and Mycosel agar slants after 18 days of incubation at 30°C. On microscopic examination, the lactophenol cotton blue prep revealed narrow septate hyphae with round conidia at the end of fine conidiophores (characterized as a lollipop appearance). These finding are consistent with a diagnosis of Blastomyces dermatiditis and were confirmed with a DNA probe. Other pertinent laboratory results included urinary antigens positive for both Blastomyces and Histoplasma and a negative cryptococcal antigen in the serum.
Discussion:
Blastomyces dermatiditis is a thermally dimorphic fungus found in the Midwest, Ohio and Mississippi River valleys and the south central portion of the United States. The infection is obtained by inhalation of spores from decaying wood along rivers and patients typically show symptoms consistent with pneumonia. In some cases, particularly in immunocompromised patients, dissemination to the skin, bone and central nervous system can occur.
Morphologic diagnosis can be made from surgical pathology specimens which show broad based, budding yeast forms with a double contoured cell wall, ranging in size from 8-15 µm. In the microbiology laboratory, the mold form grows slowly (2-3 weeks) and is characterized by narrow septate hyphae with delicate conidiophores bearing round to oval conidia which are described as lollipop-like. Due to that fact that Blastomyces is not able to be differentiated from the mold form of Paracoccidioides brasiliensis and Chrysosporium spp., confirmation of the identification is necessary. Traditionally, this was done by temperature induced culture conversion of the mold form to the yeast form but due to the availability of rapid, commercially available DNA probes specific for the exoantigen of Blastomyces dermatiditis, this test is more commonly utilized currently.
Other supplemental tests used in the diagnosis include a Blastomyces urinary antigen which shows good sensitivity in both pulmonary and disseminated disease. In our case, the positive urinary antigen for Histoplasma was considered to be a false positive result due to known cross reactivity with Blastomyces as a result of shared polysaccharides.
Cryptococcus neoformans was also included in the differential diagnosis due to the patient’s HIV status, presenting symptoms and the fact it is a common cause of fungal meningitis in individuals with CD4 counts below 200. This infection was ruled out due to a negative serum cryptococcal antigen. In addition, in tissue Cryptococcus would show variably sized (2-20 µm), narrow based yeast forms with a prominent polysaccharide capsule and grow quickly as a yeast in fungal culture.
In the case of our patient, he was started on Amphotericin B based on the histology results. He experienced resolution of his headaches and recovered well following surgery. His was discharged to an extended care facility for 6 weeks of continued IV antifungal therapy before being placed on oral voriconazole.
-Srinivasa Chekuri, MD, is a 4th year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories.
A 77 year old male with history of asthma, atrial fibrillation, and recurrent respiratory distress when visiting Vermont presented to the ED with progressive dyspnea and wheezing for the past 4 days. Two days prior, he required a “breathing treatment” at his PCP. One day ago, he saw his PCP and was prescribed prednisone and azithromycin. He denies cough, fevers, or chills. He used his albuterol and Advair inhalers which barely helped. He was found to be in Afib with RVR to the 160s, a respiratory rate in the 40s, and an oxygen saturation of 70%.
Kinyoun stain revealing broad rods with cross-barring.Colony growth on Lowenstein-Jensen medium.
Lab Identification
The organism was auramine fluorescent stain positive from the broth. The AFB culture bottle was sub-cultured to agar based medium and Lowenstein-Jensen medium, which yielded small yellow colonies. Kinyoun stain revealed broad rods with cross-barring. The organisms produced a yellow pigment when exposed to light, and a nucleic acid probe for Mycobacterium kansasii was positive.
Discussion
Mycobacterium kansasii was discovered in 1953 by Buhler and Pollack. It is an acid fast bacillus that produces yellow pigment when exposed to light (photochromogen). The bacilli are thick, long and cross-barred and have been described as ladder-like. It is prevalent in the Midwest and Southeast, and is the second most common cause of nontuberculous mycobacteria disease in patients with AIDS. Mycobacterium kansasii manifests as lung disease that clinically appears similar to tuberculosis. It can also cause local disease of the skin and subcutaneous tissue, as well as lymphadenitis and disseminated disease. Symptoms are more severe in immunocompromised hosts. Mycobacterium kansasii is generally acquired via either aspiration or local inoculation from the environment, with little evidence to support person to person transmission.
-Mustafa Mohammed, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 6 year-old girl with a history of posterior fossa ependymoma presented with a one month history of fever, headaches, vomiting and more recently, neck stiffness. Additional history includes remote tumor resection followed by radiation and chemotherapy resulting in remission, with a residual ventriculoperitoneal shunt (VPS). Her parents reported she was in good health until approximately 1 month prior to presentation and is up to date on her immunizations. She was previously seen by her primary care physician for her symptoms and treated her with amoxicillin for suspected strep throat. Upon admission, she received supportive therapy for her symptoms after she was found to have tumor recurrence on imaging. The patient was scheduled for resection approximately two weeks after discharge and on post-operative day two she developed fever, vomiting and neck stiffness again. At this time, blood cultures were drawn and a lumbar puncture (LP) was performed. Cerebrospinal fluid (CSF) from both the LP and VPS submitted for fluid analysis (Table 1) and culture.
Table 1: Cerebrospinal Fluid Analysis
Spinal Fluid
LP
VPS
Appearance
Clear
Clear
Nucleated cells
1075 cells/μL
628 cells/μL
RBC
150 cells/μL
35 cells/μL
Polys
94%
87%
Lymphs
2%
6%
Mono/Macrophage
4%
7%
Glucose
68 mg/dL
13 mg/dL
Protein
69 mg/dL
164 mg/dL
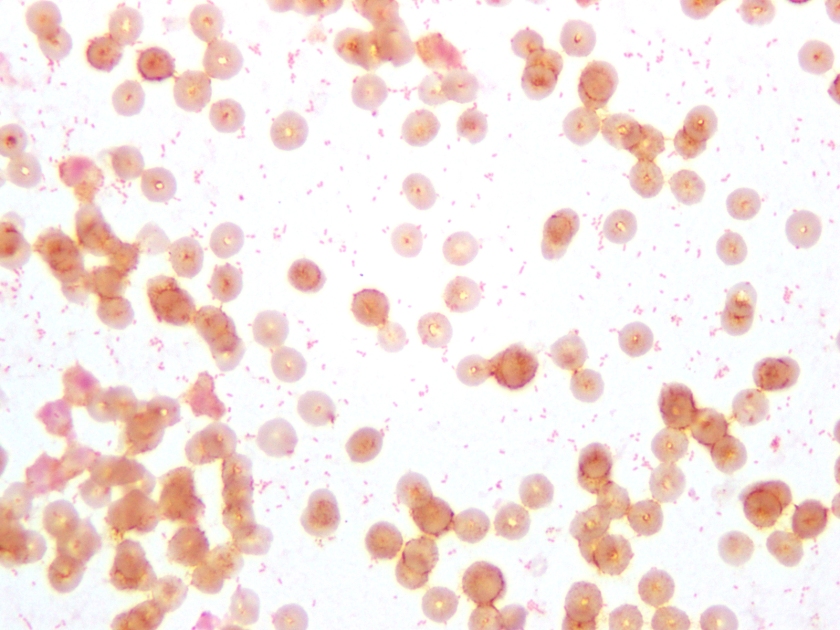
Figure 1. Gram stain of the pathogen isolated from aerobic blood culture, showing gram-negative coccobacilli, sometimes in pairs. The same organism was seen on the patient’s CSF Gram stain.Figure 2. Aerobic blood culture on (A) 5% sheep blood agar plate (BAP), showing no growth and on (B) chocolate agar plate (CAP), showing round, smooth, opaque grey-yellow colonies.
Culture results:
The CSF Gram stain showed rare, paired, Gram-negative diplococci, which could raise suspicion for Neisseria meningitidis, however the typical flattened sides of adjacent bacteria were not observed. Rather, the morphology was more consistent with Gram-negative coccobaccilli, which is better demonstrated on Gram stain of the blood culture (Figure 1). Culture of both the CSF and blood specimens grew fairly large, smooth, round, opaque grey-yellow colonies on CAP, however showed no growth on BAP (Figure 2), suggesting a fastidious organism requiring growth factors. The colonies were both catalase and oxidase positive. The organism was identified as Haemophilus influenzae by MALDI-TOF MS (matrix-assisted laser desorption/ionizations time-of-flight mass spectrometry). This H. influenzae isolate was non-typeable by slide agglutination serotyping performed at the state public health laboratory.
Discussion:
H. influenzae are small, pleomorphic, gram-negative rods or coccobacilli that are non-motile. They are facultative anaerobes that grow best between 35-37°C with 5% CO2. H. influenzae is a fastidious species, requiring hemin (X factor) and nicotinamide-adenine-dinucleotide (NAD/V factor) for growth, which are both available in chocolate agar, but not blood agar. On chocolate agar, the colonies are non-hemolytic, typically large, smooth, round and convex with an opaque, colorless or grey hue. Encapsulated strains, including H. influenzae serotype b (Hib), appear mucoid and are typically small, grey colonies on CAP. Isolates are catalase and oxidase positive. H. influenzae displays the “satellite phenomenon” when grown near Staphylococcus aureus. This occurs when colonies of S. aureus lyse nearby red blood cells releasing hemin and NAD in the media. The presence of extracellular hemin and NAD allow colonies of H. influenzae to grow in the immediate vicinity of S. aureus.
H. influenzae is widely distributed in humans, colonizing the nose and throat and is spread from person-to-person via direct contact or respiratory droplets. Severe infections, including pneumonia, bacteremia and meningitis, affect predominantly infants and children. The American Academy of Pediatrics recommends routine vaccination with the Hib conjugate vaccine for infants aged 2 through 6 months (2 or 3 doses, depending on vaccine product) followed by a booster dose at age 12 through 15 months. Hib is the only serotype preventable by vaccine. Prior to routine vaccination in the US, approximately 20,000 children under the age of 5 were infected with H. influenzae and 3-6% died each year.
-Petra Rahaman, MD is a 4th year Anatomic and Clinical Pathology resident at UT Southwestern Medical Center.
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
A 33 year old African American female presents to the hospital complaining of mild abdominal pain for the past couple of days. She is 17 weeks pregnant and has a history of two prior spontaneous abortions at 15 and 16 weeks due to a shortened cervix. She is afebrile and denies any vaginal bleeding or leakage of amniotic fluid. A complete blood count reveals mild leukocytosis and anemia. On physical examination, her cervix is 2 cm dilated with bulging membranes. She is admitted for a possible cerclage placement, and an amniocentesis is performed to rule out infection prior to the procedure. The microbiology lab received 20 ml of clear, amber fluid for Gram stain and bacterial culture.
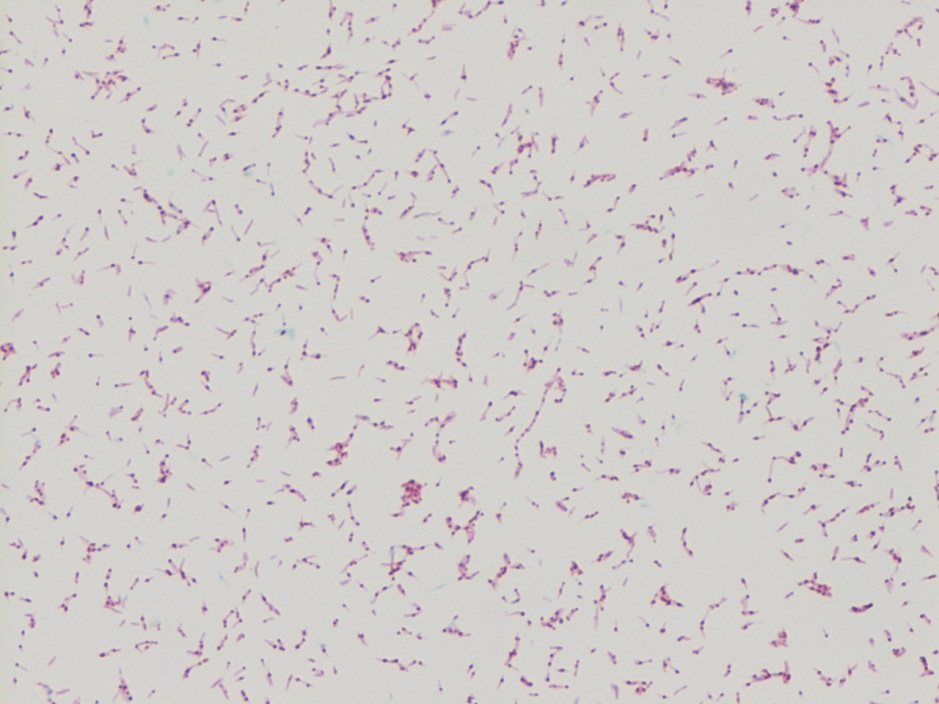
Figure 1. Direct Gram stain from the amniotic fluid showing many neutrophils and fusiform Gram negative bacilli (1000x oil immersion).Figure 2. Wright-Geimsa stain of the amniotic fluid specimen containing many acute inflammatory cells which have engulfed the fusiform bacteria (1000x oil immersion).Figure 3. Small, greyish-white colonies growing on Brucella blood agar after 48 hours of incubation under anaerobic conditions at 35°C.
Laboratory Identification:
The Gram stain showed moderate fusiform Gram negative bacilli in a background of many acute inflammatory white blood cells. Bacterial cultures grew small, greyish-white colonies as Brucella blood agar and routine blood agar after 48 hours of incubation under anaerobic conditions at 35°C. No growth was observed on kanamycin-vancomycin laked blood (KVLB) agar. The organism was identified by MALDI-TOF as Fusobacterium nucleatum and confirmed using the Vitek anaerobic identification card.
Discussion:
Fusobacterium nucleatum is an anaerobic, Gram-negative rod that is non-spore forming. It is considered normal flora of the oral cavity and gastrointestinal & genitourinary tracts of healthy adults. F. nucleatum has been implicated in the pathogenesis of oropharyngeal infections, especially in neutropenic patients with mucositis after receiving chemotherapy or bone marrow transplant. It is an important etiologic agent in a wide spectrum of extraoral infections including bacteremia, brain abscess, osteomyelitis and infections of the genitorurinary tract, including the fetal membranes. There have been many documented cases linking infections with F. nucleatum to chorioamnionitis, preterm birth, and neonatal sepsis. The mode of transmission of F. nucleatum to the amniotic fluid can be as a result of direct extension from the vaginal tract, hematogenous spread or as recently implicated, orogenital transmission.
Given that F. nucleatum is the most common of Fusobacterium species found in clinical specimens and it’s potential to cause significant disease, early identification of the pathogen is important. It grows well on a non-selective anaerobic agar and its growth is inhibited on Bacteroides bile esculin (BBE) and kanamycin-vancomycin laked blood (KVLB) agars. After 48 hours of incubation under anaerobic conditions, the colonies measure 1-2 mm in diameter and have been noted to have a characteristic internal flecking quality that is referred to as “speckled opalescence”. On Gram stain, the fusiform cells of F. nucleatum are long (usually 5-10 µm in length), slender filaments with tapered ends and may contain spherical swellings. In regards to biochemical testing, it is indole positive and lipase negative. Disk testing for Fusobacterium spp. shows the bacteria are resistant to vancomycin and susceptible to kanamycin and colistin.
While susceptibility testing is not routinely performed for all anaerobes, testing is indicated for organisms in pure culture isolated from normally sterile sites or for those more virulent organisms for which susceptibilities cannot be predicted. In the case of Fusobacterium spp., penicillin and ampicillin resistance among isolates of has been reported due to beta-lactamase production and it is recommended that all Gram negative anaerobes have a beta-lactamase screen performed. F. nucleatum is routinely susceptible to metronidazole, clindamycin and beta-lactam beta-lactamase inhibitor combination antibiotics.
In the case of our patient, her diagnosis of F. nucleatum in the amniotic fluid specimen precluded her from obtaining a rescue cerclage procedure. She was transferred to labor and delivery for a uterine evacuation secondary to the intra-amniotic infection and delivered a non-viable fetus. She received ampicillin and gentamicin as intravenous antibiotics.
-Brooke Sims, MD, is a third year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories.
A young girl presented to the emergency department with 6 days of cough, congestion, and intermittent fever up to 102°F. Respiratory viral testing, blood cultures, and a chest x-ray were ordered. The patient was found to be RSV positive and sent home with oral steroids. Two days later she presented the emergency department once again with worsening respiratory symptoms and a positive blood culture with the following organism (Figure 1).
Figure 1. Gram stain demonstrating Gram-positive cocci in pairs and chains.
Our patient developed a Streptococcus pneumoniae superinfection and bacteremia in conjunction with RSV pneumonia.
Identification
S. pneumoniae is a Gram-positive cocci that forms “lancet” shaped pairs on Gram stain (Figure 1). Due to pretreatment with antibiotics, our Gram stain shows some pairs, but many Gram variable chains of cocci as well. S. pneumoniae grows as alpha hemolytic colonies on 5% sheep blood, chocolate, and CAN (colistin nalidixic acid) agar in 12-18 hours, where it forms umbelicated colonies with a characteristic navel-like depression in the middle due to autolysins produced by the bacterium. Some serotypes of S. pneumoniae, primarily serotype 3, have a mucoid phenotype seen in Figure 3. S. pneumoniae is a member of the Streptococcus mitis group, but due to its pathogenic potential it has always been singled out. This is accomplished using two biochemical tests: bile solubility testing with 10% deoxycholate, which dissolves colonies of S. pneumoniae but not those of other Viridans group streptococci, and optochin disc testing, to which S. pneumoniae is sensitive while other Virdians group streptococci are resistant (Figures 2 and 3). Many molecular assays have trouble differentiating S. pneumoniae from S. mitis group due to their similarities on a nucleotide and protein level, so biochemical testing is still a mainstay of organism identification.
Figure 2. Growth of α-hemolytic bacterial colonies on 5% sheep blood agar. Zone around the disc indicates the organism is optochin susceptible.
Figure 3. Growth of mucoid, α-hemolytic bacterial colonies on 5% sheep blood agar. The mucoid colony morphology suggests this isolate is likely serotype 3.
Clinical Significance
S. pneumoniae is known to cause a variety of clinical manifestations in children, from community acquired pneumonia and acute otitis media to bacteremia and meningitis. S. pneumoniae is also a colonizer of the upper respiratory tract; approximately 21% of children in developed countries and 90% of children in developing countries are asymptotically colonized. Due to the high rates of S. pneumoniae colonization in children, direct urine antigen testing is inappropriate, as it cannot distinguish asymptomatic carriage from invasive disease. S. pneumoniae direct antigen detection from CSF has been shown to have < 30% sensitivity and offers no benefit over a routine cytospin Gram stain.
Vaccination in children
Around 2000 the first S. pneumoniae vaccine became available. PCV7 was a heptavalent conjugate vaccine which provided protection from the 7 most common S. pneumoniae serotypes known to cause invasive disease (4, 6B, 9V, 14, 18C, 19F, and 23F). Routine vaccination of children was a huge success which reduced the incidence of invasive pneumococcal disease attributed to vaccine strains by 99%. An indirect benefit of the PCV7 vaccine was that adults >65 years of age saw a 92% decrease in invasive pneumococcal disease caused by PCV7 serotypes, despite not being vaccinated themselves, because of reduced transmission of S. pneumoniae from children to adults. Due to the selective pressure of the vaccine, non-vaccine serotypes of S. pneumoniae such as 19A subsequently became the predominant causes of invasive streptococcal disease. In 2010, a 13-valent pneumococcal conjugate vaccine (PCV13) was FDA approved. It includes all seven S. pneumoniae serotypes contained in PCV7, plus six additional serotypes (1, 3, 5, 6A, 7F, and 19A). PCV13 provides coverage against 2/3 of all serotypes responsible for invasive pneumococcal disease in children under 5 years of age.
Follow up
The patient had an uneventful hospital stay. All subsequent blood cultures were negative and susceptibility testing found the patient’s S. pneumoniae isolate to be susceptible to penicillin, cefotaxime, and clindamycin. The patient and was discharged home after 24 hours of observation with a 7 day course of amoxicillin.
References:
Manual of Clinical Microbiology, 11th edition
Pediatric Red Book, 2015 Report of the Committee on Infectious Diseases, 30th edition
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
A 45 year-old woman was hospitalized for a bilateral subarachnoid hemorrhage with right-sided intraventricular hemorrhage secondary to a basilar artery aneurysm. On hospital day 2, after endovascular coiling of her aneurysm, she developed seizure-like activity. She was found to have new bilateral thalamic and brainstem infarcts with increased hydrocephalus and had an external ventricular drain placed.
She showed some minimal neurological improvements over the next 2 weeks until hospital day 17 when her mental status acutely declined and she developed a fever, leukocytosis, and meningeal signs. 8cc of cloudy, yellow fluid was collected via lumbar puncture. Analysis of the fluid showed pleocytosis (cell count of 54K) with a neutrophil predominance and markedly elevated protein.
CSF Gram stainCSF Gram stainCSF aerobic culture on blood agarCSF aerobic culture on MacConkey
Laboratory Identification:
Initial review of the spinal fluid gram stain showed many polymorphonuclear leukocytes and what appeared to be paired gram negative cocci suspicious for Neisseria meningitidis. However, many organisms lacked the more characteristic “kidney-bean” shape. Further inspection of the gram stain revealed many gram negative organisms which more closely resembled bacilli. Given the patient’s history and clinical course, it was determined the pathological agent was most likely a gram negative coccobacillus. On culture, the bacteria formed smooth, round, opaque colonies on Blood and Chocolate agar and was lactose non-fermenting on MacConkey agar. The bacterial colonies were also oxidase negative.
Mass spectrometry identified the organism as Acinetobacter radioresistens.
Rare gram positive appearing organisms of similar shape were also located on the gram stain. This demonstrates that Acinetobacter is known to occasionally retain the crystal violet stain leading to cases of initial misidentification.
Discussion:
Acinetobacter radioresistens is one of about 30 species of bacteria included in the Acinetobacter genus. Acinetobacter is characterized as a gram negative, aerobic coccobacillus which is non-motile, non-fermentative, and oxidase-negative. It grows well on standard aerobic media and typically forms smooth, round, mucoid colonies at 37°C. Acinetobacter is a water organism which preferentially colonizes aquatic, humid, and tropical environments; perhaps accounting for the increased incidence of Acinetobacter infections between the months of July and October.
While there have been reported cases of community-acquired Acinetobacter pneumonia in Southeast Asia and Australia, in most areas of the world Acinetobacter is known primarily as an agent of nosocomial infections. Studies show that an estimated 33% of healthcare workers are colonized with Acinetobacter and that it is one of the most prevalent bacteria isolated from the white coats of medical students. Despite its ubiquity in hospitals, Acinetobacter infections are relatively rare. Many patients may be colonized with it, but Acinetobacter only usually causes disease in immunocompromised and/or critically-ill patients with long hospitalizations. At particular risk are ventilated patients supported with multiple lines, drains, and catheters. Acinetobacter is reported as the pathological agent in a small percent of ventilator-associated pneumonias, central line-associated bloodstream infections, catheter-associated urinary tract infections, and surgical site infections. It is also recognized as a cause of nosocomial meningitis in neurosurgical patients with external ventricular drains, especially those with a history of intracranial hemorrhage and recent prior antibiotic therapy.
Acinetobacter infections are of particular concern because several species demonstrate resistance to many antimicrobials. Acinetobacterbaumanni, the species responsible for the majority of Acinetobacter infections, has demonstrated resistance to 1st-3rd generation cephalosporins, macrolides, penicillins, and aminoglycosides. Because these infections are robust and difficult to treat, patients with Acinetobacter infections have a 25-75% mortality risk depending on the site of their infection and their baseline cardiopulmonary and immune status. Currently, carbapenems are considered the gold standard treatment.
-Elaine Amoresano, MD, is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
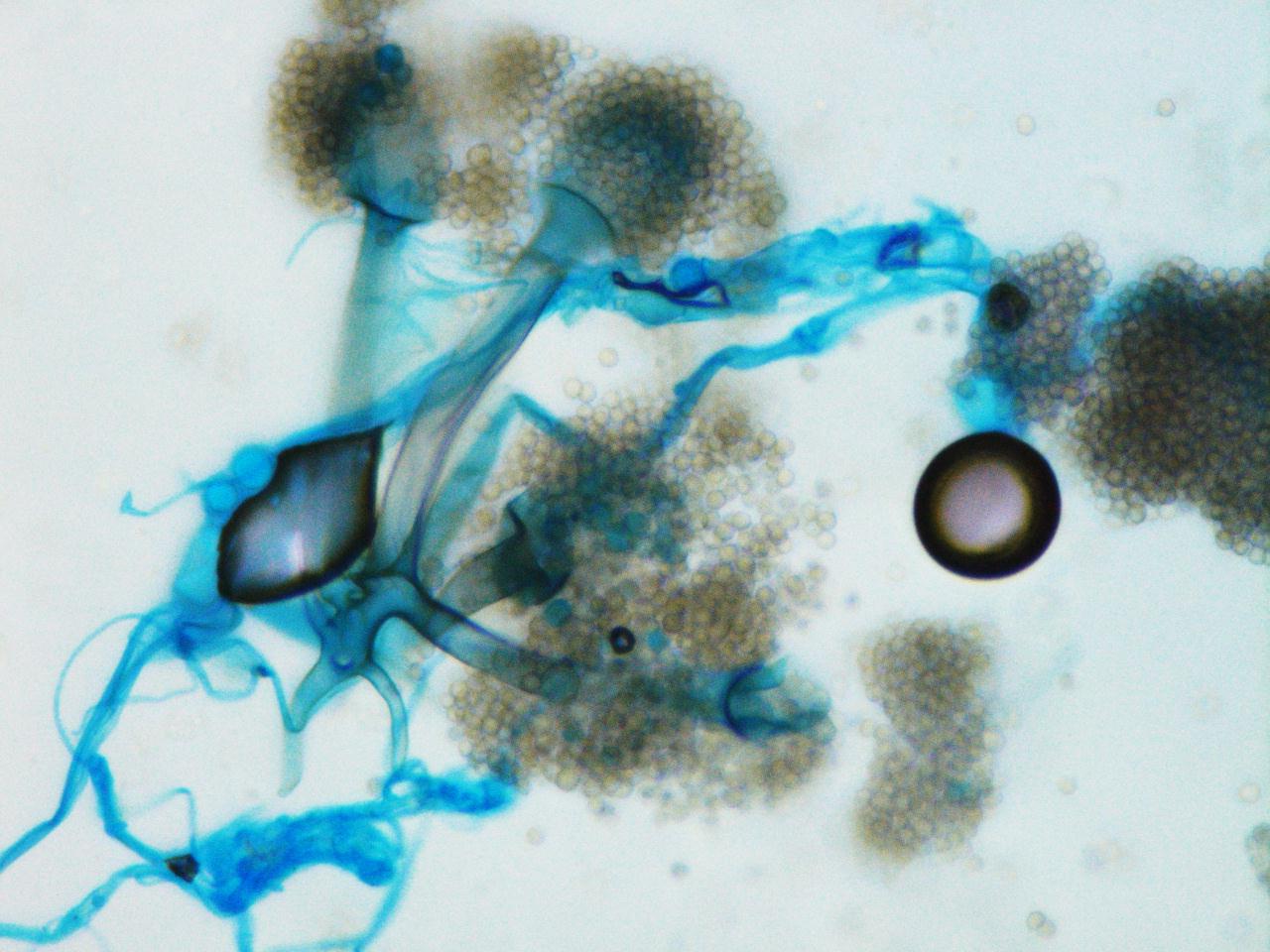
A 65 year old man presents to the emergency room with acute onset back pain. Of note, the man was diagnosed with Burkitt’s lymphoma two months prior and had recently received a course of chemotherapy. During the workup for his back pain, a chest CT is obtained and reveals a 2 cm pulmonary nodule in the left upper lobe with a surrounding “groundglass halo” highly suspicious for invasive fungal involvement. A fine needle aspiration (FNA) of the nodule is performed and tissue is sent for histopathologic examination as well as bacterial and fungal culture.
Chest CT showing a 2 cm nodule in the left upper lobeSilver stain of the FNA specimen showing ribbon-like fungal elements with rare septationsScotch-tape preparation reveals rarely septate hyphae with internodal rhizoids and pyriform sporangia supported by funnel-shaped apophyses.Scotch-tape preparation reveals rarely septate hyphae with internodal rhizoids and pyriform sporangia supported by funnel-shaped apophyses.
Laboratory Identification:
One rapidly growing white colony was identified that became grey over time. The colony was a “lid-lifter” that began pushing at the lid after only a few days. Microscopically, the organisms had broad hyphae with single and branching sporangiophores. At the ends of the sporangiophores there were pyriform, or pear-shaped, sporangia sitting atop funnel-shaped apophyses. Rhizoids were found to be internodal, or arising from the hyphae between the sporangiophores. Based on this morphology, the fungal organisms were identified as Lichtheimia corymbifera complex (formally Absidia corymbifera).
Discussion:
Lichtheimia corymbifera is an organism within the phylum Zygomycota and is one of two pathogenic species in the genus Lichtheimia. This organism is known as an uncommon cause of Zygomycosis and is only implicated in approximately 5% of cases. As in most cases of Zygomycosis, exemplified in our patient, Lichtheimia corymbifera most often affects immunocompromised patients. It is ubiquitous in the environment and is associated with decaying plant matter and soil. Disease is caused by inhalation of spores.
Important points for laboratory identification:
Lichtheimia
Growth at 35-37°C (capable of growth up to 50°C)
Inhibited by media containing cycloheximide
Internodal rhizoids
Pyriform sporangia
Apophysis
Compared to other common Zygomycetes:
Mucor
No rhizoids
Round sporangia
No apophysis
Rhizopus
Nodal rhizoids (directly opposite of the sporangiophores)
Round sporangia
No apophysis
-Britni Bryant, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.