Case:
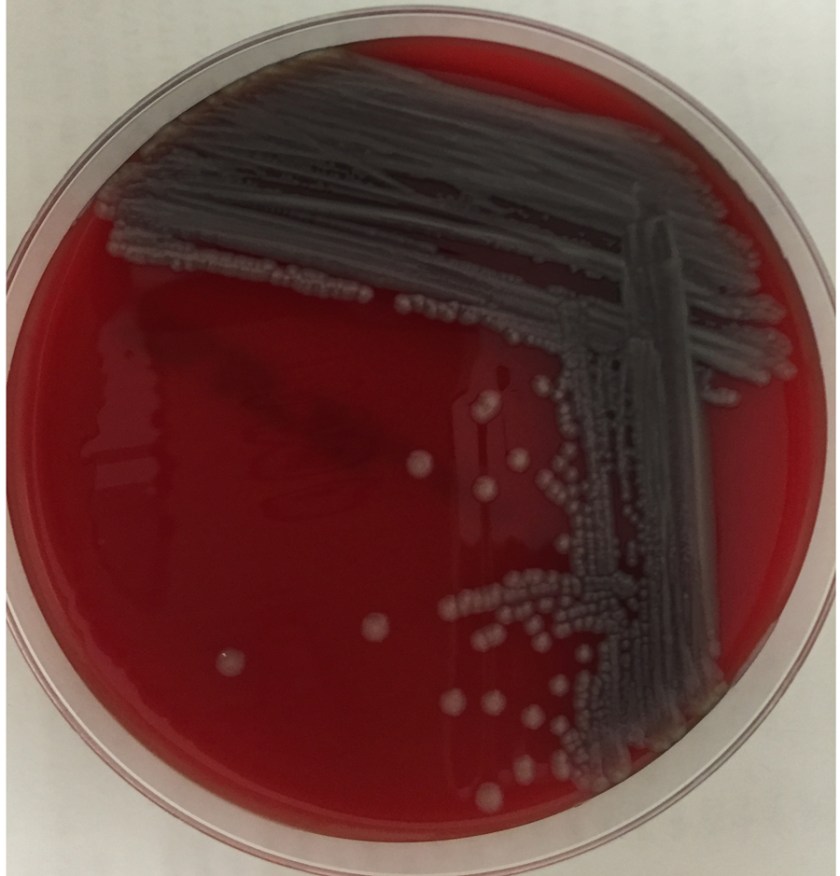
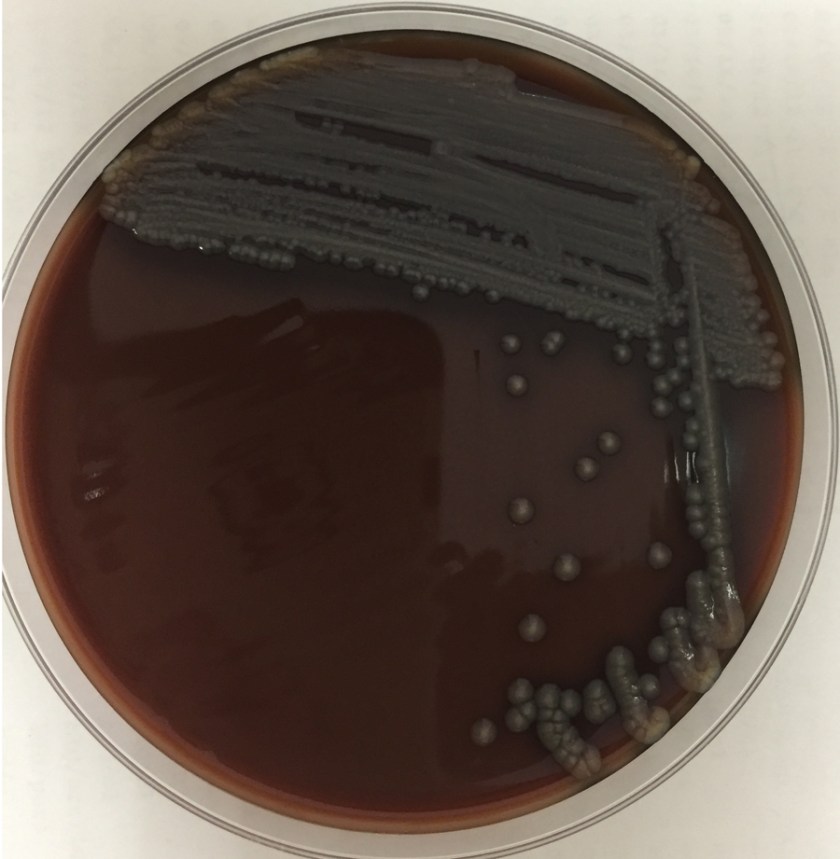
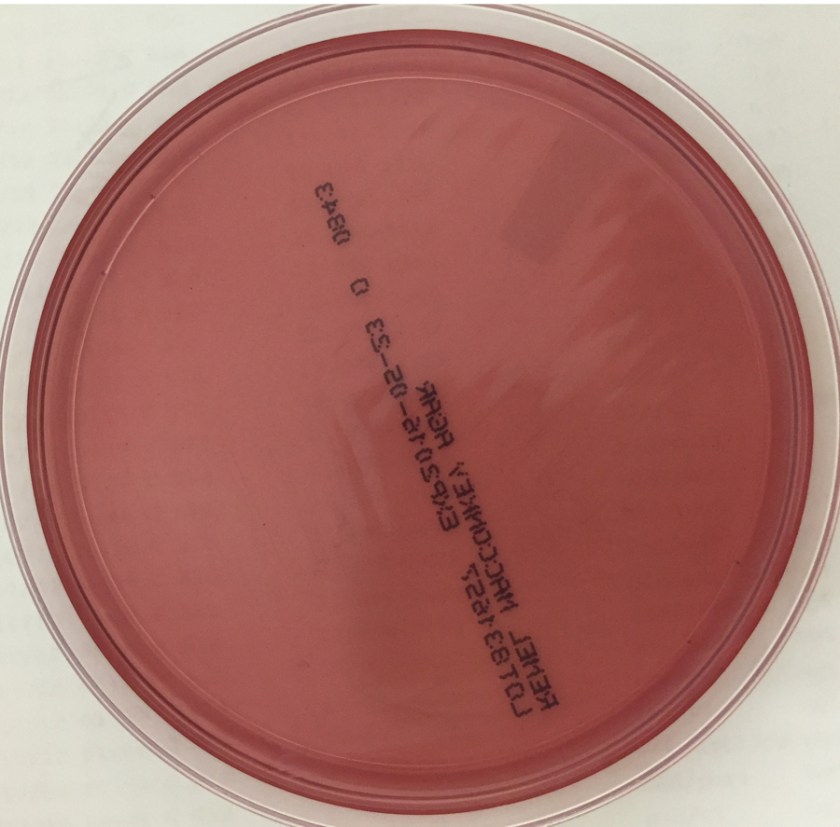
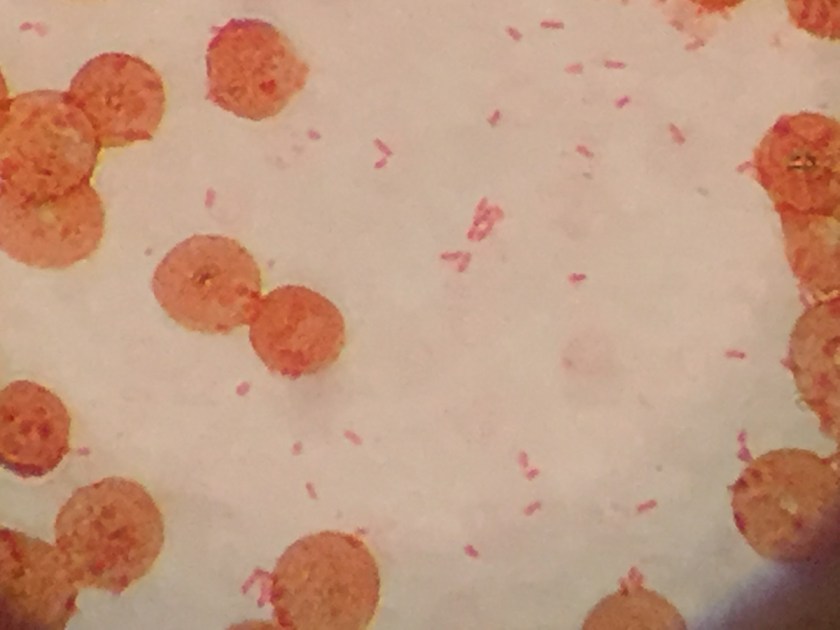
An 8-day-old baby was brought by his family to the Emergency Department. The baby had become irritable in the past 12 hours and was refusing to eat. He was born via vaginal birth at 38 weeks gestation and the pregnancy was uncomplicated besides an intrapartum fever for which mom received antibiotics during labor and baby received 48 hours of antibiotics after birth. In the ED, a lumbar puncture was performed and the resulting cerebral spinal fluid (CSF) had a protein of 353 mg/dL and glucose of <1 mg/dL. The CSF contained 2,935 nucleated cells with a differential of 76% polymorphonuclear cells, 14% macrophages, and 10% lymphocytes. Cytospin Gram stain of the CSF showed many white blood cells but no microorganisms. After 24 hours, an organism was growing on blood and chocolate agar, but not on MacConkey or Colistin Naladixic Acid (CNA) agar (Figure 1A, 1B, and 1C). Before this organism could be identified, the patient’s blood culture signaled positive with the same organism (Figure 2).
Discussion:
The organism was identified by MALDI-TOF MS (Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry) as Elizabethkingia meningoseptica. This organism was previously named Chyrsiobacterium meningosepticum and before that Flavobacterium meningosepticum.
E. meningoseptica is an oxidase-positive, indole-positive, nonmotile, glucose nonfermenting, Gram-negative rod. It grows well on blood and chocolate agars after 24-48 hours of incubation, but does not grow on MacConkey agar. Colonies appear smooth and can be non-pigmented, like our isolate, or contain a slightly yellow or salmon pigment. Elizabethkingia spp. are environmental organisms which are ubiquitous in water and soil. They can also become nosocomial pathogens due to colonization of hospital sinks and other medical devices associated with water (humidifiers, ice chests, respirators, ect.).
E. meningoseptica is a rare cause of neonatal meningitis with prematurity being the greatest risk factor for infection. E. meningoseptica meningitis has a mortality rate of up to 57% and causes severe sequelae such as brain abscesses and developmental delay in those that survive the infection. Besides neonates, Elizabethkingia spp. have been associated with a variety of infections in immunocompromised patients and currently Wisconsin is in the middle of an outbreak of > 50 patients with Elizabethkingia anopheles bloodstream infections.
E. meningoseptica have a very unusual susceptibility pattern for Gram-negatives rods, which is shared by the closely related organisms Sphingomonas, Chryseobacterium, and Empedobacter spp. They produce β-lactamases making them resistant to most β-lactam antibiotics including carbapanems and aztreonam. E. meningoseptica is generally resistant to colistin and anaminoglycosides as well. They have variable resistance to vancomycin, rifampin, and fluroquinolones, making treatment options scant.
Our case patient cleared his blood and CSF of E. meningoseptica and is clinically improving. Only time will tell the extent of long term sequelae caused by this infection.
References:
- Manual of Clinical Microbiology, 11th edition
- Mehmet Ceyhan and Melda Celik, “Elizabethkingia meningosepticum (Chryseobacterium meningosepticum) Infections in Children,” International Journal of Pediatrics, vol. 2011, Article ID 215237, 7 pages, 2011. doi:10.1155/2011/215237
- 2016 Wisconsin Outbreak of Elizabethkingia anopheles https://www.dhs.wisconsin.gov/disease/elizabethkingia.htm

-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.

Great educational case, thanks 🙂
What is antibiotic treatment for this organism
Hi Michael,
There is no standard antibiotic regimen for treating Elizabethkingia spp. Based on case reports of infection in children, piperacillin/tazobactam, fluoroquinolones, +/- aminoglycosides are possible treatment options. There are limited data describing trimethiprim/sulfamethoxazole used in combination with other antibiotics. Our patient was treated with ciprofloxacin and piperacillin/tazobactam and cleared his blood and CSF of the organism.
My newborn son is currently being treated for bacterial meningitis at Cincinnati Children’s Hospital. He was showing no signs or symptoms aside from a fever of 101.6 and repeated arching of the back when breastfeeding in the special care nursery at Fort Hamilton Hospital. He had swallowed and inhaled meconium during birth and was already on antibiotics from day 1. Can meconium cause or increase the risk of bacterial meningitis.
Hi, Bartholomew–
Thank you for reaching out. I’m sorry to hear of your newborn son, and I hope he is already showing improvement. Unfortunately, I’m unable to answer your question–our bloggers aren’t able to give medical advice. Your best bet is to talk with your son’s doctors and nurses–they are better able to answer your questions, since they are very knowledgeable about your son’s case.
We have a 41 year old male in icu with EVD associated ventriculitis and this organism is growing in multiple CSF samples and tested susceptible only to SXT.