A 53 year old man presents to urgent care with a primary complaint of an area of erythema and tenderness around a small black spot on his left shoulder, shortly after returning from Ecuador. He does not report any fevers, chills, or drainage from the affected area. The patient reported that he occasionally felt the area moving. An occlusive Vaseline dressing was applied to the central black spot, and the organism shown below emerged from the wound.
Laboratory Identification
The parasite shown above is a human botfly larva, Dermatobia hominis. The clinical history is strongly suspicious for a botfly infection, and the patient himself suggested the diagnosis.
Dermatobia hominis is identified in large part by its relatively unique presentation combined with identification of the larvae in tissue. Laboratory identification of genus and species involves comparing morphological structures including the anterior and posterior spiracles, mouthparts and cephalopharyngeal skeleton, and cuticular spines. Travel history can also be helpful for genus or species-level identification.
Discussion
The lifecycle of human botflies begins when the female botfly lays her eggs on a mosquito. Once a mosquito feeds on a host, the botfly larva drop onto the host and burrow into the skin. They may remain in that location for up to 10 weeks before dropping off the host into soil to pupate and continue the life cycle.
The human botfly is found in North America, ranging from Mexico to Paraguay and northeast Argentina. Cases in the US are primarily in travelers returning from the botfly’s native range. Measuring the incidence of infection in travelers can be difficult due to the nature of the disease. Experienced travelers may be able to remove the larva at home. In other cases the botfly larva may leave the host before the patient seeks medical care.
Testing for the presence of these larva is easy as they require oxygen coming in through a hole in the skin. Cover the lesion with a thick layer of sterile Vaseline gauze and wait approximately 5-15 minutes for the organism to emerge. Surgery is usually not required as the larva is most often removed intact. Antibiotics should be given following removal of the parasite to prevent secondary infections.
-Britt Boles, MD is a 1st year Anatomic and Clinical Pathology Resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 27 year old male presented to the Emergency Department (ED) with complaints of right knee pain and swelling for one week. Two weeks prior, he tripped while walking to work and began to feel pain in his right calf. Upon physical examination, swelling was noted in his ankles, knee, shoulders, and fingers. The knee and shoulder were tender to palpation. In the ED, he was afebrile and vitals were normal. He denied any sort of injury, chills, or rash and no history of tobacco, alcohol, or illicit substance abuse. CT scan of the lower extremity showed no acute fracture but moderate to large knee joint effusion was observed. He and his fiancé (male partner) has been in a monogamous relationship for almost a decade, however the patient did have a history of gonorrhea nine years ago but was treated. Knee arthrocentesis was performed. The fluid was yellow and cloudy and contained 27,000 WBCs. The Gram stain of the synovial fluid showed many intracellular gram negative diplococci and the joint fluid culture grew out Neisseria gonorrhoeae. PCR of the rectal swab also detected N. gonorrhoeae.
Discussion
N. gonorrhoeae is the causative agent of gonorrhea, a sexually transmitted disease. In the United States, it is the second most commonly reported communicable disease.1 While infections can be asymptomatic, in men, gonorrhea commonly causes acute urethritis with dysuria, urethral discharge, and rarely, epididymitis.2,3,4 In women, gonorrhea can cause cervicitis and lead to pelvic inflammatory disease (PID), infertility, ectopic pregnancy, and chronic pelvic pain.5,6 Those with gonococcal endocervicitis can be co-infected with Chlamydia trachomatis and/or Trichomonas vaginalis, other causative agents of sexually transmitted diseases. N. gonorrhoeae can cause extragenital infections in the pharynx and rectum, which are most commonly seen among men who have sex with men (MSM). Disseminated gonococcal infection is rare (0.5-3% of infected individuals) and can be characterized by low grade fever, hemorrhagic skin lesions, tenosynovitis, polyarthralgia and septic arthritis. Complications of disseminated infections may include permanent joint damage, endocarditis, and meningitis. Gonococcal conjunctivitis mainly affects newborns from untreated mothers.7
Gonorrhea can be diagnosed clinically by a history and physical examination and also, by microbiological methods. Home collection kits are available to increase convenience. On a Gram stain, N. gonorrhoeae, a gram negative coccus, frequently appears within or closely associated polymorphonuclear leukocytes (PMNs) typically as diplococci pairs. Direct smears can be prepared from urethral, endocervical sites, and normally sterile or minimally contaminated sites such as joint fluid. Swab specimens (e.g. urogenital, pharyngeal, vaginal or rectal) should be collected with a Dacron or Rayon swab as calcium alginate and cotton swabs may be toxic or inhibitory for the bacteria.8 Specimens must be transported to the microbiology immediately. 9 Blood and joint fluid are also acceptable specimen types for culture for detection of disseminated gonococcal infection.
Enriched selective media for culture of N. gonorrhoeae includes MTM medium, ML medium, GC-Lect and the New York City medium. Plates should be incubated in a CO2 incubator (between 3-7%) at 35C to 37C for optimal growth.9 Gram negative diplococci recovered from urogenital sites that grow on the selective media and are oxidase-positive can be presumptively identified as N. gonorrhoeae. Another quick biochemical test that can be done is superoxol; N. gonorrhoeae produce immediate bubbling whereas N. meningitidis and N. lactamica produce weak, delayed bubbling. Confirmation using other testing methods such as carbohydrate utilization tests (e.g. N. gonorrhoeae produces acid from glucose only), immunological methods, enzymatic procedures, or DNA probe are also available.10
Compared to standard culture methods, Nucleic Acid Amplification Tests (NAAT) offer more rapid results and increased sensitivity. Additionally, NAATs may also include additional targets such as C. trachomatis, a frequent co-pathogen, as part of the assay. NAATs should be used according manufacturer’s protocols and on validated specimen types. For example, the Cepheid Xpert CT/NG test (as used by our patient here) can be used to test asymptomatic and symptomatic individuals and the acceptable specimen types are urine, pharyngeal, and rectal swabs, patient-collected vaginal swabs, and clinician-collected endocervical swabs.11 Given the legal implications of a N. gonorrhoeae diagnosis in a child, the CDC recommends that NAATs can be used to test for N. gonorrhoeae from vaginal and urine specimens from females and urine for males.12 For extragenital specimens, only validated FDA-cleared NAATs assays using pediatric specimens should be used.
The CDC recommends that uncomplicated gonorrhea be treated with ceftriaxone and azithromycin. However, between 2000-2010s, elevated MICs to both ceftriaxone and cefixime were seen and emerging azithromycin resistance is still a concern. The CLSI M100 currently recommends agar dilution or disk diffusion for antimicrobial susceptibility testing for N. gonorrhoeae. Susceptible and resistant interpretative breakpoints are available for penicillin, most cephems, tetracycline, ciprofloxacin, and spectinomycin. Of note, for azithromycin, only the susceptible category has a breakpoint.13
Image 1. Gram stain of synovial fluid showing many intracellular gram negative diplococci. Image 2. Chlamydia trachomatis and Neisseria gonorrhoeae PCR. Orange and Brown= targets for N. gonorrhoeae; light and dark green=control genes.
References
CDC. Sexually Transmitted Disease Surveillance, 2020. Atlanta, GA: Department of Health and Human Services; April 2022.
CDC. Gonococcal Infections Among Infants and Children. Sexually Transmitted Infection Treatment Guidelines, Atlanta, GA: Department of Health and Human Services; 2021.
CLSI. Performance Standards for Antimicrobial Susceptibility Test. CLSI supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute; 2022, Edition 32
-Maikel Benitez Barzaga, MD is a Pathology Resident (PGY-1) at The George Washington University Hospital. His academic interest include hematology, microbiology, molecular and surgical pathology.
-Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.
I’ve mentioned before how important it is to know clinical history before attending a biopsy, and I cannot stress this point enough. As the first line of screening, the intermediary between clinician and pathologist, the role of the cytologist is to prepare, assess, and convey. In a cancer center, we have three main populations: the patients with the unknown primary, the patients with the suspected primary, and the patients with the suspected metastasis. In the event of a suspected metastasis, we’ll review previous relevant pathology material if we have it onsite. Unless the clinician is requesting additional prognostic markers, the review process helps us eliminate the unnecessary repetition of immunostains (IHC) by confirming that the current material is morphologically consistent with the prior material. Sometimes we still perform old-school cytology without a plethora of ancillary studies. HA!
Most of the endobronchial ultrasound (EBUS) procedures performed at our institution are for lung cancer staging or differentiation between a lung cancer metastasis and an extra-pulmonary metastasis. Not that we don’t see the occasional sarcoid- or anthracosis-related process from time to time, but our most common indication is cancer. For an 88-year-old male patient with multiple lung nodules and both mediastinal and hilar lymphadenopathy, confirmation of metastasis was the main objective of the EBUS procedure. The patient’s pertinent medical history includes former tobacco use, squamous cell carcinoma of the lung (diagnosed percutaneously in 2022), clear cell renal cell carcinoma (s/p partial nephrectomy in 2020), prostate cancer (radiated in 2007), melanoma (excised in 2001), and cutaneous squamous cell and basal cell carcinoma (also previously excised in 2002 and 2008). With an extensive cancer history, the lung nodules and thoracic nodes could be any of them, although metastatic squamous cell carcinoma of the lung was clinically favored. My awesome cytologist colleague, Kelly, attended the EBUS procedure. The Rapid Onsite Evaluation (ROSE) was a clear-cut “adequate for diagnostic material,” and the attending pathologist added “tumor cells present.” The following morning, Kelly stopped by my desk to ask my opinion of the 12R (right hilar) lymph node she was screening. She said, “look at my dots. Do these look like the same cells to you? Or are they different? Because I feel like they’re different.” Before putting the slide on my scope, I asked, “so… like a combined adenosquamous? Or a small cell component?” She replied, “not small cell. Something… I don’t know, but they look different. The patient was recently diagnosed with lung cancer and has a history of renal cell.” I fixated on the H&E cell block slides (Images 1-3) before perusing the Diff-Quik and Papanicolaou-stained slides (Images 4-5). “Uhm… Why are there two different types of tumor cells here?! The cytoplasm here is so… vacuolated, but it’s not quite like lung adeno, and the other group… even the n/c (nuclear-to-cytoplasmic) ratio is different. What is this?” Kelly replied, “okay, so there are definitely two different types of tumor here.” I looked up, “It has to be. Absolutely, yes.”
Kelly entered her diagnosis into our laboratory information system and brought the case over to the pathologist on cytology service for the day. She explained her thought process, and the pathologist also questioned if it was a combined process, such as a lung adenosquamous and maybe the original lung biopsy only sampled the squamous component. With the most recent clinical history of both lung squamous cell carcinoma and clear cell renal cell carcinoma, an IHC panel was appropriately selected. Later that afternoon, the pathologist exclaimed, “IT’S BOTH! IT’S SQUAMOUS AND RCC!” The clusters of squamous cell carcinoma did not stain for PAX8 (a renal cell carcinoma marker) (Image 6), and the same cluster stained positive for p40 (a squamous cell carcinoma marker) (Image 7). Within the same level of the cell block, the cluster of cells that appeared morphologically different than squamous cluster stained positive for PAX8 (Image 8) and negative for p40 (Image 9), confirming a renal cell carcinoma component. A small focus of p40-positive cells was present next to the p40-negative renal cell carcinoma (Image 9), further demonstrating mixed histology. This finding was shared with other pathologists, and the results were immediately called to the pulmonologist as this was a critical finding. Sometimes we encounter a partially involved node where the tumor cells are intermixed with lymphocytes, sometimes the lymph node yields more tumor than the primary site, and sometimes, albeit rarely, we encounter a lymph node infiltrated by two different carcinomas.
Due to the patient’s bulky disease and PD-L1 expression of 30%, the medical oncologists primary aim was to treat the squamous cell carcinoma first and follow up renal cell carcinoma therapy second. After the first few cycles of treatment, the lung nodules have decreased in size, but the thoracic nodes remain unchanged. Once the squamous cell carcinoma is controlled or demonstrates a more significant response, immunotherapy may be added to target both, with a tyrosine kinase inhibitor directed at renal cell carcinoma metastases in the event of progression.
-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
I awoke to a text recently that simply said, “Can I ask you a question?” Having finished medical school 22 years ago, I get this very frequently and know from personal anecdotal statistics that it’s either a medical issue (high probability) or someone needs money (much less common). This is not a text from work nor is it from a channel that will result in additional funds deposited on my behalf. This is from an acquaintance, by which I mean it could be any of the following: family member, friend, colleague, ex-girlfriend of an ex-boyfriend, co-worker, random person I met somewhere, etc. I spent some time on the phone in response to this text, recommended a course of action, and solved the problem. The details of this discussion (or the hundreds of others I had over the years) are privileged and irrelevant. The point is that I was “being a doctor’. A problem was presented by a person in need with real concerns about their health (or a loved one’s), I assessed the information they provided, and suggested a next step. My advice is usually spot on and appreciated which stems from my being cautious but concerned. Another important feature of my advice derives from one of my mantras: “Don’t scare the straights!” (which I learned from the comic genius, Bill Murray, in Ghostbusters).
This is one of the hardest aspects of being a doctor (especially when you are a student). It’s really great that you recognize (sometimes immediately) that someone has a life-threatening illness… but they don’t need to know that unless they are within a safe, secure medical environment where action can be taken. Moreover, medical issues are private for the same reason. It’s pretty clear to all of us that we shouldn’t yell “Fire!” in a crowded theatre or even jokingly say words that sound like “bomb,” at an airport. But here’s a true story of what I mean with medicine. Many years ago, I happen to be on an airplane (at cruising altitude) coming back from Africa, where my friend, Paul Farmer (RIP), was also a passenger. Another colleague of ours (a surgeon) was also on the plane. Paul was having an eye issue which looked mild but irritating. Our colleague said, loudly in her confident tone, “Do you think it could he Ebola?” Paul and I exchanged a quick glance, both thinking, “Don’t scare the straights!” I think you see my point. But, for clarity, a personal example. One winter, my husband and I were returning from the city to our suburb, which required a brisk, long walk from the train. The sidewalks were icy and, in places, uneven. He stepped off and fell full force on his shoulder. The next morning he couldn’t move it and it was painful. My immediate thought was, “He broke his shoulder.” Did I say, “Dude, you totally broke your shoulder!” No. We were having an open house to sell our place and he was all stressed about it. So, I said, “Be careful with your arm and we will go to urgent care afterward.” This made him calm. I even made him drive to urgent care (it was not his dominant shoulder) to reassure him he was okay. In urgent care, the ortho surgeon (who happened to be that day’s coverage) walked in after the x-ray and said, “Dude, you broke your shoulder!” And my husband promptly passed completely out onto the examination table. It’s all about understanding the acuity of the situation and striving to not make it worse.
Have I ever been wrong? Of course! Because the only way to truly care for a medical concern is to evaluate it yourself in person with appropriate tools. And almost all of the times I have been wrong (which is only a few), there was some crucial aspect that was not shared because either it wasn’t known or there was discomfort with sharing.
But what I am describing is not unique to me. I’m quite sure every doctor gets these calls with frequency. It’s the purest form of practice because there is no financial transaction presumed, assumed, or demanded.
But what about “doing my job?” Let’s break that down. I work for a non-profit and have a private consultation practice (non-overlapping, non-conflicting). Currently, I am financially compensated (at about $175/hour (pre-tax)) for any/all of the following: health system implementation, grant writing/administration, education, research management, social media production/communication, expert scientific/business consultations, committee participation, abnormal laboratory case review, daily laboratory management, intra-operative consultation, market insights/research, etc. Not much of that sounds like I’m fighting death and stamping out disease at the individual patient level, the life task I as trained for in medical school. Importantly, I’m also hard salaried across all my work so I don’t do individual billing except for a few things like abnormal slide review. Many of my physician colleagues do have to engage in individual billing. But I think much of what I do still sounds very familiar to many of my physician colleagues who see patients every day. When (in my opinion) my physician colleagues should be spending every hour of every day “being a doctor,” as I described above, I fear they spend a lot of time instead documenting, managing, and administrating to ensure they are compensated. I am of the very unpopular opinion that healthcare should be free but I also believe healthcare workers should be compensated aligned to their impact on patients. The medical profit insistence paradigm continues to widen inequity while decreasing the care time for patients in lieu of format/template/documentation to justify billing. I have to spend time doing this non-patient care but, fortunately, they are limited because of the narrow slice of medical billing to which my services are privy.
Here is a specific example to demonstrate the difference I’m discussing. I received an abnormal smear to review from the laboratory. The white blood cell count was over 400,000 cells (ref 10 – 30), the smear was a “medical student”-level diagnosis, the patient was on a supposedly effective treatment, but they had left against medical advice. There are many ways to respond to this case. My question was, “Is this patient okay, right now?” and my immediate action reflex said, “This patient needs to see an oncologist right now.” But she left AMA. How you as a patient or doctor respond to this says a lot about you as a person but also about the fiscal constraints in which you work. What did I do? I called the patient who had, thankfully, been admitted elsewhere, and asked them to please have their doctor call me back. The doctor did, I told them the information, and my suggestion that oncology see them immediately. Oncology saw them a few hours later. Let’s summarize. I spent about 20 minutes reviewing all of the clinical and laboratory information, about 1 hour on the phone over 2 days, and about 10 minutes documenting all of this in the patient’s medical record. I was subsequently paid an additional $25 two months later for that documentation by the patient’s insurance company. So, I “did my job” for $16.67/hour over my base but I was also “being a doctor,” which likely was best for the patient. Which is most important at the end of the day? I certainly didn’t need the extra $25 but the patient definitely needed my input. Importantly, note that the insurance company valued my time at a 10-fold lower rate than did my hospital.
A recent study demonstrated that when nurse practitioners are used instead of physicians, healthcare costs were higher.1 This study follows other studies which have shown the opposite. I don’t have an opinion about quality of care, appropriateness, or territorial pissings in the current debate between MDs and NPs about scope of practice; in fact, I see NP’s quite frequently for my healthcare. But we are all being asked to always be conscious of costs in healthcare when all we should be focusing on is, “How is the patient doing right now?” Grand efforts, like task shifting domestically and internationally, are assumed to save money but they simply don’t do so universally. Where costs could be easily cut (i.e., administration) or outsourced (i.e., finance, HR, IT), they aren’t because C-suites are in charge of cost cutting. But doctors (and NPs and all front line medical workers) are the ones being told to be cost conscious and find cost savings—when their job should only be asking the question, “How is the patient doing right now?”
I love “being a doctor,” especially when I can help someone reach a positive outcome. I love “doing my job” because it’s variable, ever-changing, challenging, rewarding, and I feel my compensation is appropriate. I really love when “doing my job” and “being a doctor” align around the same task. Finding this alignment as frequently as possible produces the happiest healthcare workers and the best care for patients, in my opinion.
Note: As an employee of a 501(c)(3), my salary information is public knowledge.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
A 32 year old male with alcoholic cirrhosis presented to the emergency department with progressive lower extremity swelling. On presentation he was found to have jaundice due to hemolytic anemia secondary to spur cell anemia. Admission hemoglobin was 4.3 mg/dL (4.0-11.0 mg/dL) and bilirubin, both total and direct, were 6.3 mg/dL (0.2-1.3 mg/dL) and 2.9 mg/dL (0.0-0.5 mg/dL), respectively. He also had acute kidney injury (AKI) thought to be secondary to hepatorenal syndrome leading to the development of anasarca. A urinalysis was performed as part of the evaluation for his AKI that showed 100 WBC/HPF, > 187 RBC/HPF, and moderate bacteria which triggered a urine culture.
Laboratory Identification
Urine received in the microbiology laboratory was plated on Blood and MacConkey/CNA agars and grew non-hemolytic, lactose-fermenting gram negative rods (Image 1). Indole testing was negative. Given this biochemical pattern, a member of the Enterobacterales was suspected as typically seen in urine cultures. However, MALDI-TOF MS provided the surprising identification of Salmonella enterica subsp. arizonae. Xylose Lysine Deoxycholate (XLD) agar was set up to confirm the unusual identification (Image 2). Hydrogen sulfide production is typical of Salmonellae, and lactose fermentation, a trait unique to some isolates of S. enterica subsp. arizonae, was confirmed. The organism was submitted to the Texas Department of Health laboratory where the isolate was definitively identified as Salmonella enterica subsp. arizonae (IIIa 14:z4,z23) by whole genome sequencing.
Image 1. Patient isolate of S. enterica subsp. arizonae exhibiting lactose fermentation on MacConkey agar after 18 hours of incubation at 35°C (A). Lactose-fermentation is a unique hallmark of S. enterica subsp. arizonae compared to other Salmonellae (B).Image 2. Patient isolate of S. enterica subsp. arizonae exhibiting hydrogen sulfide production and lactose fermentation on XLD agar after 18 hours at 35°C (A). Note the abundant yellow color of the medium (black arrowhead) compared to S. enterica subsp. Enterica serovar Enteritidis which does not ferment lactose, but also produces hydrogen sulfide (B, white arrowhead).
Discussion
This is a rare case of an extraintestinal infection caused by Salmonella enterica subsp. arizonae. Salmonellaeare motile, gram negative, facultatively anaerobic bacilli that are members of the Enterobacterales. The genus is composed of two species, S.enterica and S. bongori. Salmonellaenterica is further subdivided into six subspecies: enterica (group I), salamae (group II), arizonae (group IIIa), diarizonae (group IIIb), houtenae (group IV), and indica (group VI). Salmonella bongori used to be classified as group V but was separated as a unique species based on genomic analysis.1S. bongori almost exclusively causes zoonotic infections, while S. enterica subsp. enterica is the most frequent cause of human clinical disease. Salmonella taxonomy is complicated further by the division of members of S. enterica subsp. enterica into >2500 unique serovars based on immunoreactivity to lipopolysaccharide (O) and two flagellar (H) surface antigens. These are then further separated into “typhoidal” and “non-typhoidal” serovars based upon the characteristics of infection (Image 3).
Image 3. Hierarchical structure of Salmonella taxonomy. S. enterica subsp. arizonae is boxed in red to highlight is taxonomic position away from other pathogenic Salmonellae. Adapted from reference number 6.
Until recently, determinative testing was almost uniformly performed by serological confirmation of agglutination with O and H antigen-specific antisera. This has been a mainstay of epidemiological analysis of foodborne Salmonella outbreaks. Only recently has whole genome sequencing been adapted as a higher throughput and more discriminatory alternative to classical serotyping schemes. Salmonella nomenclature often uses a genus-species-subspecies format followed by serovar (e.g. Salmonella enterica subsp. enterica serovar Typhi), or it can be reported as genus-serovar for short (e.g. Salmonella Typhi). Formal identification will include information concerning the two flagellar antigens and lipopolysaccharide antigens, in addition to the formalized subspecies using the formula: genus-species-subspecies [space] O antigens [colon] Phase 1 H antigen [comma] Phase 2 H antigen. In this case, the formal identification from the state laboratory for this isolate was Salmonella enterica subsp. arizonae IIIa 14:z4,z23.
About 99% of human infections are due to Salmonellaenterica subspecies enterica (group I)including the serotypes Enteritidis, Typhimurium, Typhi, Paratyphi.2 Infections due to Salmonella enterica subspecies arizonae are rare; serovar IIIa 41:z4,z23 is associated with 10-20 infections per year.3 Infection typically begins as gastroenteritis from food poising or from animal sources, particularly reptiles or poultry. Disease is typically seen in the young and immunocompromised and can progress to invasive disease including sepsis, meningitis, and osteomyelitis.4 It is unclear why there are lower rates of Salmonella enterica subspecies arizonae infections in humans as compared to Salmonella enterica subspecies enterica, but there is evidence to suggest Salmonella enterica subspecies arizonae and diarizonae have altered intestinal colonization in murine models leading to failure of Salmonella to persist in the mammalian intestinal tract.5
This patient had alcoholic cirrhosis and uncomplicated cystitis secondary to Salmonella extraintestinal infection at the time of presentation. It is unclear if this patient had gastroenteritis prior to developing cystitis and the limited medical history did not reveal exposure to reptiles or poultry. In this case, the patient completed seven days of ceftriaxone without complication or recurrence of infection.
References
Agbaje M, Begum RH, Oyekunle MA, Ojo OE, Adenubi OT. Evolution of Salmonella nomenclature: a critical note. Folia Microbiol (Praha) 2011; 56(6): 497-503.
Brenner FW, Villar RG, Angulo FJ, Tauxe R, Swaminathan B. Salmonella nomenclature. J Clin Microbiol 2000; 38(7): 2465-7.
Shariat NW, Timme RE, Walters AT. Phylogeny of Salmonella enterica subspecies arizonae by whole-genome sequencing reveals high incidence of polyphyly and low phase 1 H antigen variability. Microb Genom 2021; 7(2).
Abbott SL, Ni FC, Janda JM. Increase in extraintestinal infections caused by Salmonella enterica subspecies II-IV. Emerg Infect Dis 2012; 18(4): 637-9.
Katribe E, Bogomolnaya LM, Wingert H, Andrews-Polymenis H. Subspecies IIIa and IIIb Salmonellae are defective for colonization of murine models of salmonellosis compared to Salmonella enterica subsp. I serovar typhimurium. J Bacteriol 2009; 191(8): 2843-50.
Achtman M, Wain J, Weill FX, Nair S, Zhou Z, et al. (2012) Multilocus Sequence Typing as a Replacement for Serotyping in Salmonella enterica. PLOS Pathogens 8(6): e1002776. https://doi.org/10.1371/journal.ppat.1002776
–Denver Niles, MD is the Medical Microbiology fellow at UT Southwestern Medical Center. Prior to his Medical Microbiology fellowship, he completed pediatric infectious disease training at Baylor College of Medicine/Texas Children’s Hospital.
–Muluye Mesfin, SM(ASCP)CM is the microbiology laboratory supervisor at UT Southwestern Medical Center where he has worked for 12 years. Prior to this, Mo completed a bachelor of science degree in medical technology at the University of Maryland.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
An adult woman presented to the emergency department five days after undergoing gynecological surgery. The patient presented with fever and severe right lower quadrant abdominal pain. Computed tomography (CT) scan with contrast showed a ring enhanced loculated fluid collection within the cervix, which was concerning for an abscess. The patient was admitted to the hospital and empirically started on piperacillin-tazobactam, but continued to have fevers despite the antibiotics. Blood and urine samples were sent to the microbiology lab for bacterial culture but no organisms were isolated from either source. Two days later, the patient underwent a diagnostic laparoscopy, abdominal wash-out, and drainage of the abscess. The abscess fluid was sent for aerobic and anaerobic bacterial culture. Gram stain of the specimen showed 3+ white blood cells with no organism seen. The anaerobic culture grew 4+ pinpoint white colonies on blood agar after 5 days of incubation. Further identification of these colonies by MALDI-TOF MS revealed Mycoplasma hominis.
Image 1. Blood agar with 4+ pinpoint translucent colonies.
Discussion
Mycoplasma hominis is often a commensal of the urogenital tract, but it can be associated with urogenital infections including pelvic inflammatory disease (PID), pregnancy-related infections, and urethritis in males. There are multiple risk factors for Mycoplasma hominis genital infection including young adult age, multiple sexual partners, and pregnancy. Immunocompromised patients have a higher risk for Mycoplasma hominis extragenital infections as nearly 50% of reported extragenital infections isolated from immunocompromised patients.2Mycoplasma hominis can cause extragenital infections including septic arthritis,4 septicemia, osteitis, retroperitoneal abscesses3, mediastinitis,1 and pneumonia.
Laboratory diagnosis of Mycoplasma hominis is challenging due to the fastidious nature of the organism and its lack of the cell wall makes it undetectable by gram staining. The more specific tests including molecular tests for Mycoplasma hominis are not routinely ordered unless there is a strong clinical suspicion, which makes diagnosis more challenging. Mycoplasma hominis can grow on 5% sheep blood and chocolate agars; however, such growth is very slow and may take from 2 to 7 days of incubation.1 The usual growth of Mycoplasma hominis reveals tiny-sized pinpoint colonies that may be overlooked (Image 1). Once growth is observed, MALDI-TOF MS can be used for identification.6
There are multiple types of selective media for the isolation of Mycoplasmahominis including SP4 agar supplemented with arginine, Hayflick agar, A7, and A8 agars.9 Both A7 and A8 agars contain arginine to enrich Mycoplasma growth but differ in the antibiotic content used to inhibit the growth of other commensals. Agar plates should be put for incubation under 5 to 10% CO2 or under anaerobic conditions at 35°C for at least 5 days.9 On these selective agars Mycoplasma hominis has a characteristic fried egg appearance and can be seen by the aid of a stereomicroscope. However, use of specific agar is not widespread.
Molecular testing of Mycoplasma hominis using nucleic acid amplification (NAAT) assays such as polymerase chain reaction (PCR) is a more sensitive and faster method of detecting Mycoplasma hominis compared with culture. However, PCR is neither widely available nor standardized. PCR assays for Mycoplasma hominis generally use 16S rRNA as a gene target, but other targets, including gap, fstY, and yidC, have been developed.7 Clinical picture should be taken into account when evaluating the significance of a positive PCR test as Mycoplasmahominis can be a commensal organism and PCR does not distinguish between live and dead organisms.
Mycoplasma spp. lack a peptidoglycan cell wall. This makes Mycoplasma spp. intrinsically resistant to β-lactams and to all antibiotics, which target the cell wall, including glycopeptide antibiotics. Mycoplasma hominis is also resistant to rifampin, sulfonamides and trimethoprim. Tetracyclines, macrolides, and fluoroquinolones are often used. Antimicrobial susceptibility testing is rarely performed, with only a few specialized laboratories offering the testing. Clinical and laboratory standards institute guidelines (CLSI M43) is followed using microbroth dilution. Agar disc diffusion testing is not used for Mycoplasma hominis as there is no correlation between inhibitory zones and minimal inhibitory concentrations.8Mycoplasma hominis can be evaluated for susceptibility to clindamycin, tetracycline, and levofloxacin.10
After isolation of Mycoplasma hominis was reported, doxycycline was added to the patient’s antibiotic regimen. The patient responded well with subsiding of the fever and stabilization of her vital signs.
References
Xiang, L., & Lu, B. 2019. Infection due to Mycoplasma hominis after left hip replacement: case report and literature review. BMC infectious diseases, 19(1), 50. https://doi.org/10.1186/s12879-019-3686-z
Meyer RD, Clough W. 1993. Extragenital Mycoplasma hominis infections in adults: emphasis on immunosuppression. Clin Infect Dis. Suppl 1:S243-9. doi: 10.1093/clinids/17.supplement_1.s243. PMID: 8399923.
Adams M, Bouzigard R, Al-Obaidi M, Zangeneh TT. 2020. Perinephric abscess in a renal transplant recipient due to Mycoplasma hominis: Case report and review of the literature. Transpl Infect Dis.(5):e13308. doi: 10.1111/tid.13308. Epub 2020 Jul 7. PMID: 32378787.
Luttrell LM, Kanj SS, Corey GR, Lins RE, Spinner RJ, Mallon WJ, Sexton DJ. 1994. Mycoplasma hominis septic arthritis: two case reports and review. Clin Infect Dis.19(6):1067-70. doi: 10.1093/clinids/19.6.1067. PMID: 7888535.
Pereyre S, Tardy F, Renaudin H, Cauvin E, Del Pra Netto Machado L, Tricot A, Benoit F, Treilles M, Bebear C. 2013. Identification and subtyping of clinically relevant human and ruminant mycoplasmas by use of matrix-assisted laser desorption ionization–time of flight mass spectrometry. J Clin Microbiol 51:3314–3323.
Ferandon C, Peuchant O, Janis C, Benard A, Renaudin H, Pereyre S, Bebear C. 2011. Development of a real-time PCR targeting the yidC gene for the detection of Mycoplasma hominis and comparison with quantitative culture. Clin Microbiol Infect 17:155–159.
Clinical and Laboratory Standards Institute. 2011. Methods for antimicrobial susceptibility testing for human mycoplasmas; approved guideline M43-A. Clinical and Laboratory Standards Institute, Wayne, PA.
Stabler S, Faure E, Duployez C, Wallet F, Dessein R, Le Guren R. 2021. Mycoplasma hominis extragenital abscess. J Clin Microbiol, 59(4). https://doi.org/10.1128/JCM.02343-20
–Omar Abdelsadek, MD is a PGY-1 (AP/CP) Pathology Resident at University of Chicago (NorthShore) Pritzker School of Medicine.
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
A 27 year old female with a history of substance abuse, presented to the ED with a swollen left eye, resulting from a fall in the shower that hit her eye on the tub. She denies losing consciousness or neck pain. Her eye has swollen since then and she noticed yellow drainage from her eye. Her past medical history was unremarkable although she was diagnosed as having sexually transmitted infections (STI) with Neisseria gonorrhoeae and Chlamydia trachomatis 3 months prior to the current event. Her HIV and syphilis screening were negative.
The drainage from her eye was collected for culture and Gram stain and sent to the Microbiology laboratory. The initial Gram stain showed moderate neutrophils and very few gram negative diplococci (GNDC). The culture grew pure growth of the same organism on Chocolate agar during overnight incubation. It was identified as Neisseria gonorrhoeae by MALDI-ToF. The patient was reached out by the emergency nurses for the Ceftriaxone injection.
Discussion
Neisseria gonorrhoeae belong to the Neisseriaceae family, including Kingella, Eikenella, and many other genera. Neisseria gonorrhoeae is gram negative cocci in pairs and have a distinct kidney bean shape. They thrive in the mucous membranes of the respiratory and urogenital tracts.1 While the pathogenicity tends to vary among Neisseria spp; N. gonorrhea is a primary pathogen that does not belong in the usual flora of humans in any amount, unlike other Neisseria that are opportunistic and can be part of usual flora.1N. gonorrhoeae only has been reported in human cases. N. gonorrhoeae and N. meningitidis are considered fastidious organisms that require CO2 and iron. These organisms are aerobic bacteria that only grow on chocolate media that has RBC hemolyzed. When N. gonorrhoeae infects humans; it has a surface receptor that binds transferrin directly competing with the human host for iron supplies.1 Transferrin is a glycoprotein that delivers iron throughout the body.2
N. gonorrhoeae is typically acquired through unprotected sexual activity. Once transmitted, it can be found in vaginal, oral and anal secretions.3 The recorded cases of N. gonorrhoeae in 2018-2019 have gone up 5.9%; since 2009 there has been a 92.0% increase in cases, with a lot more young men contracting the disease since 2009.3 Improvement in screening and tracking techniques can also be a reason for the drastic increase in U.S cases.3 While most of the time N. gonorrhoeae stays in the mucosal membranes, it can also thrive in other parts of the body.1 The most common genital infection causes painful urination, a pus-like substance that discharges from the penis, and pain and tenderness in the testicular region.4 For women, it can cause increased discharge, pelvic pain, and bleeding between periods.4 Untreated genital N. gonorrhoeae can cause pelvic inflammatory disease (PID) which can lead to abortion and sterility in both men and women.1N. gonorrhoeae also has the potential to affect but is not limited to the rectum, eyes, throat, and joints where it can cause pain, swelling, and rashes.4 Pregnant women that have an N. gonorrhoeae infection can pass it onto their offspring through vaginal delivery, and it is very important to screen for N. gonorrhoeae during pregnancy.4 In the US providers must put antimicrobial (erythromycin) eye drops in the babies born regardless of the STD status of the mother.1 A neonate exposed to N. gonorrhoeae can develop blindness and rashes.1 Untreated N. gonorrhoeaecan commonly causes recurrent rectal infection in women. While ocular gonococcal eye infection can be encountered more frequently in neonates born to infected mothers through vaginal delivery, ocular gonococcal infections in adults are extremely rare and can potentially be caused by incidental inoculation of infected genital secretions of their own (auto-infection).1
In most cases, N. gonorrheae can be cultured from a swab of the male urethral or female endocervix, or vaginal samples. Non-genital samples, such as rectal and oral sources can also be used to diagnose extra-genital gonococcal infections. Nucleic acid amplification tests (NAAT) are commonly used for rapid diagnosis of gonococcal infection from genital, anal, or oral sources. For samples collected from other sources, culture is the primary method of the diagnostic approach. N. gonorrhoeae grows well on chocolate agar. MTM (modified Thayer martin) agar supports the growth of N. gonorrhoeae as it is a selective media for N. gonorrhoeae, containing nystatin, colistin, and vancomycin to suppress the growth of other bacteria.5N. gonorrhoeae was susceptible to penicillin in 1976, and, by 1980, penicillinase-producing N. gonorrhoeae was discovered in Southwest Asia.1 The most common treatment is ceftriaxone intramuscularly with oral azithromycin for those who are allergic to cephalosporins like ceftriaxone gemifloxacin or injectable gentamicin.4
References
Mahon, C. R., & Lehman, D. C. (2019). Textbook of diagnostic microbiology. Elsevier Saunders.
Ogun, A. S. (2021, July 31). Biochemistry, transferrin. StatPearls [Internet].
Centers for Disease Control and Prevention. (2014, January 29). Std facts – gonorrhea.
Mayo Foundation for Medical Education and Research. (2021, October 5). Gonorrhea.
Cheng, A., & Kirby , J. (2014, March). Evaluation of the hologic gen-probe panther, APTIMA Combo 2 assay in a tertiary care teaching hospital. American journal of clinical pathology.
-Alejandro Soto, MLS(ASCP)CM
-Phyu M. Thwe, Ph.D., D(ABMM), MLS(ASCP)CM is Microbiology Technical Director at Allina Health Laboratory in Minneapolis, MN. She completed her CPEP microbiology fellowship at the University of Texas Medical Branch in Galveston, TX. Her interest includes appropriate test utilization and extra-pulmonary tuberculosis.
A 35 year old male with a history of alcohol use disorder in early remission, acute alcoholic hepatitis with multiple admissions for worsening liver function was admitted for acute kidney injury and worsening encephalopathy. Blood cultures were collected due to leukocytosis and the anaerobic bottle flagged positive for gram negative bacilli at 4.6 days. The organism, shown in Image 1, was sent to a reference laboratory and was identified as a Campylobacter species, unable to further identify. The patient will receive a liver transplant at another institution.
Image 1. Campylobacter species morphology in a blood smear.
Discussion
Campylobacter species are gram-negative, oxidase-positive, non-fermenting, microaerophilic, non-spore forming, motile rods typically with one or more helical turn.1,2 When two bacteria form short chains, these appear as “S” shaped and/or “gull-wing” shaped. These bacteria are generally 0.2 µm by 0.5-5.0 µm in size and can be as long as 8.0 µm.1Campylobacter species are widely distributed in most warm-blooded animals (e.g., poultry, cattle, pigs, sheep, cats, and dogs) and they grow optimally at 37-42 °C. There are more than 20 Campylobacter species, not all of which cause illness but are potentially pathogenic. Campylobacter jejuni accounts for approximately 90% of human Campylobacter infections, while less common species such as Campylobacter coli, Campylobacter upsaliensis, Campylobacter fetus, and Campylobacter lari can also cause infection.3
Transmission of Campylobacter is believed to be foodborne via undercooked meat (particularly poultry), unpasteurized milk, or improperly treated water. Person-to-person transmission is rare, but may occur via the fecal-oral route. The infection load for Campylobacter species is relatively low, with fewer than 500 organisms causing infection.4 In human infection, these bacteria usually colonize the intestinal tract leading to diarrhea (often bloody), stomach cramps, fever, nausea, and vomiting.5 Clinical manifestation usually occurs 2 to 5 days after the individual is infected and lasts approximately a week. Diagnosis is established definitively by stool culture and sometimes by blood culture.2 In some cases, long-term effects of Campylobacter infection include an array of clinical syndromes including enteritis, bacteremia, arthritis, septic abortion, meningitis, irritable bowel disease, and Guillain-Barre syndrome [4]. Individuals with a greater risk for infection include those 65-years or older, pregnant women, and those with weakened immune systems.5
Campylobacteriosis is the most common form of acute infectious diarrhea in developed countries with a higher incidence than both Salmonella and Shigella.1 The Center for Disease Control and Prevention estimates that 1.5 million people in the United States are affected by Campylobacter infection each year—making it the most common bacterial cause of diarrheal illness in the United States.3 Unfortunately, the incidence of hepatitis associated with Campylobacter species infection is unknown, as few case-reports related to Campylobacter colitis6and Campylobacter jejuni 7,8,9,10 have been published. Although the liver is often involved in systemic infections resulting in various types of abnormal liver function tests, mild to severe hepatocellular dysfunction is an uncommon observation in those with Campylobacter infection.
Most individuals infected with any Campylobacter species recover with only fluid replenishment while the diarrhea lasts and no antibiotic treatment. However, those with or at risk for severe illness should be considered for antibiotic treatment. The antibiotics that are used to treat infection are azithromycin and fluoroquinolones (usually resistant). Antimicrobial susceptibility testing can help guide appropriate therapy.3
Centers for Disease Control and Prevention. Campylobacter (Campylobacteriosis) For Health Professionals [Internet]. 2019 [updated December 23, 2019]. Available from: https://www.cdc.gov/campylobacter/technical.html.
Yoon JG, Lee SN, Hyun HJ, Choi MJ, Jeon JH, Jung E, et al. Campylobacter jejuni Bacteremia in a Liver Cirrhosis Patient and Review of Literature: A Case Study. Infect Chemother. 2017;49(3):230-5. Epub 2017/06/14. doi: 10.3947/ic.2017.49.3.230. PubMed PMID: 28608661; PubMed Central PMCID: PMCPMC5620392
-Amelia M. Lamberty is a MS in Pathology student at the Larner College of Medicine at the University of Vermont.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
The lab technologist approached the Lab Safety Officer to ask what should be done with a collection of liquid wastes that were collected from the chemistry analyzers. The LSO had worked with multiple labs for years helping to determine how to dispose of their liquid chemical wastes according to the regulations. He thought he was pretty well aware of the hazardous chemical wastes coming from the labs, but he had no idea this chemistry analyzer waste existed. He dug a bit deeper. As he called around to the different labs in the system, he learned not all sites were handling the waste the same way. Some sites saved the excess waste and poured it into other containers to use on the analyzers. Some labs threw the containers in the trash with liquid inside, and other sites simply poured the excess chemicals down the sink drain.
Some laboratories and lab systems are very large, and there are probably many practices, some newer, some older, that have developed over time, because “someone said so,” or because a vendor said it was acceptable. The LSO may not always be able to know about every practice in each lab. Staff should always escalate questions about waste processes when there is a concern.
Managing hazardous (chemical) wastes is a complicated process, and training and education is needed in all laboratories. The regulations surrounding waste are numerous and complicated, and it would be unlikely that every lab employee would aware of all of them. Here are some basics that are true for all laboratories:
Pouring Bulk Wastes Down the Drain is (Usually) Incorrect and Possibly Illegal
In general, manually pouring bulk amounts of chemical waste down the drain is not permitted by the EPA. What is a bulk waste? It is defined as 200 mL or more. That means if you have >200 mL of a reagent left over in a container, you cannot pour it down a drain for disposal. That chemical is now waste and must be properly collected, labeled, and stored until a waste contractor can pick it up.
There are, of course, exceptions to every rule. If a waste drain line is connected to a drain, for example, that is not considered “pouring,” and it is acceptable provided a lab has informed the local wastewater treatment center about what is going down the drain. Performing a gram stain in microbiology and letting the residual chemicals go down the drain is allowed also. That is considered part of the gram stain process, and it is not viewed as “pouring” chemicals down the drain. Also, the wastewater facility is aware that these chemicals are going down the drain.
Another exception exists in some laboratories that have an external “chemical pit” which is tied to certain sinks and drains in the lab. That means that all wastes poured down these drains go straight to a collection tank which neutralizes the chemicals. The tank is emptied periodically by a contracted vendor. Since there is no waste going to the local wastewater system, the local authority does not need to be contacted about what goes down the lab drains.
Hazardous Waste Must be Properly Stored
Anytime a lab collects chemical waste, it must be properly stored. There are two types of waste storage areas, Satellite Accumulation Areas (SAA) and Central Accumulation Areas (CAA). A Satellite Accumulation Area is a storage area near to where the waste is generated. The SAA must be within the line of sight of where the waste is made, it cannot be in another room or around the corner. You must store the waste where it can be seen from where it was generated. You cannot move waste from one SAA to another SAA. You can. However, move waste from a SAA to a Central Accumulation Area (like a hazardous waste shed outside, for example).
SAAs can store up to 55 gallons of waste. Waste must be stored inside of a flammable cabinet if it is flammable, and acid wastes cannot be stored next to bases. SAAs and CAAs must have a specific emergency contact poster hung nearby which indicates the location of the nearest fire extinguisher as well as an emergency contact in case of a spill or accident. CAAs must be checked weekly for proper labeling, open containers, and leaking, and these checks must be documented.
Hazardous Waste Must be Properly Labeled
Anytime a lab collects chemical waste, it must be properly labeled per EPA regulations. All waste containers must be labeled with the identity of the contents and the words “Hazardous Waste.” There must also be an indication of the waste hazard(s), such as a pictogram or an NFPA diamond. If waste is collected into an empty reagent jug, you may not use the wording or warning label from the original jug.
Dates should never be placed on chemical waste labels when stored in a Satellite Accumulation Area, but dates always need to be on containers once moved to the Central Accumulation Area. If the waste vendor picks up containers directly from your SAA, you never need to place dates on the containers.
Again, the proper management of the laboratory hazardous wastes is complicated. There is a great deal to learn and to put in practice. Many regulations have exceptions, and some of them depend on the facility’s waste generator status. If you have questions, reach out to your EPA (or state branch) representative, or ask an available safety expert. Make sure your lab is handling chemical wastes appropriately and safely.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Leukemic Reticuloendotheliosis (LRE) is a term that was first used in 1923 but is a name that most of us would not recognize today. In 1958, Bournocle et al. published a paper that characterized LRE as a separate clinical disorder and described the clinical course, pathologic features, treatment options and prognosis. The study also described an unusual morphology of the malignant cells seen in this condition. The malignant cells were noted to be small mononuclear cells with projections around the circumference of the cytoplasm. Another decade went by before these cells were given the nickname “hairy cells”. At the time, though LRE was considered a fatal disease, splenectomy appeared to be a beneficial treatment, thus pointing to a lymphocytic disorder. Later, in 1976, an article was published that suggested that these hairy cells were monocytic rather than lymphocytic in origin. The true lineage of these hairy cells was unknown until the development of newer immunophenotypic methodologies in the mid to late 1970s. Today, hairy cell leukemia (HCL) is considered a rare, chronic B cell leukemia that comprises 2% of lymphoid leukemias and responds well to therapy.
Patients may be entirely asymptomatic at diagnosis, and the finding of hairy cells on the peripheral smear from a routine CBC prompts further investigation. Patients do not usually require treatment at diagnosis, and many patients live a normal lifespan. Originally, diagnosis was based on clinical and laboratory result correlation: CBC results, observation of the characteristic hairy cells, and splenomegaly. One of the first tests used for diagnosis of HCL was tartrate-resistant acid phosphatase activity (TRAP stain). Today, standard practice is immunophenotyping by flow cytometry. HCL is characterized by the expression of B-cell antigens CD19, CD20, and CD22 in addition to bright CD11c expression with CD103, CD25, CD123 and Annexin A1 (ANXA1) co-expression. Annexin A1 is the most specific immunohistochemical marker for HCL. In 2011, the BRAF-V600E mutation was identified as the genetic causal event of HCL, allowing even more advances in the diagnosis and therapy for HCL.
As the disease progresses, most patients experience increasing cytopenia, including monocytopenia, and persistent splenomegaly. Treatment is usually started when a patient meets certain guidelines, which include a severe cytopenia or pancytopenia, malignant lymphocytosis, increased susceptibility to infection or symptomatic splenomegaly. Historically, the only available treatment was splenectomy. In the 1980’s, interferon therapy was introduced and was able to induce partial responses in some patients. In the 1990’s the purine analogs, cladribine or pentostatin, became available as the preferred first line treatment for HCL. Treatment response is good and offers prolonged remission rates. For patients who experience relapse, rituximab may be used in combination with a purine analog. Most recently, anti-CD22 immunotoxins and molecular targeted therapy with BRAF inhibitors have been introduced for cases that do not respond to other therapies.
Additional discoveries into the biology of the disease have identified new subtypes of HCL. It is important to distinguish between classic HCL and Hairy Cell leukemia variant (HCLv) because they are treated differently. HCLv may be more aggressive and does not respond well to purine analogs alone. HCLv is often diagnosed at older age than classic HCL In HCLv the WBC is often elevated, with lymphocytosis, and there is a lack of monocytopenia. The hairy cells seen on a peripheral blood smear may be more abundant than in classic HCL. These HCLv cells also often have a distinct nucleolus not seen in HCL cells. As well, these cells can have a morphology that appears to be somewhere between prolymphocytes and hairy cells. Unlike HCL, HCLv cells are negative for CD25 and BRAF-V600E. HCLv represents only about 10% of HCL cases. Because of its rarity, and the gray areas surrounding differential diagnosis between HCL and HCLv, studying these rare cases can help lead to a better understanding and management of both HCL and HCLv patients.
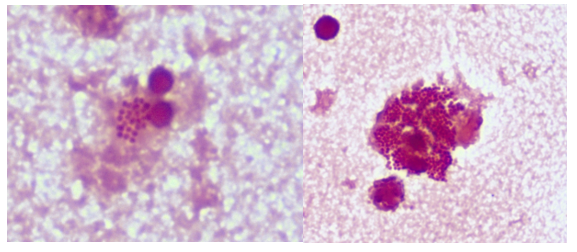
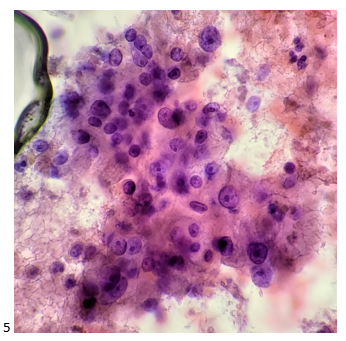
About 1200 new cases of HCL are diagnosed each year in the US. HCL is 4-5 times more common in males, with a median age at diagnosis of 55-60. This is an unusual case because the patient is female, was older at diagnosis, with no cytopenia or splenomegaly noted. This patient is a 79-year-old female who, one year ago, was referred to a Hematology Oncology practice with a several year history of a mildly elevated WBC with increased lymphocytes, without absolute lymphocytosis. She was referred after a peripheral smear exhibited prolymphocytes and the “hairy’ appearing lymphocytes shown below in Image 1.
Image 1. Hairy Cells seen on peripheral blood smear.
Peripheral blood was sent for myeloid/lymphoid disorders and acute leukemia analysis by flow cytometry. Remarkable in this case were the results of the flow cytometry studies. Flow cytometry performed on the peripheral blood revealed 2 distinct morphological populations of lymphocytes. The majority of lymphs appeared to be small, with scant cytoplasm, round nucleus, clumped chromatin, and inconspicuous nucleoli. These cells were identified as a monoclonal kappa restricted B cell population exhibiting co-expression of CD23 and CD5, consistent with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL). A second population of lymphs were larger, with more abundant granular cytoplasm and hairy projections, large nuclei, condensed chromatin, and inconspicuous nucleoli. This second population displayed CD20 expression and was positive for CD11c, CD103 and FMC-7. CD25, CD5 and CD23 were negative.
The immunophenotyping of this second population of cells suggests a diagnosis HCL; or is it suggestive of HCLv? The patient was older at diagnosis, leukocytosis and lymphocytosis are present, and monocytopenia is absent. Hairy cells were over 8% of the differential, though lacking the distinct nucleoli of HCLv. Prolymphocytes were noted. CD25 was negative in this patient and is usually exhibited in HCL.
An immunological scoring system for HCL has been proposed with one point given to each of markers for CD11c, CD103, CD123 and CD25. One point is given if the marker is expressed and no point when it is not expressed. A score of 3 or 4 is observed in 98% of cases of HCL and is usually 0-1 in other HCL-like disorders. This patient’s cells showed expression of CD11c and CD103, was CD25 negative and CD123 was not evaluated so would score at least a 2, which puts her somewhere in an inconclusive score. Additionally, a bone marrow biopsy has not been done and there therefore results for TRAP or annexin A1 immunostaining, or BRAF-V600E mutations are not available.
With a diagnosis of a B-lymphocytosis consistent with CLL/SLL and a simultaneous HCL, or HCLv, this patient is an interesting case. Several articles and reviews in literature of other patients with CLL and HCL give further insight into the biology of HCL. Literature suggests that concurrent HCL and CLL may indicate a common origin. Patients with HCL may subsequently develop CLL, which can mimic a relapse of HCL. Therapy requires treating each case individually and watchful waiting in asymptomatic cases. Rituximab with or without purine analogs have been useful to treat both disorders simultaneously.
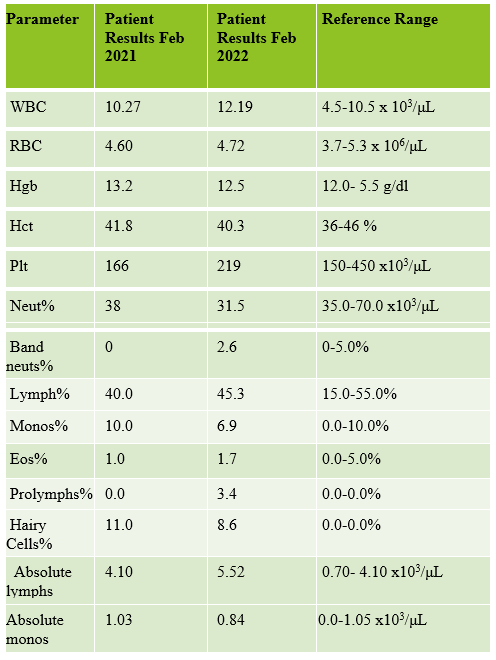
Table 1. CBC results from a patient in 2022 and 2022.
This patient at 1 year following diagnoses has developed a mildly increasing lymphocytosis and is being monitored. Both her CLL/SLL and HCL still appear to be in the indolent, “wait and see” stage. The patient has declined further workups at this time.
References
Bain, Barbara J. Blood Cells: A Practical Guide. 5th ed. Wiley Blackwell, 2015. Print.
Chang-Hun Park, Hyun-Young Kim, M.D.et al. Efficacy of Annexin A1 Immunostaining in Bone Marrow for the Diagnosis of Hairy Cell Leukemia. Laboratory Medicine Online 2019; 9(4): 236-241
Falini B, Tiacci E. New treatment options in hairy cell leukemia with focus on BRAF inhibitors. Hematol Oncol. 2019; 37(Suppl. 1): 30– 7..Maitre, E.; Cornet, E.; Troussard, X. Hairy cell leukemia: 2020 update on diagnosis, risk stratification, and treatment. Am. J. Hematol. 2019, 94, 1413–1422.
Obiorah IE, Francischetti IMB, Wang HW, Ahn IE, Wang W, Raffeld M, Kreitman RJ, Wiestner A, Calvo KR. Concurrent chronic lymphocytic leukemia/small lymphocytic lymphoma and hairy cell leukemia: clinical, pathologic and molecular features. Leuk Lymphoma. 2020 Dec;61(13):3177-3187.
Scheinberg M, Brenner AI, Sullivan AL, Cathcart ES, Katayama I. The heterogeneity of leukemic reticuloendotheliosis, “hairy cell leukemia”. Evidence for its monocytic origin. Cancer. 1976 Mar;37(3):1302-7
Shao, Haipeng et al. “Distinguishing hairy cell leukemia variant from hairy cell leukemia: development and validation of diagnostic criteria.” Leukemia research vol. 37,4 (2013)
Verma V, Giri S, Bhatt VR, Amador-Ortiz C, Armitage JO. Synchronous or Metachronous Hairy Cell Leukemia and Chronic Lymphocytic Leukemia: A Case Series and Literature Review. Front Oncol. 2017 Jan 9;6:270.
X. Troussard, M.R. Grever. The revised guidelines for the diagnosis and management of hairy cell leukaemia and the hairy cell leukaemia variant. r J Haematol, 193 (1) (2021), pp. 11-14
-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.