I’ve mentioned before how important it is to know clinical history before attending a biopsy, and I cannot stress this point enough. As the first line of screening, the intermediary between clinician and pathologist, the role of the cytologist is to prepare, assess, and convey. In a cancer center, we have three main populations: the patients with the unknown primary, the patients with the suspected primary, and the patients with the suspected metastasis. In the event of a suspected metastasis, we’ll review previous relevant pathology material if we have it onsite. Unless the clinician is requesting additional prognostic markers, the review process helps us eliminate the unnecessary repetition of immunostains (IHC) by confirming that the current material is morphologically consistent with the prior material. Sometimes we still perform old-school cytology without a plethora of ancillary studies. HA!
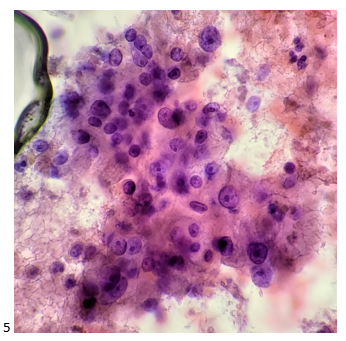
Most of the endobronchial ultrasound (EBUS) procedures performed at our institution are for lung cancer staging or differentiation between a lung cancer metastasis and an extra-pulmonary metastasis. Not that we don’t see the occasional sarcoid- or anthracosis-related process from time to time, but our most common indication is cancer. For an 88-year-old male patient with multiple lung nodules and both mediastinal and hilar lymphadenopathy, confirmation of metastasis was the main objective of the EBUS procedure. The patient’s pertinent medical history includes former tobacco use, squamous cell carcinoma of the lung (diagnosed percutaneously in 2022), clear cell renal cell carcinoma (s/p partial nephrectomy in 2020), prostate cancer (radiated in 2007), melanoma (excised in 2001), and cutaneous squamous cell and basal cell carcinoma (also previously excised in 2002 and 2008). With an extensive cancer history, the lung nodules and thoracic nodes could be any of them, although metastatic squamous cell carcinoma of the lung was clinically favored. My awesome cytologist colleague, Kelly, attended the EBUS procedure. The Rapid Onsite Evaluation (ROSE) was a clear-cut “adequate for diagnostic material,” and the attending pathologist added “tumor cells present.” The following morning, Kelly stopped by my desk to ask my opinion of the 12R (right hilar) lymph node she was screening. She said, “look at my dots. Do these look like the same cells to you? Or are they different? Because I feel like they’re different.” Before putting the slide on my scope, I asked, “so… like a combined adenosquamous? Or a small cell component?” She replied, “not small cell. Something… I don’t know, but they look different. The patient was recently diagnosed with lung cancer and has a history of renal cell.” I fixated on the H&E cell block slides (Images 1-3) before perusing the Diff-Quik and Papanicolaou-stained slides (Images 4-5). “Uhm… Why are there two different types of tumor cells here?! The cytoplasm here is so… vacuolated, but it’s not quite like lung adeno, and the other group… even the n/c (nuclear-to-cytoplasmic) ratio is different. What is this?” Kelly replied, “okay, so there are definitely two different types of tumor here.” I looked up, “It has to be. Absolutely, yes.”

Kelly entered her diagnosis into our laboratory information system and brought the case over to the pathologist on cytology service for the day. She explained her thought process, and the pathologist also questioned if it was a combined process, such as a lung adenosquamous and maybe the original lung biopsy only sampled the squamous component. With the most recent clinical history of both lung squamous cell carcinoma and clear cell renal cell carcinoma, an IHC panel was appropriately selected. Later that afternoon, the pathologist exclaimed, “IT’S BOTH! IT’S SQUAMOUS AND RCC!” The clusters of squamous cell carcinoma did not stain for PAX8 (a renal cell carcinoma marker) (Image 6), and the same cluster stained positive for p40 (a squamous cell carcinoma marker) (Image 7). Within the same level of the cell block, the cluster of cells that appeared morphologically different than squamous cluster stained positive for PAX8 (Image 8) and negative for p40 (Image 9), confirming a renal cell carcinoma component. A small focus of p40-positive cells was present next to the p40-negative renal cell carcinoma (Image 9), further demonstrating mixed histology. This finding was shared with other pathologists, and the results were immediately called to the pulmonologist as this was a critical finding. Sometimes we encounter a partially involved node where the tumor cells are intermixed with lymphocytes, sometimes the lymph node yields more tumor than the primary site, and sometimes, albeit rarely, we encounter a lymph node infiltrated by two different carcinomas.

Due to the patient’s bulky disease and PD-L1 expression of 30%, the medical oncologists primary aim was to treat the squamous cell carcinoma first and follow up renal cell carcinoma therapy second. After the first few cycles of treatment, the lung nodules have decreased in size, but the thoracic nodes remain unchanged. Once the squamous cell carcinoma is controlled or demonstrates a more significant response, immunotherapy may be added to target both, with a tyrosine kinase inhibitor directed at renal cell carcinoma metastases in the event of progression.

-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
