Just in time for Halloween: a recently-published study in mBio discusses the 2014 outbreak of Listeria monocytogenes tied to caramel apples. There’s not enough water in caramel and an apple is too acidic to support this bacterium, so how did this outbreak occur? From the study: “Our findings suggest that the 2014 listeriosis outbreak associated with caramel-coated apples can be explained by growth of L. monocytogenes occurring at the interface between two foods which, by themselves, are inhibitory to pathogen growth.”
Author: Lablogatory
Microbiology Case Study–An 18 Year Old Pregnant Woman with Nausea and Vomiting
Case history:
An 18 year old pregnant woman at 16 weeks gestation presented at the emergency department with nausea and vomiting for 3 days. Three days ago she and some of her friends ate chicken at a party. None of her friends experience her symptoms. Laboratory tests revealed urinary tract infection and a stool sample was sent to the microbiology laboratory for culture.
She was prescribed an antibiotic and was released from the ED.
Laboratory identification:
The organism grew well on MacConkey agar, and formed small colorless lactose-negative colonies. Gram stain revealed short gram-negative bacilli and MALDI-ToF confirmed the bacteria as Yersinia enterocolitica.
Discussion:
Yersinia enterocolitica is a gram negative, short, non-spore-forming bacillus in the family Enterobacteriaceae. They can exhibit bipolar staining, especially from the primary sample. It is a facultative anaerobe can grow at temperatures ranging from 4-43oC that is motile at room temperature but non-motile at 37oC. The organism grows well on MacConkey agar, and forms small colorless lactose-negative colonies but if the clinical team is suspicious for Yersinia, a selective growth medium is recommended. The most widely used is cefsulodin-irgasin-novobiocin (CIN) agar, which inhibits the growth of competing flora and produces characteristic colony morphology (red color with “bull’s eye” appearance).
The major route of Y. enterocolitica infection is through contaminated foods or water. The primary pathogenic event is colonization of the intestinal tract where most of the pathologic effects and clinical manifestations occur. Temperature and calcium concentration regulate expression of virulence factors that guide the invading Yersinia and allow them to survive and disseminate.
The most common form of disease caused by Y. enterocolitica is gastroenteritis associated with consumption of contaminated food or water, especially raw or undercooked pork such as chitterlings. Disease can range from self-limited gastroenteritis to terminal ileitis and mesenteric lymphadenitis that can be misdiagnosed as appendicitis. Gastrointestinal infections are usually self-limiting and do not merit antimicrobial therapy. However, in immunocompromised hosts and in patients with septicemia or invasive infection, the mortality can be high (approximately 50%).
Kossivi Dantey, M.D. is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.

–Christi Wojewoda, MD, is certified by the American Board of Pathology in AP/CP and Medical Microbiology. She is currently the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Antimicrobial Testing–Are We Doing it Wrong?
Antibiotic resistance is a huge concern for microbiologists. In addition to stewardship programs and regulating agricultural use of antibiotics, is it time to re-examine clinical testing paradigms?
A recent study suggests that the typical way microbiologists test for antibiotic susceptibility–meuller-hinton plates and antibiotic disks–might be fallible. When his team tested Salmonella against polymyxin using typical methods, the organism tested sensitive; when the tested the same organism against the same antibiotic using medium that more closely resembled human cells, the organism tested resistant.
Bloomberg Business discusses the paper here. The article is worth your time, even if the info-graphic gives erroneous information (it mentions meuller-hinton broth instead of meuller-hinton agar plates).
Ammonia and Hyperammonemia
Ammonia is a small molecule that is produced as a part of normal tissue metabolism. Its formation results from the breakdown of compounds containing nitrogen, such as the amino groups in proteins and the nitrogenous bases in nucleic acids. In the tissues, ammonia is stored mainly in the form of amino acids, specifically the amino acid glutamine which has three amino groups. Normally, the body can remove excess ammonia easily via the liver pathway known as the urea cycle. This short, 4-step cyclical pathway converts two ammonia molecules into a small, water soluble urea molecule, making it able to be easily excreted in the urine. Without a functional urea cycle however, the body has no other adequate mechanism for getting rid of the ammonia that is constantly being produced by metabolism.
Liver damage or disease can disrupt the urea cycle, causing blood ammonia levels to rise. This is the most common cause of elevated ammonia in the adult population. In a pediatric patient, elevated ammonia is frequently seen as a consequence of an inborn error of metabolism (IEM). Many IEM, especially those in the urea cycle pathway, will result in elevated blood ammonia levels. In addition, in IEM causes, the ammonia concentrations may be well over 1000 µmol/L, when the normal range of ammonia is generally in the 30 – 50 µmol/L range. Elevated blood ammonia concentrations are serious because ammonia is toxic to the brain. The higher the ammonia concentration is, and the longer it stays high, the more brain damage that will occur.
Interestingly, the concentration of ammonia in the blood may not correlate with the neurological symptoms that are seen. Usually if the ammonia concentration is <100 µmol/L, the person will show no symptoms at all. Concentrations of ammonia in the 100 – 500 µmol/L range are associated with a wide variety of symptoms including: loss of appetite, vomiting, ataxia, irritability, lethargy, combativeness, sleep disorders, delusions and hallucinations. These patients may present with an initial diagnosis of altered mental status, and if there is no reason to suspect an elevated ammonia, the symptoms may lead to drug or alcohol testing. When ammonia concentrations are >500 µmol/L, cerebral edema and coma may be seen, with cytotoxic changes in the brain. Ammonia concentrations in the 1000+ µmol/L range are extremely critical and are treated aggressively with dialysis to pull the ammonia out of the system. In particular, urea cycle defects require close monitoring of ammonia and glutamine concentrations, with immediate response when they rise.
Laboratory testing for ammonia is often problematic as contamination can occur from a number of sources including atmospheric ammonia, smoking and poor venipuncture technique. In addition if the sample is not centrifuged and analyzed promptly, ammonia is formed by the continuous deamination of amino acids and the concentration increases by 20% in the first hour and up to 100% by 2 hours. Consequently samples to be tested for ammonia should be placed on ice immediately after being collected and transported to the lab for analysis as soon as possible. Many minimally elevated ammonia results are a consequence of poor sample handling. However, a truly elevated ammonia is a critical lab finding that should be addressed immediately.

-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.
You Make the Diagnosis: a 32-Year-Old with Mild Jaundice
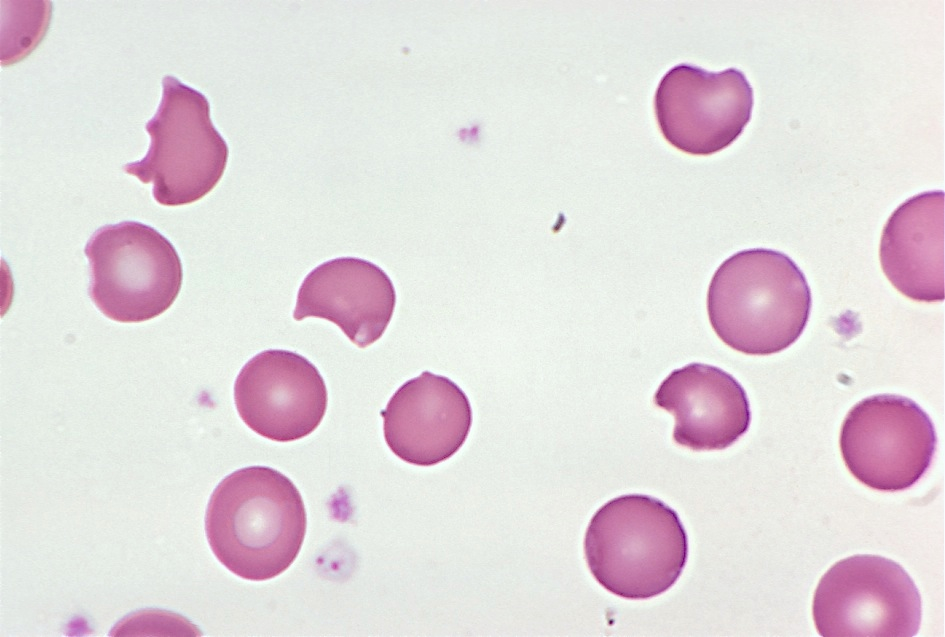
A 32-year-old male presents with mild jaundice and flank pain. He recently developed sinusitis, which was treated with trimethoprim-sulfamethoxazole, but is otherwise healthy. His hemoglobin is 10.2 g/dL (13.5-17.5), MCV is 90 μm3 (80-100), and total bilirubin is 3.4 mg/dL (0.2-1.5). A representative field from his blood smear is shown here. What is the most likely diagnosis?
- Aplastic anemia
- Iron-deficiency anemia
- Glucose-6-phosphate dehydrogenase deficiency
- Autoimmune hemolytic anemia
- Megaloblastic anemia
The answer is glucose-6-phosphate dehydrogenase (G6PD) deficiency. G6PD deficiency is an X-linked recessive disorder in which patients produce decreased amounts of G6PD, a red blood cell enzyme involved in detoxifying free radicals.
When a patient with G6PD deficiency is exposed to an oxidant stress (which can be anything from an illness to ingestion of certain foods or drugs), the resulting reactive oxygen species attack structures within the red cell.
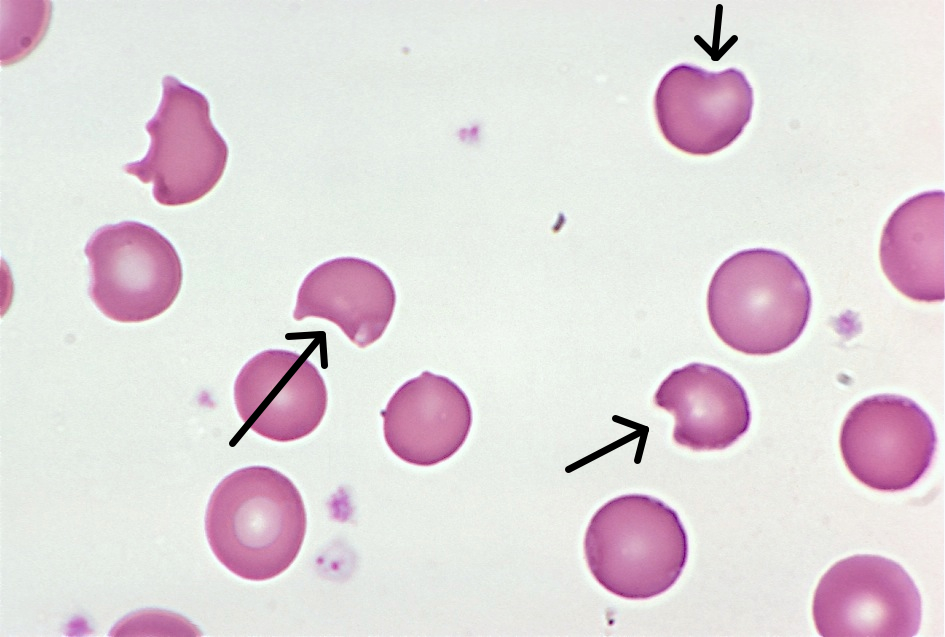
Globin chains are particularly vulnerable to oxidant damage. They become denatured and stick to the inside of the red cell membrane, forming inclusions called Heinz bodies, which are visible on crystal violet staining. Heinz bodies are removed by macrophages in the spleen, leaving visible “bites” in the red cells. Several bite cells are visible in this patient’s blood smear (arrows).
Most episodes of hemolysis in patients with G6PD deficiency resolve on their own after the offending substance is removed.

-Kristine Krafts, MD, is an Assistant Professor of Pathology at the University of Minnesota School of Medicine and School of Dentistry and the founder of the educational website Pathology Student.
Microbiology Case Study: An 8-Week-Old Female with Pallor, Vomiting, Fever, and Blue Feet
Clinical History
An 8 week old female was brought to an outside hospital due to pallor, decreased eating over several days, vomiting, fever, and blue color in the feet. The patient had received her two month vaccinations the day prior to presentation. Her past medical history was significant for being born at 32 weeks gestation, followed by an uneventful 4 week NICU stay. At the outside hospital the patient was in respiratory distress, tachycardic, with pallor. She was intubated and transferred to our institution due to concern for an ALTE (apparent life-threatening event). Blood and CSF specimens were drawn. Upon presentation, the patient had a white blood cell count of 19,600/mm3. Her CSF had 63 nucleated cells/mm3 (30% neutrophils, 49% lymphocytes, 11% monocytes), glucose of 23 mg/dL and protein of 212 mg/dL. Blood and CSF cultures were performed with the following results:
Laboratory Identification
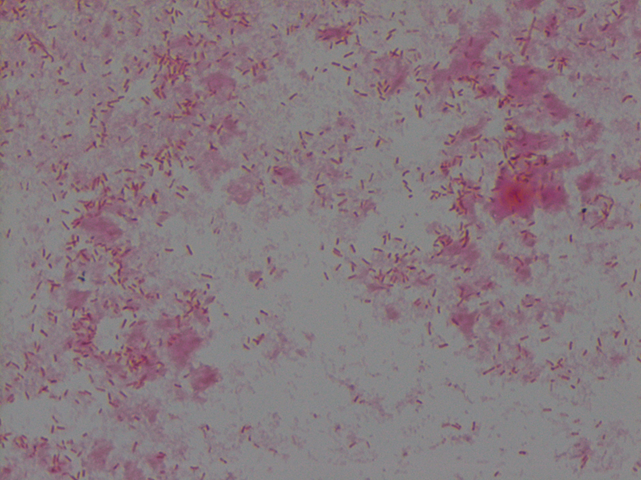
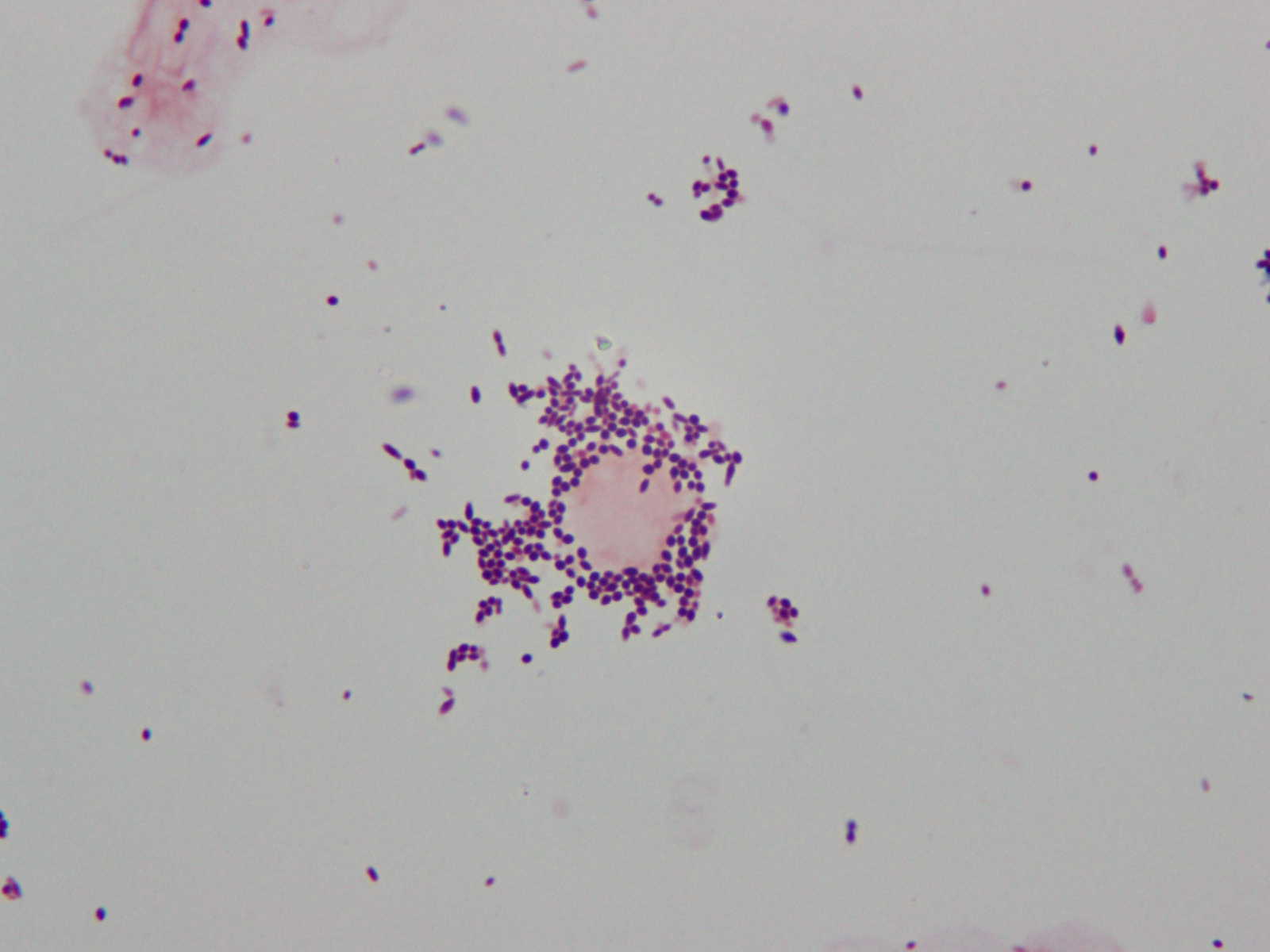
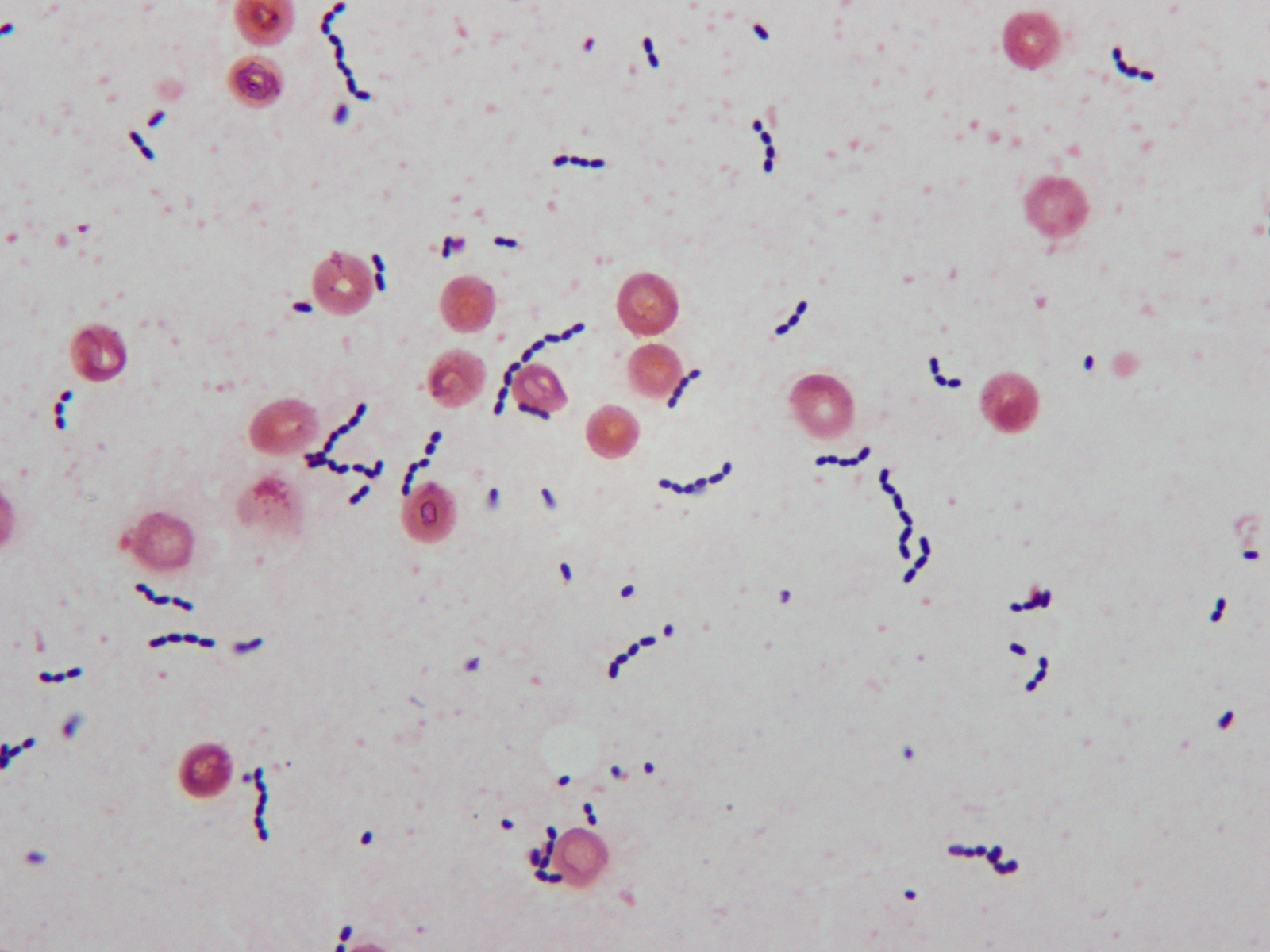
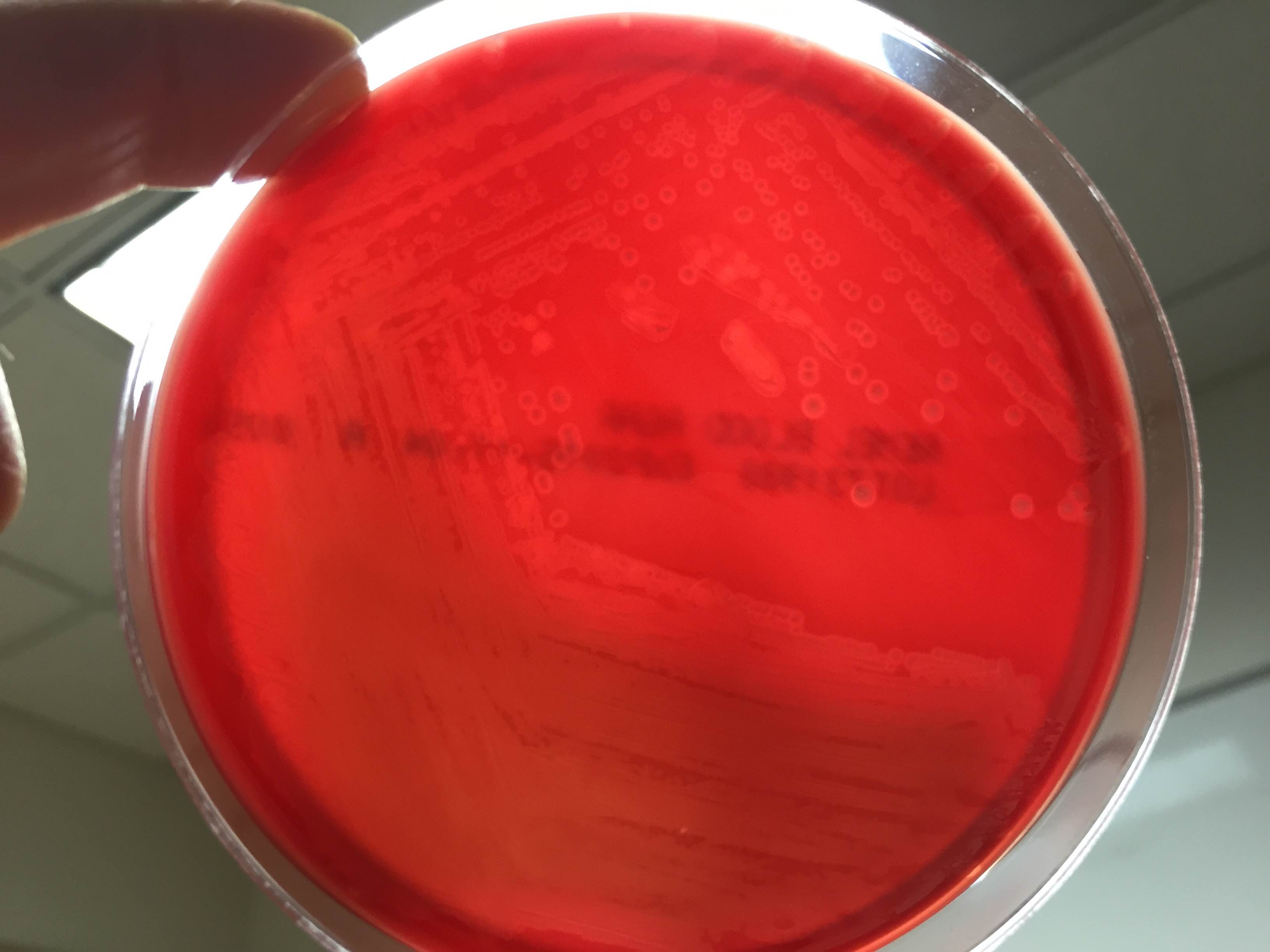
CSF Gram stain was read as many Gram-variable coccobacilli (Image 1) and blood culture Gram stain was resulted as Gram-positive cocci in pairs and chains (Image 2). The Nanosphere Verigene Gram-positive blood culture molecular assay was performed on the positive blood culture broth immediately following Gram staining. CSF and positive blood culture specimens were plated to 5% sheep blood, chocolate, MacConkey, and CNA agars. In >24 hours colonies from both specimens grew a single organism on sheep blood, chocolate, and CNA agars. On blood agar, colonies exhibited a soft zone of b-heomlysis (Image 3). Colony Gram stains showed Gram-positive cocci in chains, catalase testing was negative, and the organism typed in Lancefield antigen group B. Verigene identified the organism directly from the positive blood culture broth as Streptococcus agalactiae (aka Group B Streptococcus or GBS) and MALDI-TOF mass spectrometry confirmed the identification of S. agalactiae.
Discussion
Laboratory Considerations
As our CSF specimen demonstrated, streptococci can be difficult to interpret from specimen Gram stains. Organisms are often are pleomorphic in size and shape and they have a tendency to stain Gram-variable. This lead to the report of Gram-variable coccobacilli on our patient’s CSF culture.
S. agalactiae produces a soft zone of b-heomlysis on sheep blood agar. Unlike Streptococcus pyogenes (aka Group A Streptococcus) which produces a wide zone of b-hemolysis, soft b-hemolysis can often be very subtle, especially with young growth. Soft zones b-hemolysis can best be seen by holding plates up to a light source or my moving a colony out of the way to observe if hemolysis is present underneath. The pattern of S. agalactiae b-hemolysis is very similar to that produced by Listeria monocytogenes. Streptococcal isolates that type as Lancefield Group B, but produce large zones of b-hemolysis can create confusion and are most likely not S. agalactiae, but S. porcinus or S. pseudoporcinus.
Clinical Significance
S. agalactiae is the cause of significant neonatal disease. Early-onset infection presents as systemic infection, respiratory distress, apnea, shock, and pneumonia within the first 24 hours of life (range, 0–6 days). Meningitis is less common in early-onsetS. agalactiae infections, found in just 5-10% of cases. Late-onset disease presents at 3 to 4 weeks of age (range, 7–89 days) as meningitis and/or sepsis with other focal infection. Approximately 50% of survivors of early- or late-onset meningitis have long-term neurologic sequelae.
S. agalactiae colonizes the urogenital or gastrointestinal track of 10-30% of pregnant women. Being born to a S. agalactiae colonized mother is the most significant risk factor for development of disease in neonates. For this reason, women are screened for “Group B Strep” colonization between 35 and 37 weeks of pregnancy. Women found to be colonized receive prophylactic antibiotics immediately prior to delivery to prevent transmission to the child. Since implementation of these practices in 1996, there has been a substantial decline in early-onset S. agalactiae infections. Interestingly, these measures have not affected the incidence of late-onset disease.
Treatment
Until recently S. agalactiae was considered universally susceptible to penicillin. There have now been a few reports of S. agalactiae isolates with increased penicillin MICs due to mutations in the penicillin binding protein Pbp2x. The detection of these isolates is still extremely rare, so much so that S. agalactiae susceptibility testing for penicillin and other b-lactams is not considered necessary at this time. Penicillin and its derivatives are the preferred treatment option.
Patient follow-up
Our patient had a complicated course of late-onset Group B Streptococcal meningitis including multifocal cerebral infarctions and seizures. She was treated with a 28 day course of ampicillin. Blood cultures taken 24 hours after the start of antibiotics were negative and her CSF culture was negative when rechecked 5 days after her presentation. Due to her complicated course, the patient was hospitalized for 4 weeks. Follow-up appointments have shown the patient’s MRI is nearly normal 8 weeks post infection and the patient is doing well, although she is still followed by neurology to assess for long term sequelae.
Our patient’s mother had an unknown Group B Strep carrier status at the time of her birth, as she was born at 32 weeks, which is before routine screening occurs for pregnant women. Either way, the mother’s status would not have affected the patient’s risk for late-onset Group B Streptococcal infection.
References:
- Red Book 2015
- Journal of Clinical Microbiology, 10th edition

-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
The Path to Molecular Diagnostics – MB(ASCP) Certification
While I have been working in the field of all things “Molecular” for close to twelve years, it wasn’t until early this year that I decided to actually sit for the ASCP certification exam in Molecular Biology. With over five years working in research and currently going on seven years in a clinical lab, I was feeling pretty confident about my knowledge and background, but then panic set in. Would I be able to pass a test? I haven’t taken an exam since my final years of college! I have two young children who are extremely active in extracurricular activities, a husband who also works full time. Needless to say, any extra time I had for myself would be spent studying. It didn’t take long to find out that while there was a very general outline of topics covered and an extensive list of textbooks to serve as a starting point, there were not specific details on where to focus my efforts. There was no single study guide, no tangible tools I could utilize to make exam preparation fit into my busy life any easier.
Fast forward to the present, where all of the panic was for not. In February I did pass (with flying colors) and happily sport MB (ASCP)CM after my name. When I was recently approached about writing on a regular basis for Lablogatory, I knew it would be an amazing opportunity to educate others on the exciting field of Molecular Diagnostics as well as combat the fear that comes with taking the Molecular Biology exam. I plan to focus on more specific areas in the field of Molecular Diagnostics that I came across in my studies, which will help others in their preparation for the MB(ASCP) exam. I will cover theory, applications, techniques, and practices. Also, keep an eye out for case study questions that I will provide to stretch your thinking through interpretation of molecular results, at the same time, keeping you up to date on hot topics in the field.
With all that said, the first most important suggestion I have is: spend time preparing to study. While it might seem silly to some, having a plan BEFORE you jump into study mode will actually set you up for success. All too often, just reading everything you can on every single topic will result in information overload and ultimately burn you out. You will quickly find yourself jumping all over the place frantically trying to memorize every detail you come across.
First, browse the content outline and choose some texts to review. Notice how I say, “Choose some?” Don’t feel like you have to read all of them. I went online and reviewed the texts, I asked colleagues for recommendations, then decided to purchase two books. You might find that you need more or less, just don’t go overboard.
Next organize a binder. I am extremely visual and hands on so I study best with things in front of me that aren’t electronic based. I divided my binder based on the content outline. You will come across papers, technical notes, and procedures that you will want to keep as study tools. Having a binder for all of these notes from multiple sources will keep you on track. It will also serve as a great reference guide for you as you move through your career.
Now is where you can get super retro. You may have noticed in my photos that I made flash cards! It is a little archaic and time consuming, but I knew I was going to be busy with my daughter’s traveling basketball team; therefore, I needed something small I could take with me to study while sitting on the bleachers. I am aware of software programs that allow you to make electronic based flash cards, so if that works better for you feel free to try that route.
My take home message is, obtain and prepare whatever tools you need to get yourself ready to study. Organization is key and setting aside time each day, even if only an hour to focus on one application or theory will definitely be to your benefit. Reach out to colleagues and gather as much information as you can. Once all of your tools are in place, it’s time to get to work! For anyone interested in obtaining their MB(ASCP) certification, I urge you to check out the content outline and list of texts on the ASCP Board of Certification site.

-LeAnne Noll, BS, MB(ASCP)CM is a molecular technologist at Children’s Hospital of Wisconsin and was recognized as one of ASCP’s Top Five from the 40 Under Forty Program in 2015.
Microbiology Case Study: 32 Year Old Male with HIV
Case:
A 32 year old male with a history of HIV presented with a non-productive cough, pleuritic chest pain, and subjective fevers and chills. The patient’s CD4 count was 23 cells/mL; he was not on highly active anti-retroviral therapy (HAART) or prophylaxis for opportunistic infections. A bronchoscopy was performed out of concern for opportunistic infection; a silver stain of bronchoalveolar lavage fluid from the right middle lobe revealed the following.

Laboratory identification:
Pneumocystis jiroveci (P. carinii) was identified based on morphologic examination of the silver stained fluid. The spherical, slightly dented or concave firm-walled cystic form (4-7 mm in diameter) was identified within the foamy alveolar fluid. Flexible-walled trophozoite forms may also be present in pulmonary fluid but are difficult to recognize. The organism may also be identified by a monoclonal antibody microscopic method of detection (highly sensitive but expensive and may have nonspecific staining) or nucleic acid amplification methods. The organism does not grow in routine culture.
Discussion:
Pneumocystis is an opportunistic pathogen with worldwide distribution that has closer homology to fungi than protozoa, which is why the name was changed from P. carinii to P. jiroveci. Its life cycle is not entirely understood, but there are cyst forms, sporozoite forms, and trophozoite forms.
Infection is acquired by inhalation. It is believed that most people are sub-clinically infected during childhood and that the infection is usually well contained by the immune system. During times of immunocompromise, the organism adheres to type I pneumocytes and replicates extracellularly while bathing in alveolar lining fluid causing the alveolar spaces to fill with foamy material. The organism is not susceptible to common antifungal agents and is treated with trimethoprim-sulfamethoxazole.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Ketones
Most people who work in a clinical laboratory know a little about ketones or ketone bodies. The two facts that most people know include: 1) when you perform a urinalysis (UA), it includes a semiquantitative ketone result, and 2) high ketones are seen in diabetic ketoacidosis. But what is a ketone, where do they come from, and what are we measuring when we measure ketones?
In the laboratory medicine world, “ketones” refers specifically to acetoacetate (Acac), acetone and beta-hydroxybutyrate (BOHB). When the human body cannot utilize glucose, either because it is not present (fasting, starvation) or because it is present but cannot be used (lack of insulin to get glucose into the cells), the body instead breaks down fatty acids for energy. Fatty acids are mostly made up of long chains of carbons with hydrogens attached, so one of the main products of fat breakdown is 2-carbon acetyl-CoA. When a person is using lots of fats, like when they cannot use glucose, the production of acetyl-CoA exceeds the body’s ability to metabolize it via the Kreb’s cycle and it ties up lots of coenzyme A (CoA) needed for other processes. Thus, the body combines two excess acetyl-CoA into an acetoacetate, freeing up the CoA. The more acetyl-CoA produced from fat breakdown, the more acetoacetate produced. From there, the acetoacetate is converted to BOHB enzymatically or degrades spontaneously to acetone. BOHB is a dead end. Once there, the BOHB simply continues to build up until the production of acetyl-CoA no longer exceeds its utilization capacity. At that point, the BOHB is converted back to acetoacetate and then to acetyl-CoA for the body to be able to utilize it.
The most common form of ketoacidosis is probably diabetic ketoacidosis, in which blood glucose levels are high, but the glucose cannot get into the cells and be used, so fats are broken down for energy. At the height of a ketoacidosis, roughly 70% of the ketones in the body will be in the form of BOHB. This has implications for what we measure and for the monitoring of the treatment of ketoacidotic crises. UA dipstick ketones measure acetoacetate, and some will also detect acetone. None of the available UA methods measure BOHB. Thus, ketones measured in a UA will rise as ketoacidosis occurs, drop at the height of ketoacidosis as they are converted to BOHB, and then rise again as the condition is resolving and BOHB is converted back to Acac. A high Acac will occur both at the beginning and toward the end of the ketoacidosis, and Acac may actually be low at the height of a ketoacidotic crisis. BOHB on the other hand rises as the crisis evolves and drops as the crisis is resolved. The best test for following the resolution of a ketoacidotic crisis is repeat BOHB measurements.
BOHB is generally measured enzymatically on blood samples. BOHB response is maximal about 3 hours after glucose peaks. For example in a diabetic ketoacidosis, the peak BOHB will occur about 3 hours after the glucose peaks and in a normal patient given a glucose load, the BOHB will be lowest about 3 hours after the glucose peaks. During resolution of ketosis BOHB decreasing by half about every four hours as long as no more ketones are being produced. The test for BOHB is most commonly performed quantitatively using a kit adapted to the open channel on a chemistry analyzer. A point of care analyzer is also now available for BOHB.
Measuring ketones is most commonly used to monitor ketoacidosis, but ketone measurement can also be helpful in the differential diagnosis of some inborn errors of metabolism. For example, in fasting states, ketones should be elevated. If they are not, it can be an indication of disorders in fatty acid metabolism, or ketone metabolism itself. Additionally, in hyperammonemia states, the absence of ketones and acidosis indicates a urea cycle defect. Their presence suggests an organic acid disorder. Thus measuring ketones has multiple uses in medicine.
-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.
Calling New Laboratory Directors and Managers
If you’re a laboratory director or manager who’s recently stepped into that role, the editors of Lab Medicine want to hear from you. As a new leader, you’re sure to have questions, challenges, and insecurities. Leave your questions in the comments, and it could be discussed in a future podcast.
