Clinical History
An 8 week old female was brought to an outside hospital due to pallor, decreased eating over several days, vomiting, fever, and blue color in the feet. The patient had received her two month vaccinations the day prior to presentation. Her past medical history was significant for being born at 32 weeks gestation, followed by an uneventful 4 week NICU stay. At the outside hospital the patient was in respiratory distress, tachycardic, with pallor. She was intubated and transferred to our institution due to concern for an ALTE (apparent life-threatening event). Blood and CSF specimens were drawn. Upon presentation, the patient had a white blood cell count of 19,600/mm3. Her CSF had 63 nucleated cells/mm3 (30% neutrophils, 49% lymphocytes, 11% monocytes), glucose of 23 mg/dL and protein of 212 mg/dL. Blood and CSF cultures were performed with the following results:
Laboratory Identification
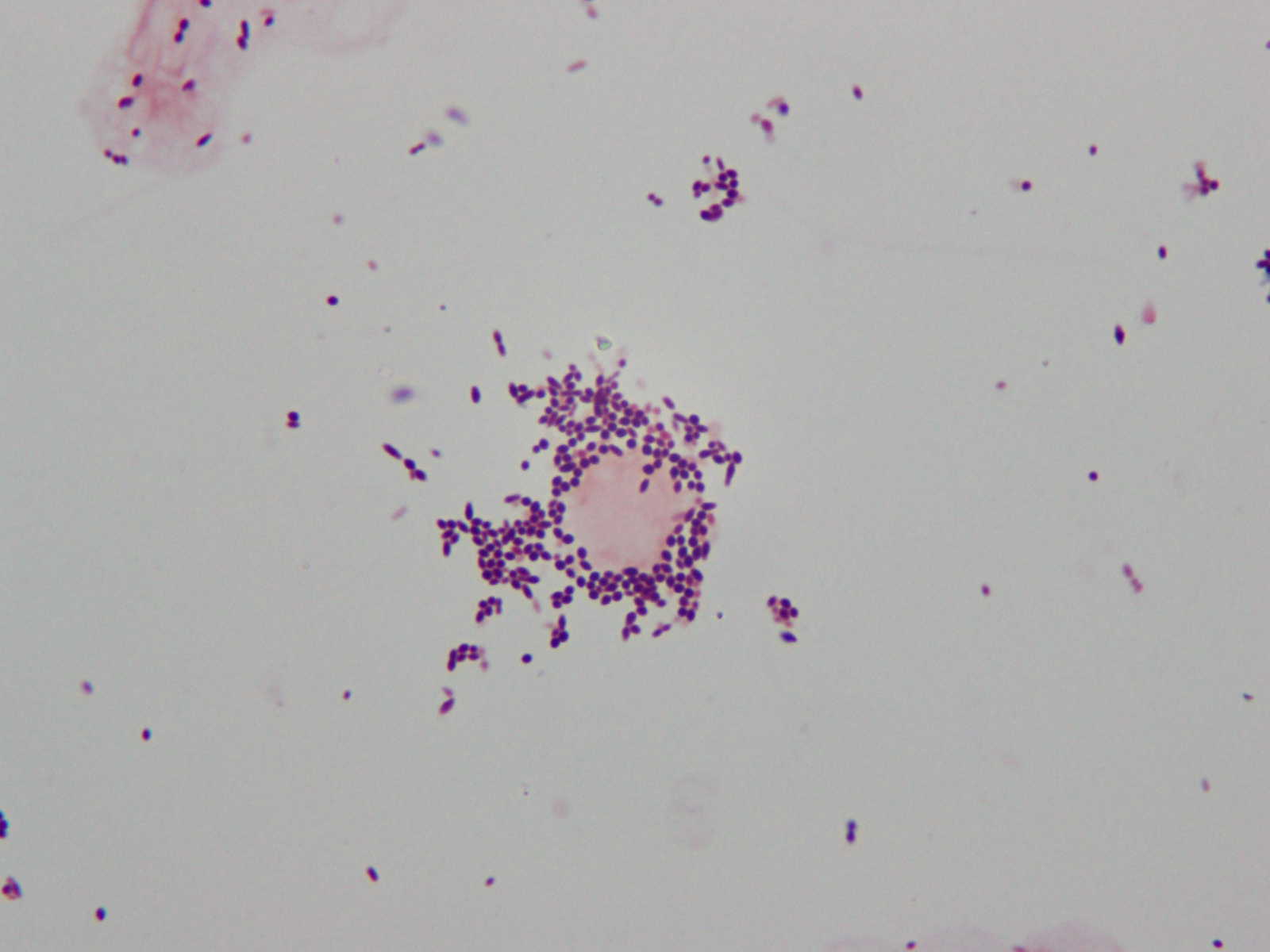
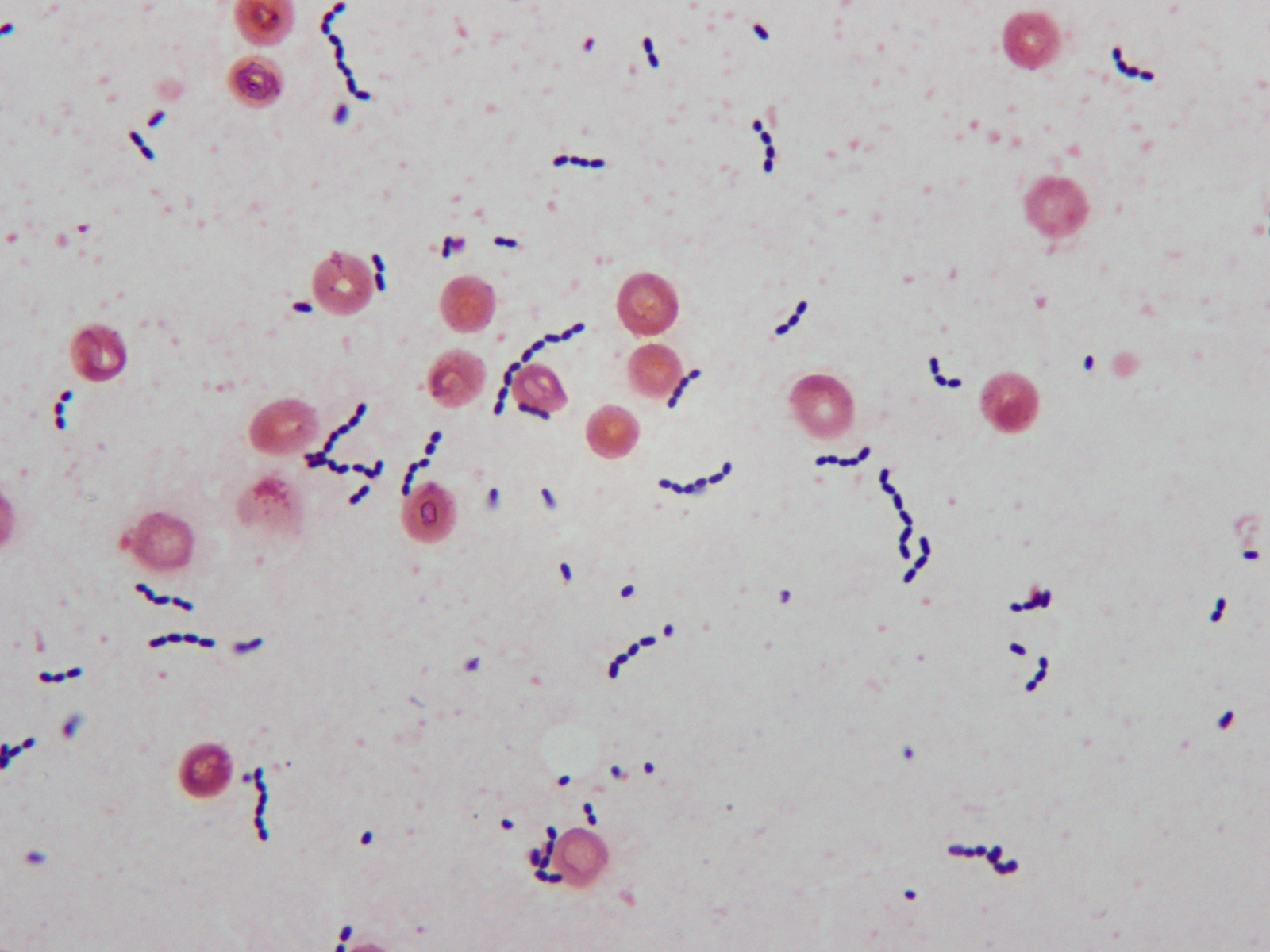
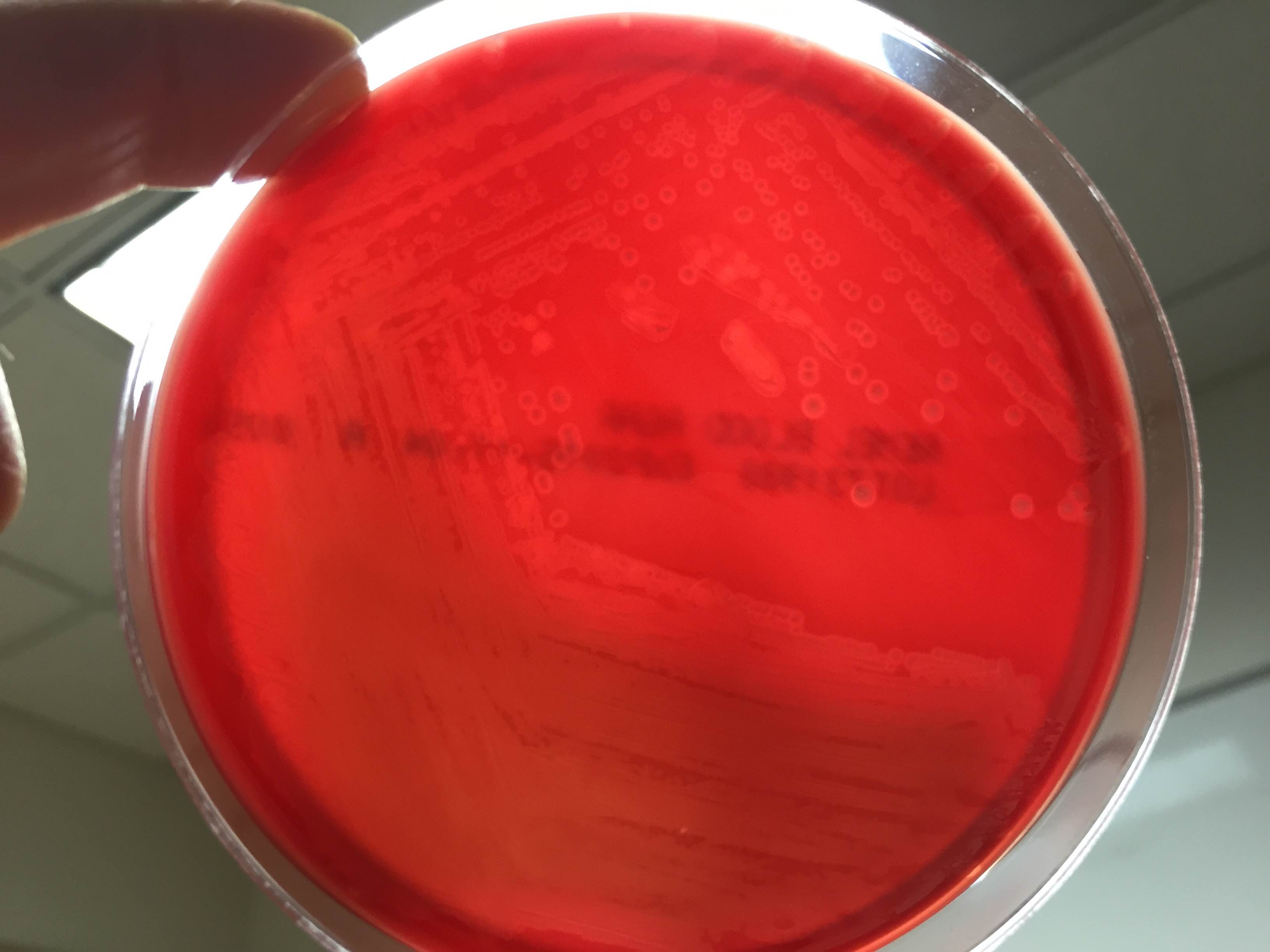
CSF Gram stain was read as many Gram-variable coccobacilli (Image 1) and blood culture Gram stain was resulted as Gram-positive cocci in pairs and chains (Image 2). The Nanosphere Verigene Gram-positive blood culture molecular assay was performed on the positive blood culture broth immediately following Gram staining. CSF and positive blood culture specimens were plated to 5% sheep blood, chocolate, MacConkey, and CNA agars. In >24 hours colonies from both specimens grew a single organism on sheep blood, chocolate, and CNA agars. On blood agar, colonies exhibited a soft zone of b-heomlysis (Image 3). Colony Gram stains showed Gram-positive cocci in chains, catalase testing was negative, and the organism typed in Lancefield antigen group B. Verigene identified the organism directly from the positive blood culture broth as Streptococcus agalactiae (aka Group B Streptococcus or GBS) and MALDI-TOF mass spectrometry confirmed the identification of S. agalactiae.
Discussion
Laboratory Considerations
As our CSF specimen demonstrated, streptococci can be difficult to interpret from specimen Gram stains. Organisms are often are pleomorphic in size and shape and they have a tendency to stain Gram-variable. This lead to the report of Gram-variable coccobacilli on our patient’s CSF culture.
S. agalactiae produces a soft zone of b-heomlysis on sheep blood agar. Unlike Streptococcus pyogenes (aka Group A Streptococcus) which produces a wide zone of b-hemolysis, soft b-hemolysis can often be very subtle, especially with young growth. Soft zones b-hemolysis can best be seen by holding plates up to a light source or my moving a colony out of the way to observe if hemolysis is present underneath. The pattern of S. agalactiae b-hemolysis is very similar to that produced by Listeria monocytogenes. Streptococcal isolates that type as Lancefield Group B, but produce large zones of b-hemolysis can create confusion and are most likely not S. agalactiae, but S. porcinus or S. pseudoporcinus.
Clinical Significance
S. agalactiae is the cause of significant neonatal disease. Early-onset infection presents as systemic infection, respiratory distress, apnea, shock, and pneumonia within the first 24 hours of life (range, 0–6 days). Meningitis is less common in early-onsetS. agalactiae infections, found in just 5-10% of cases. Late-onset disease presents at 3 to 4 weeks of age (range, 7–89 days) as meningitis and/or sepsis with other focal infection. Approximately 50% of survivors of early- or late-onset meningitis have long-term neurologic sequelae.
S. agalactiae colonizes the urogenital or gastrointestinal track of 10-30% of pregnant women. Being born to a S. agalactiae colonized mother is the most significant risk factor for development of disease in neonates. For this reason, women are screened for “Group B Strep” colonization between 35 and 37 weeks of pregnancy. Women found to be colonized receive prophylactic antibiotics immediately prior to delivery to prevent transmission to the child. Since implementation of these practices in 1996, there has been a substantial decline in early-onset S. agalactiae infections. Interestingly, these measures have not affected the incidence of late-onset disease.
Treatment
Until recently S. agalactiae was considered universally susceptible to penicillin. There have now been a few reports of S. agalactiae isolates with increased penicillin MICs due to mutations in the penicillin binding protein Pbp2x. The detection of these isolates is still extremely rare, so much so that S. agalactiae susceptibility testing for penicillin and other b-lactams is not considered necessary at this time. Penicillin and its derivatives are the preferred treatment option.
Patient follow-up
Our patient had a complicated course of late-onset Group B Streptococcal meningitis including multifocal cerebral infarctions and seizures. She was treated with a 28 day course of ampicillin. Blood cultures taken 24 hours after the start of antibiotics were negative and her CSF culture was negative when rechecked 5 days after her presentation. Due to her complicated course, the patient was hospitalized for 4 weeks. Follow-up appointments have shown the patient’s MRI is nearly normal 8 weeks post infection and the patient is doing well, although she is still followed by neurology to assess for long term sequelae.
Our patient’s mother had an unknown Group B Strep carrier status at the time of her birth, as she was born at 32 weeks, which is before routine screening occurs for pregnant women. Either way, the mother’s status would not have affected the patient’s risk for late-onset Group B Streptococcal infection.
References:
- Red Book 2015
- Journal of Clinical Microbiology, 10th edition

-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.

Very interesting post. Fifty three years ago I lost my firstborn to a pneumonia when two days old. I became aware of Streptococcus agalactiae of course, in my technology training, and have been convinced ever since of the toll this organism takes on our newborns.