Case history:
An 18 year old pregnant woman at 16 weeks gestation presented at the emergency department with nausea and vomiting for 3 days. Three days ago she and some of her friends ate chicken at a party. None of her friends experience her symptoms. Laboratory tests revealed urinary tract infection and a stool sample was sent to the microbiology laboratory for culture.
She was prescribed an antibiotic and was released from the ED.
Laboratory identification:
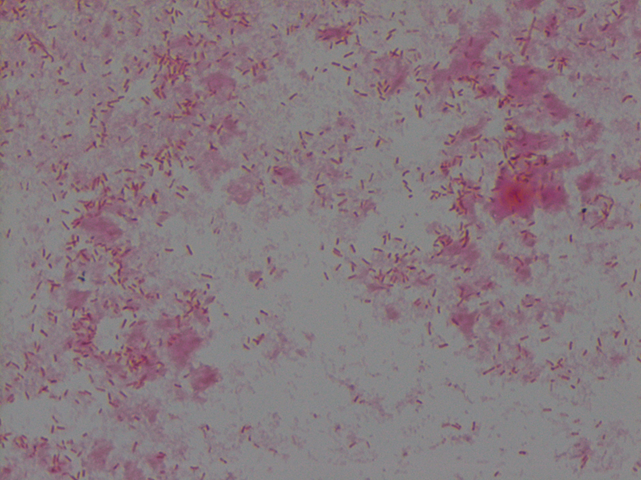
The organism grew well on MacConkey agar, and formed small colorless lactose-negative colonies. Gram stain revealed short gram-negative bacilli and MALDI-ToF confirmed the bacteria as Yersinia enterocolitica.
Discussion:
Yersinia enterocolitica is a gram negative, short, non-spore-forming bacillus in the family Enterobacteriaceae. They can exhibit bipolar staining, especially from the primary sample. It is a facultative anaerobe can grow at temperatures ranging from 4-43oC that is motile at room temperature but non-motile at 37oC. The organism grows well on MacConkey agar, and forms small colorless lactose-negative colonies but if the clinical team is suspicious for Yersinia, a selective growth medium is recommended. The most widely used is cefsulodin-irgasin-novobiocin (CIN) agar, which inhibits the growth of competing flora and produces characteristic colony morphology (red color with “bull’s eye” appearance).
The major route of Y. enterocolitica infection is through contaminated foods or water. The primary pathogenic event is colonization of the intestinal tract where most of the pathologic effects and clinical manifestations occur. Temperature and calcium concentration regulate expression of virulence factors that guide the invading Yersinia and allow them to survive and disseminate.
The most common form of disease caused by Y. enterocolitica is gastroenteritis associated with consumption of contaminated food or water, especially raw or undercooked pork such as chitterlings. Disease can range from self-limited gastroenteritis to terminal ileitis and mesenteric lymphadenitis that can be misdiagnosed as appendicitis. Gastrointestinal infections are usually self-limiting and do not merit antimicrobial therapy. However, in immunocompromised hosts and in patients with septicemia or invasive infection, the mortality can be high (approximately 50%).
Kossivi Dantey, M.D. is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.

–Christi Wojewoda, MD, is certified by the American Board of Pathology in AP/CP and Medical Microbiology. She is currently the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
