Contrary to popular belief, “irregardless” is not a word. The correct word is “regardless.” One can be frustrated or one can be flustered, but it is incorrect to say one is “flustrated.”When these common grammatical errors are made, it can be very irksome for some Type A Personality laboratory professionals. For those in the field of lab safety, however, this can be a lesson for learning how to improve the lab safety culture.
Very often grammatical errors are made because people simply do not remember what is correct, or the correct use of the word was never explained to them. If we hear something that is wrong, we may make a judgement about the person who said it—they are not well-educated, they are lazy, etc. We tell ourselves a story, and often, unfortunately, it is inaccurate.
You walk into the laboratory and you see the new tech Judy working at the bench with no gloves. Last week you spoke to Judy about the same issue, and she told you she would wear them from now on. In your frustration you believe Judy to be obdurate and someone who willfully violates lab safety practices. Because these things are in your mind, the conversation you are about to have with Judy will not go well.
Consider the following options:
Judy ran out of gloves and doesn’t know where to get more.
Judy went to get more gloves in the store room, but there is a combination lock on the door and she doesn’t know what it is.
Judy has developed a skin reaction to the gloves and is embarrassed to bring it up.
Judy just received a phone call that her mother is very ill and she is quite upset.
Judy saw the supervisor working without gloves and assumed you spoke to her last week because it’s your job to look out for safety.
These are just some of the possible influences on Judy’s decision not to wear gloves. To have good conversations about safety, your job is to determine the real issue without telling yourself stories first. Maybe everyone in the lab says “irregardless.” Maybe no one ever told Judy the correct word to use.
If you want to make a difference in your lab safety culture, think about the sources of influence on staff behavior. Ask about the reasons for the behavior, and work patiently to educate people about the consequences of unsafe actions. Use these tactics to reduce the amount of “flustration” you may feel when working to promote safety every day.
-Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
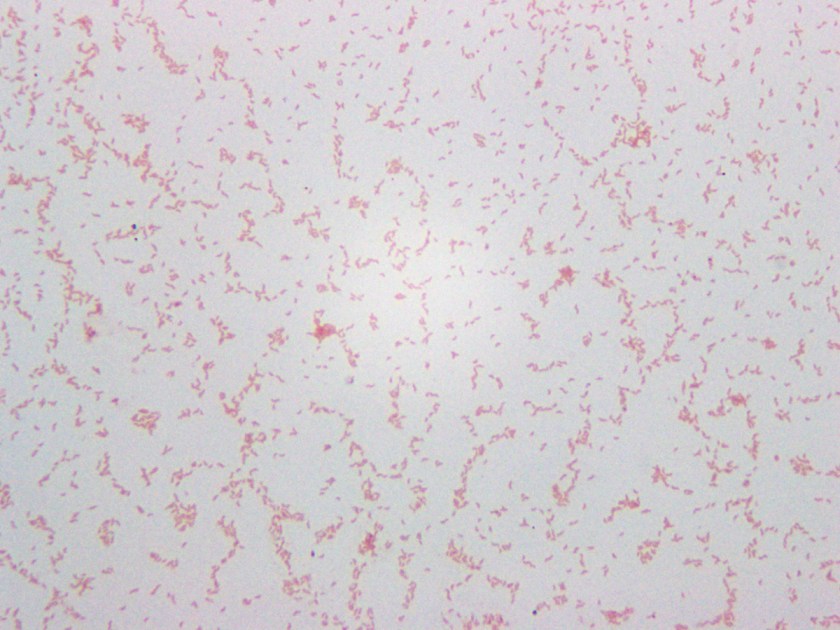
A 4-year-old girl with no past medical history had been feeling unwell for one day following a barbecue she had attended a few days prior. Her symptoms worsened to include colicky abdominal pain and bloody diarrhea, with as many as eight bowel movements per day. This persisted for the following two days; thereafter, she presented to the hospital also complaining of fever, nausea, and vomiting. She was found to be dehydrated and pale on exam, and was admitted for intravenous rehydration. Fecal leukocyte testing and stool cultures were sent. A Gram stain of the pathogen isolated from stool culture is shown in Figure 1.
An infectious etiology is highly suspected given this patient’s presentation, leading to work-up with fecal leukocytes and stool cultures. The presence of fecal leukocytes, which was positive in this patient, is a strong indicator of inflammatory diarrhea. Bacterial stool culture allows for detection of Salmonella, Shigella, Campylobacter, E. coli O157:H7, Yersinia, Aeromonas, and Plesiomonas.
Many different culture mediums are used to isolate bacterial gastrointestinal pathogens. In addition to the routine 5% sheep blood agar and MacConkey agar, a case of infectious diarrhea requires further workup to rule out the above mentioned pathogens. Sorbitol-MacConkey agar is a variant of traditional MacConkey agar, and is used to detect E. Coli O157:H7, which differs from other E. coli strains by its inability to ferment sorbitol, thus forming colorless colonies on this media. Xylose lysine deoxycholate (XLD) and hektoen enteric (HE) agars are utilized for the selection and differentiation between Salmonella and Shigella. A sweep of bacteria growing on the blood agar plate and subsequent oxidase testing is used for detection of Aeromonas and Plesiomonas, which are oxidase positive organisms unlike normal fecal flora which is oxidase negative. Cefsulodin-irgasan-novobiocin (CIN) agar is used for the selection and differentiation of Yersinia, which utilizes inhibitory substances (cefsulodin, irgasan, novobiocin, bile salts, and crystal violet) to prevent the growth of most bacteria. The agar also contains a pH indicator that turns red or pink when mannitol is fermented; with Yersinia having a characteristic ‘bull’s eye’ colonies with red centers and clear edges. CIN is incubated at room temperature for 48 hours. Finally, Campy CVA agar is a selective media for Campylobacter containing antimicrobial agents cefoperazone, vancomycin, and amphotericin B (CVA) which inhibit normal fecal flora. This media is incubated at 42°C under microaerophilic conditions, which support the growth of Campylobacter jejuni and C. coli.
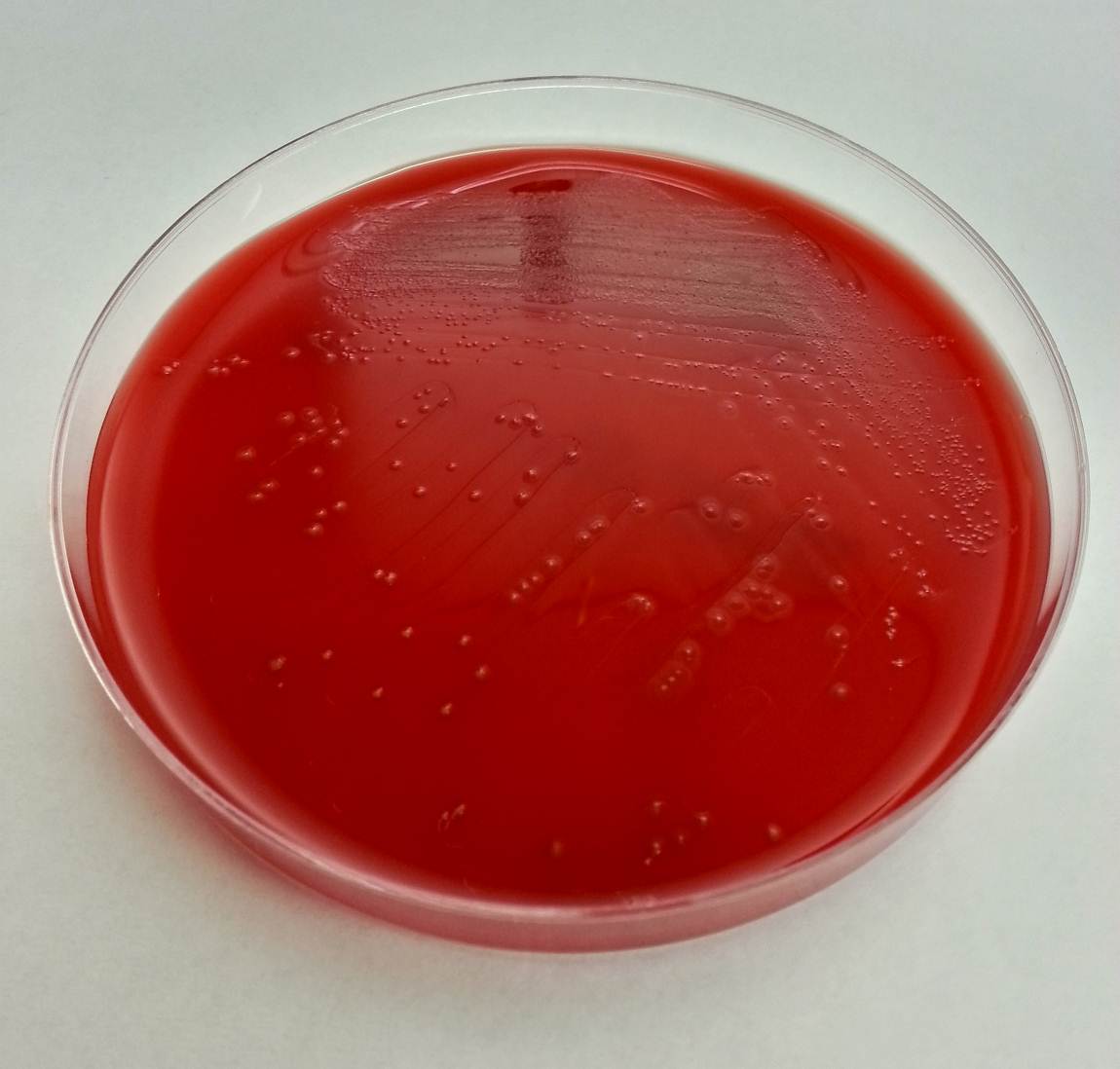
Our patient’s culture grew gray, non-hemolytic colonies on Campy CVA agar (Figure 2). The organism was identified as Campylobacter jejuni by MALDI-TOF MS (matrix-assisted laser desorption/ionization, time of flight mass spectrometry).
Figure 2. Bacterial colonies growing on Campy CVA agar
Campylobacter are gram-negative, microaerophilic, curved or spiral rods in the family Campylobacteriaceae. They are widely distributed in animals and infection is most often transmitted by contaminated foods, particularly undercooked chicken. The species most commonly associated with human infections are C. jejuni and C. coli, with C. jejuni accounting for the large majority. Infection with C. jejuni has been linked with subsequent development of Guillain-Barre syndrome two to three weeks following the initial illness. Our patient improved following two days of IV fluids and antibiotics with no subsequent follow up after discharge.
References:
Manual of Clinical Microbiology, 11th edition
-Said Albahra, MD, 1st year Anatomic and Clinical Pathology resident at the University of Texas Southwestern Medical Center.
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
In a post back in September, I quickly summarized the abnormalities that can occur with chromosomes as a whole (such as deletions, insertions, transversions, etc). There is so much more to learn (more than I could possibly put into one blog post), because the way chromosomes behave, depends on their structure and DNA sequence. For instance, genes with the same DNA sequence will behave differently depending on where they are located on a chromosome as well as the effect of the surrounding DNA sequence.
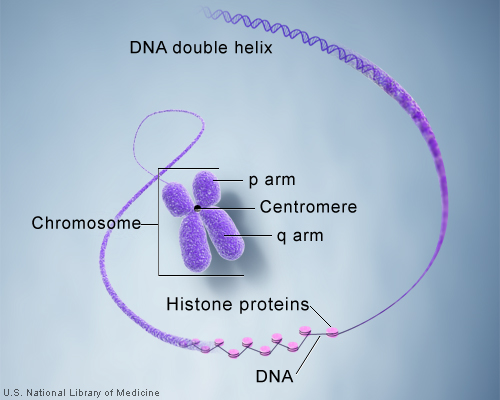
So how exactly is the immense length of DNA compacted into a chromosome? Let’s take a DNA sequence and see just how it makes up a chromosome. A single molecule of DNA spools around histone protein cores forming bead like structures called nucleosomes. Between each nucleosome is a sequence of DNA termed “linker DNA.” The amino acids associated with histones are lysine and arginine. The super coiled form is compacted and can be visualized as a karyotype in laboratory testing.
The centromere is the connection point of the duplicated chromosome, while telomeres are the endpoints. The short arm of the chromosome is termed “p” and the long arm of the chromosome is termed “q.” If we take these two chromosome arms into consideration, there are three types of chromosome morphology:
Metacentric – Chromosome arms are equal in length
Sub-centric – One arm is longer than the other
Acro-centric / Telocentric – One arm is extremely small or even missing
Chromosomal Staining Methods
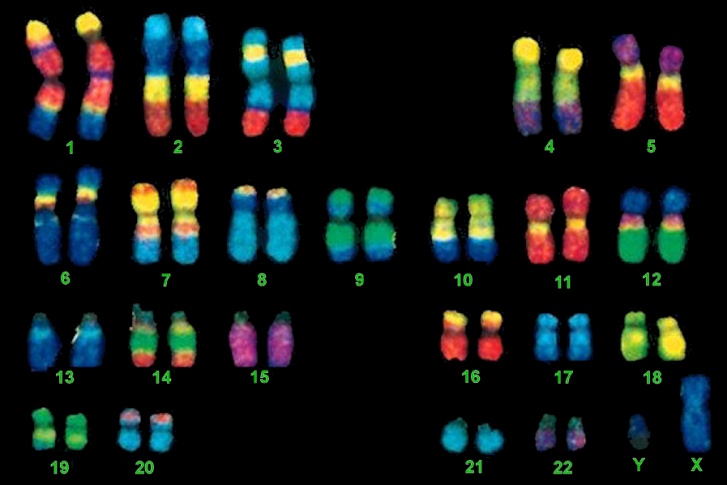
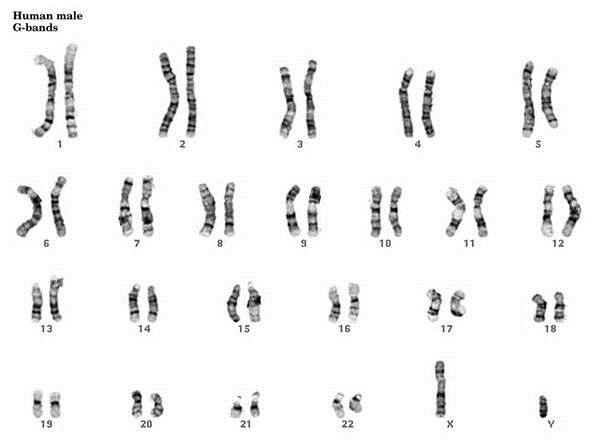
As I mentioned above the complete set of chromosomes for an individual can be visualized via a karyotype. I’ve listed a few of the ways this can be accomplished:
G-Banding – Chromosomes are stained with giesma stains. The appearance differs based on the treatment of chromosomes prior to staining.
Q-Banding – Chromosomes are stained with fluorescent dyes, quinacrine or quinacrine mustard. Q-Band staining is similar to G-banding in that the fluorescent regions represent the AT-rich regions of the chromosome.
R-Banding – Results from heat treatment in a phosphate buffer followed by staining with Giesma dyes.
C-Banding – Centromere staining that results from alkali treatment.
TYPE OF BANDING
STAINING SUMMARY
G-Banding
· Geisma stain
· AT-rich regions stain darker than GC-rich regions
Q-Banding
· Quinacrine fluorescent dye stains AT-rich regions
R-Banding
· Banding pattern is opposite G-banding
C-Banding
· Stains heterochromatic regions close to the centromeres
· Usually stains the entire long arm of the Y chromosome
So how do you exactly identify chromosomal location based on banding patterns?
In studying disease and mutation, we follow a specific type of nomenclature to designate the regions that are of interest to us. Let’s take for instance something like the 22q11.2 deletion. What do all of these numbers and letters mean? To quickly summarize, 22q11.2 deletion syndrome occurs from the deletion of a small piece of chromosome 22 at a location: q11.2
22q11.2 DELETION
22
· Chromosome 22
q
· Long arm of chromosome (q)
1
· Region 1
1
· Band 1
2
· Sub band 2
So now, when we add in karyotope information you might see something like the following:
46, XY, del(8)(q21)
When you break it down, it states the patient is male (XY) and has a deletion in the long arm (q) of chromosome 8 at region 2, band 1
Translocation nomenclature can get a little more confusing:
46, XX, t(3;12)(p12.1;p11)
This designates a female has a translocation between the short arms (p) of chromosomes 3 and 12 and region 1, band 2, sub band 1; and region 1 band 1 respectively.
An example of Down syndrome: 47, XX + 21 (Female has an extra chromosome 21)
An example of Klinefelter Syndrome: 47, XXY (Male with extra X chromosome)
What do “FISH” have to do with Molecular Biology?
FISH, an acronym for Fluorescent In-Situ Hybridization, is a method used to detect and visualize protein, RNA, and DNA structures in the cell. FISH analysis is a relatively fast method that provides great resolution as it incorporates fluorescent probes labeled for detection of specific regions, deletions, and translocations. The images below show the difference between FISH and Karyotype images.
Robertsonian translocations are of importance because they involve translocating most of one entire chromosome to the centromere of another chromosome. They can be balanced or unbalanced. A balanced translocation usually results in no health difficulties because there isn’t a gain or loss of genetic material. However, due to the duplication or deletion of genetic material in an unbalanced translocation, syndromes and other malformations are likely to occur. The chromosome pairs common for Robertsonian translocations include translocations between 13 and 14, 14 and 21, and 14 and 15.
During a Robertsonian Translocation two chromosomes (typically acrocentric in formation) will break apart at their centromeres. The long arms will fuse to form a single chromosome and the short arms will also join to form a product. Typically the product created by the short arms contains nonessential genes and is eventually lost through cell division. Most people with ROB have only 45 chromosomes in each cell containing all of the essential genetic material and appear normal.
An example of a balanced Robertsonian Translocation would be when the long arms of chromosomes 14 and 21 fuse together. Phenotypically, the heterozygous carrier would appear normal because there are two copies of the major chromosome arms, resulting in two copies of the essential genes. However, children of the carrier could inherit an unbalanced translocation that causes Trisomy 21 (Down Syndrome).
Test your Knowledge!
Which two amino acids are associated with histones?
What type of chromosome morphology is shown:
If you wanted to stain chromosomes to see varying regions that were AT-rich, which type of stain would you use?
Describe the following karyotype results: 46, XX, t(1;14)(p21.3; p17.6)
Answers
Lysine and Arginine
Sub-centric
G-Banding (although Q-Banding also will produce darker regions that are AT-rich)
Female patient, with a translocation between the p and q arms of chromosomes 1 and 14, and region 2, band 1, sub band 3; and region 1 band 7, sub band 6 respectively.
References:
Buckingham, L. (2012). Molecular Diagnostics: Fundamentals, Methods and Clinical Applications (2nd ed.). Philadelphia: F.A. Davis Company.
Coleman, W.B, Tsonagalis, G.J. (2005). Molecular Diagnostics: For the Clinical Laboratorian. New York: Springer-Verlang
Searle, B. Rarechromo.org. The Rare Chromosome Disorder Support Group. 1996. Web. 19 Dec. 2015.
-LeAnne Noll, BS, MB(ASCP)CM is a molecular technologist at Children’s Hospital of Wisconsin and was recognized as one of ASCP’s Top Five from the 40 Under Forty Program in 2015.
Two weeks after returning from a camping vacation in Cape Cod, a 58 year old man presented to the emergency room with six days of fatigue, fever, chills, arthralgia, myalgia, mild right upper quadrant pain, and a frontal headache. Clinical workup revealed worsening leukopenia, thrombocytopenia, and elevated transaminases when compared to preliminary testing done by the patient’s primary care provider at the onset of his symptoms. His preliminary workup was also negative for Lyme antibody, EBV and CMV IgM, and viral hepatitis markers. At no point did the patient notice a skin rash or a tick anywhere on his person.
Differential Diagnosis:
Lyme Disease
Anaplasmosis
Ehrlichiosis
Babesiosis
Rocky Mountain Spotted Fever
Viral Meningitis
Bacterial Meningitis
Leptospirosis
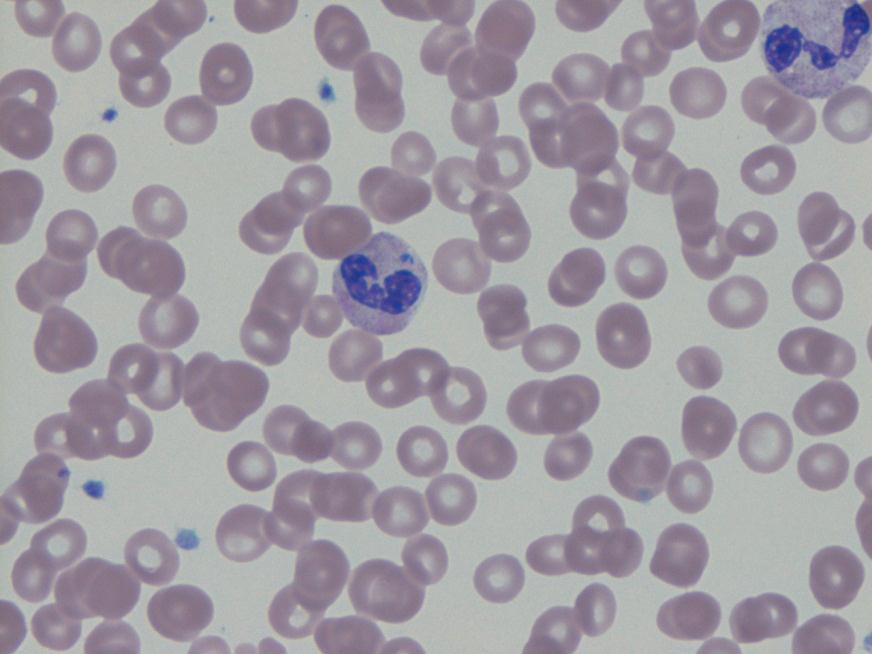
Blood smear showing granulocyte with intracytoplasmic morulae.Blood smear showing granulocyte with intracytoplasmic morulae.
Laboratory Identification:
Anaplasma phagocytophilium was initially identified by PCR. Retrospectively, the blood smears originally examined for Babesia by both hematology and parasitology were reviewed. Both slides showed multiple granulocytes with intracytoplasmic morulae.
Discussion
Anaplasma phagocytophilium is the bacterium responsible for the tick-borne disease known as human granulocytic anaplasmosis. Anaplasma is transmitted to humans primarily through the bite of an infected Ixodes scapularis, the same species of tick which transmits Borrelia burgdorferi (Lyme disease) and Babesia spp. (human babesiosis). Anaplasmosis, Lyme disease, and babesiosis therefore share roughly the same geographical distribution in the United States with northeastern and upper midwestern states reporting the most cases.
Anaplasmosis most commonly presents about 1-2 weeks after a tick bite with the sudden onset of a variety of non-specific symptoms including fever, chills, headache, malaise, myalgia, nausea, and abdominal pain. Anaplasmosis, unlike other tick-borne diseases, rarely causes a rash. Routine blood tests may show thrombocytopenia, leukopenia, or elevated liver enzymes in some patients. Severe clinical presentations, more common in immunosuppressed patients, may include difficulty breathing, hemorrhage, renal failure or neurological problems. Anaplasmosis is estimated to be fatal in less than 1% of cases.
A routine blood smear is the quickest method for establishing an early presumptive diagnosis. Microscopic examination of the smear may reveal microcolonies of Anaplasma known as morulae within the cytoplasm of infected granulocytes. Ehrlichia, in contrast, will preferentially target and form morulae within monocytes. Because not all patients with anaplasmosis have visible morulae, this test is diagnostically insensitive and should be followed by further testing.
Confirmatory serologic testing for anaplasmosis includes an indirect immunofluorescence assay using an Anaplasma phagocytophilum antigen. For the highest sensitivity, this test should be performed on paired serum samples collected at least 2 weeks apart with the first sample taken as early in the disease as possible. A positive test will demonstrate a four-fold rise in antibody titers. Although it is a very sensitive detection method when run with paired samples, the lengthy testing time is less than ideal for patients requiring hospitalization for their disease.
A PCR assay on a sample of whole blood, although only available at a few reference laboratories, is the most efficient and accurate way to detect Anaplasma during the acute phase of the illness. The sample used for PCR testing should be taken before the initiation of antibiotic therapy as it causes the sensitivity of this test to rapidly decline.
Doxycycline is the first line treatment for adults and children of all ages with anaplasmosis as recommended by both the CDC and the AAP Committee on Infectious Diseases. Patients should be treated for at least 3 days after the fever subsides. Standard duration of treatment is 7 to 14 days. Therapy should be initiated immediately when there is a high clinical suspicion of anaplasmosis. A physician should never wait for the results of confirmatory testing to begin treatment. Most patients see improvement within 24-48 hours of treatment and non-response to doxycycline may indicate a different disease process.
Anaplasmosis, like many other tick-borne diseases, is a nationally reportable disease. All cases should be reported to local and state health departments as well as the CDC.
-Elaine Amoresano, MD, is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
I decided to take this year-end opportunity to say good bye for a while. It’s with some regret that I hang up my blogging hat for now. My next year is going to extraordinarily busy, as I take on the role of President of AACC. As much as I have enjoyed writing posts to this blog for the last 2 ½ years, I’m afraid blogging routinely will have to take a back seat for 2016. I do hope to get an occasional post in, but we’ll see.
It has been my distinct pleasure to write posts for Lablogatory. I encourage any of you who have any inclination at all to write about lab related issues, to take up blogging for this feature. Putting your thoughts on paper is one of the best ways I know to clarify those thoughts. Writing about something is somewhat akin to teaching it; doing so helps you to understand and learn it yourself. It has also let me see just how clearly I can express the concepts I’m trying to get across.
Another thing that blogging has clearly taught me is to be sure of my facts. Seeing something in writing always gives it so much more weight than simply hearing it. I have always been surprised by the number of things that I “know” to be fact from my laboratory years of experience, that I cannot find backing or literature support for. Thus when I’m blogging about a topic, I often find myself suddenly questioning, exploring and confirming things that I’ve always assumed were “fact”. And if I can’t find supporting references, I clearly express that it is an opinion and where that opinion arises from.
And lastly, writing posts for this blog has allowed me to interact with a wide variety of people I would not have met otherwise, starting with Kelly Swails, who often tweaked my posts into something better, and continuing on with people who have responded, both online, and in person. Even one of my hospital administrators in Risk Management stopped me one day in the hall to say, “Oh! I read your blog about dilutions!”
Posting articles for this blog has given me the opportunity to think about a variety of topics, to clarify my thoughts by putting them into writing, and to interact with some great people. I hope to be able to pick this back up after my term of office. In the meantime, many thanks to everyone who has read my posts. See y’all on the other side!
-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.
Case History:
A 29 year old woman presents to the hospital with contractions at 30 weeks gestation. This is her first pregnancy and it was previously uncomplicated. She did not experience loss of fluid or vaginal bleeding and did not have a history of recent illness or fever. A swab for group B Streptococcus (GBS) was collected and the patient was started on prophylactic penicillin. Clinical evaluation revealed evidence of acute infection with an elevated C-reactive protein and an increased white blood cell count with 97% neutrophils. Amniocentesis was performed and the amniotic fluid was sent to the laboratory for Gram Stain and culture.
Labor was allowed to progress and the infant was delivered vaginally. Cultures of cerebrospinal fluid and blood from the neonate were negative. The placenta was sent for histologic evaluation.
Gram stain shows Gram negative bacilli.Tiny gray colonies on blood agar with a bleach-like odor.Small, pale yellow colonies on chocolate agar.
Laboratory Identification:
The laboratory workup revealed a gram negative bacillus with rounded ends that grew small grey to pale yellow colonies on blood and chocolate agars. The colonies had three regions; a raised central region, a refractile flat region, and an outer rougher spreading region. The colonies had a distinct bleach-like smell. There was no growth on MacConkey agar. The organisms were oxidase positive, catalase and indole negative. Mass spectrometry was utilized to identify the organism as Eikenella corrodens.
Discussion: Eikenella corrodens is a component of normal mouth and upper respiratory tract flora. It is most notable for causing head and neck infections, periodontal disease, and as a significant player in “fight bite” infections. “Fight bite” results when a clenched fist hits another person’s mouth and the teeth cause lacerations to the hitter’s hand, which can subsequently lead to infection. Eikenella is implicated approximately 25% of the time in these types of infections. Only on very rare occasion is Eikenella known to cause gynecologic infections. Endometritis or cervicitis may infrequently be caused by colonization of an intrauterine contraceptive device (IUD) by Eikenella. And rarely, Eikenella is implicated as the isolated bacteria in cases of acute chorioamnionitis.
In the medical literature there are currently only 8 reported cases of chorioamnionitis caused by a pure Eikenella infection. As in our case, each of the women in the case reports had clinically silent infections and only presented with preterm labor. Most of the women were found to have elevated white blood cell counts in the absence of fever or alterations in other vital signs. In each case, the fetal membranes were intact. Two of the cases resulted in fatal infection of the neonates. Of note, three of the women were mentioned to be the recipients of oral intercourse throughout their pregnancies.
One of the reported cases involved a woman whose partner had a tongue piercing and it was noted that they engaged in daily oral sex during the pregnancy. The authors speculated that the tongue piercing played a role in the development of chorioamnionitis by either ascending vaginal infection or hematogenous spread caused by trauma from the tongue ring.
It is not known if a similar history was present in this case. The patient was treated with ampicillin and gentamycin and discharged following delivery. She is currently doing well. The infant has had no signs of infection, but at the time of this writing he is being treated in the neonatal intensive care unit for sequelae of prematurity.
References:
Garnier F, Masson G, Bedu A, et al. Maternofetal infections due to Eikenella corrodens. J Med Microbiol 2009; 58, 273-275.
Jadhav A, Belfort M, Dildy G. Eikenella corrodens chorioamnionitis: modes of infection? Am J Obstet Gynecol 2009; 200, e4-5.
-Britni Bryant, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
As a clinical laboratory scientist or a pathologist, perhaps you have questioned from time to time your value in the backdrop of our current state of healthcare. During my career, I admit to having felt that pathologists and laboratory staff are under-recognized for their contributions to provision of care on a day-to-day basis. Effective, efficient and most importantly, quality laboratory testing is clearly one of the key components for safe patient-centered care.
Laboratory testing is the single highest volume medical activity and lab tests directly affect a majority of medical decisions. Laboratory activity generates significant and potentially expensive downstream costs including prescriptions, imaging studies, and procedures. Although the laboratory most often provides indirect patient care, it is both necessary and critical. In particular, laboratory testing is becoming more intricate and “personalized” and thus brings us the golden opportunity to intervene on behalf of the patient.
A classic and current example is the recent development of novel “target-specific” oral anticoagulants. These drugs certainly provide benefit to patients on several levels, but also are still associated, unfortunately with risks of bleeding (as with all anticoagulants). These drugs came to the market without specific coagulation tests or antidotes, both of which are necessary in the event of bleeding.
Some tests are on the horizon (e.g. dilute thrombin time) and some are available with proper validation/calibration (e.g. anti-factor Xa activity). Late 2013 and early 2014 saw the approval of Kcentra prothrombin complex concentrate for emergent warfarin reversal in patients with active hemorrhage and just a few weeks ago, idarucizimab (Praxbind) was FDA-approved for reversal of dabigatran-associated bleeding. Andexanet, a Factor Xa inhibitor reversal agent is in Phase III trials and we should anticipate its arrival on the market soon. These are, of course, welcome additions to our armament.
Although these drugs and their reversal agents may be housed and released from our pharmacies upon order, the onus is on us as laboratory professionals to stay abreast of these new entities, therapeutics etc. so we can aid in their appropriate use. Our hematology, coagulation and transfusion services, along with pathologists, should be “at-the-ready” to answer questions and guide our clinical colleagues. Protocols for reversal strategies are key and we must take on a prominent role on the committees that develop these.
Never forget the important role YOU play in everyday diagnosis, prognosis and treatment decisions! Each day represents an opportunity for us to step up to the plate and be major players in this ever-changing and challenging healthcare environment. Let’s continue to make our presence and our value known!
-Dr. Burns was a private practice pathologist, and Medical Director for the Jewish Hospital Healthcare System in Louisville, KY. for 20 years. She has practiced both surgical and clinical pathology and has been an Assistant Clinical Professor at the University of Louisville. She is currently available for consulting in Patient Blood Management and Transfusion Medicine. You can reach her at cburnspbm@gmail.com.
“The Clinical and Laboratory Standards Institute (CLSI) has published a new document titled Management of Critical- and Significant-Risk Results (GP47-Ed1). This guideline provides current best practice recommendations for developing and implementing a policy and procedures for the identification, reporting, and management of critical- and significant-risk laboratory results. Emphasis is placed on management responsibilities such as development of the policy, the process, procedures, job descriptions, and monitoring systems that ensure effective reporting and compliance with regulatory requirements.
This new document refers to results as critical risk and significant risk, depending on the degree of risk to the patient. The recommendations in the standard are intended to be consistent with best practices for patient safety, and compliant with current, pertinent regulatory and accreditation requirements. GP47 includes an executive summary and appendixes with sample policies, reporting methods, escalation procedures, and monitoring tools.
This document is intended for clinical and laboratory directors, managers, and personnel who develop and implement laboratory policies and processes. The standard is also intended for health care administrators who oversee compliance with regulatory requirements, accreditation, and clinical practice standards related to patient safety. The recommendations cover every laboratory discipline and pertain to clinical laboratories of every size, scope, and complexity.”
Mumbai is one of the financial capitals in India, and millions of commuters ride its railway network to and from work every day. However, over the past several years, the available public transportation has not increased in proportion to the city’s rise in population. This has resulted in overcrowded trains and a staggering death toll from accidents and falls. In 2005, a total of 494 passengers lost their lives after falling from running trains. This figure went up subsequently in the coming years and climbed to 901 by 2013. In 2015 nine people a day, on average, lose their lives while on the move.
Knowing these facts, how inclined would you or your lab staff be to take a train ride in Mumbai? Not very. Yet, there are people in that city who willingly get on board every day. These conditions of danger are normal for them. This is their culture. They have become immersed in it, and it has become difficult for them to step back and look at the big picture–even for their own safety. They have to get to work.
In the past, laboratory professionals worked in departments where mouth-pipetting was normal, where eating, drinking and smoking was common, and where working without PPE was accepted. Today we look at old lab pictures of these behaviors and react (I hope) with surprise. But what applies to the commuters in Mumbai might also apply to labs of the past as well—those technologists were immersed in their culture.
Since those times, many lab safety regulations have been put in place, but that hasn’t fixed the safety culture everywhere. There may be, of course, other reasons for unsafe conduct in the laboratory. There may be behaviors that have been held onto after years of practice, there may be a lack of safety education, or safety may simply not be a priority for lab leadership. All of these factors are a part of the lab safety culture. Do you know the culture on your lab?
Assessing the culture in your laboratory is important. If you are in leadership, you should not assume that your singular view of the culture is accurate. There are several ways to evaluate the culture; make a visual assessment, review injury and exposure incidents, or have staff take a written culture assessment.
Provide adequate safety education for your staff. Are they aware that there might be a better, safer way? Do they know where the PPE and engineering controls are? Have they been trained in their use? Is there any safety leadership holding staff accountable so that there are not too many people on the train?
Laboratory professionals have to get to work, but unlike the workers of Mumbai, it’s not necessarily the trip to work that’s an issue; it’s the work places which are not inherently safe. It takes knowledge, education, training and focus to keep people safe in the laboratory. Put safety in its proper perspective: we are not dealing with falling from a train, but we do encounter injuries, exposures, and lab-acquired infections, some of which can be just as deadly as a fall. Know your safety culture, and learn what it will take to make the needed changes so that no one in your lab becomes a statistic.
-Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
I’m thoroughly convinced that in order to change laboratory information systems (LIS) and get the new LIS to work correctly you need a mixture of one part laboratory professional, one part information technology (IT) specialist, and one part interpreter. Add together and then vortex vigorously.
The laboratory professional is a given. It is absolutely necessary to have a person or people who understand the lab tests inside and out, from linear range to reference intervals to instrument capabilities to antibiotic susceptibilities to type and cross-match. There must be people with an understanding of how the tests work and what type of information is needed in order to ensure that when a test result appears in the electronic medical record for the doctor to see, it is an accurate result that makes sense and is interpretable.
The IT specialist is also a given. This person or people must completely understand not only how to program the system, but what type of programming is possible – what the computer system is capable of doing – or not doing. Being currently immersed in changing LIS systems at my institution, I have come to appreciate more and more how these two individual types must be able to communicate with each other and work together to design and implement an LIS that is functional for everyone.
Which brings us to the “interpreter”. Sometimes IT and lab people simply don’t speak the same language. I know I sometimes feel as though the IT people have begun speaking in tongues. I’m occasionally amused by the totally blank looks on the faces around me, and no doubt on my own. Thus what a project like this requires is a facile communicator with enough knowledge of both the lab and the programming to successfully interpret between the experts. I’m calling this person an “interpreter”, but calling him/her a communicator would be just as accurate.
In my institution the interpreter role is most frequently filled by laboratory technologists who have gone over to the Dark Side, otherwise known as Information Technology. Much as I hate to lose them as medical laboratory scientists, they are pretty nearly worth their weight in gold as interpreters when changing LIS systems. To continue the analogy, without their input in the mix, the vigorous vortexing necessary often results in an emulsion, not a smooth mixture. The finished product may not function as desired simply because the programmer did not understand what was needed, or the laboratory professional did not understand the inherent capabilities of the LIS.
With any luck, we have enough interpreters in our mix to end up with a functional LIS we can all live with. I know the current meetings are going as smoothly as they are due to these people’s work.
-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.













{kind=link}
{kind=link}