Case History:
A 29 year old woman presents to the hospital with contractions at 30 weeks gestation. This is her first pregnancy and it was previously uncomplicated. She did not experience loss of fluid or vaginal bleeding and did not have a history of recent illness or fever. A swab for group B Streptococcus (GBS) was collected and the patient was started on prophylactic penicillin. Clinical evaluation revealed evidence of acute infection with an elevated C-reactive protein and an increased white blood cell count with 97% neutrophils. Amniocentesis was performed and the amniotic fluid was sent to the laboratory for Gram Stain and culture.
Labor was allowed to progress and the infant was delivered vaginally. Cultures of cerebrospinal fluid and blood from the neonate were negative. The placenta was sent for histologic evaluation.


Laboratory Identification:
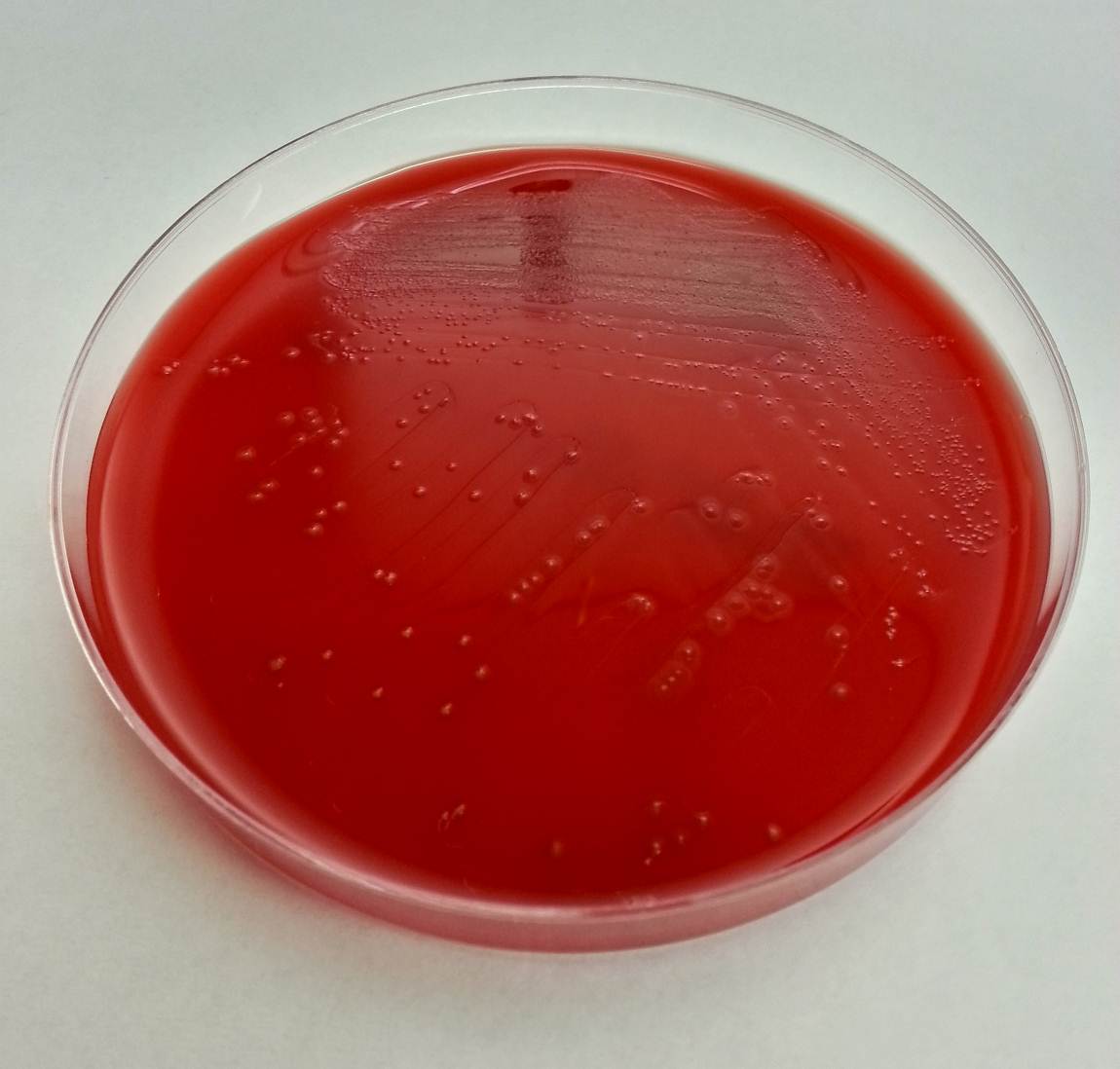
The laboratory workup revealed a gram negative bacillus with rounded ends that grew small grey to pale yellow colonies on blood and chocolate agars. The colonies had three regions; a raised central region, a refractile flat region, and an outer rougher spreading region. The colonies had a distinct bleach-like smell. There was no growth on MacConkey agar. The organisms were oxidase positive, catalase and indole negative. Mass spectrometry was utilized to identify the organism as Eikenella corrodens.
Discussion:
Eikenella corrodens is a component of normal mouth and upper respiratory tract flora. It is most notable for causing head and neck infections, periodontal disease, and as a significant player in “fight bite” infections. “Fight bite” results when a clenched fist hits another person’s mouth and the teeth cause lacerations to the hitter’s hand, which can subsequently lead to infection. Eikenella is implicated approximately 25% of the time in these types of infections. Only on very rare occasion is Eikenella known to cause gynecologic infections. Endometritis or cervicitis may infrequently be caused by colonization of an intrauterine contraceptive device (IUD) by Eikenella. And rarely, Eikenella is implicated as the isolated bacteria in cases of acute chorioamnionitis.
In the medical literature there are currently only 8 reported cases of chorioamnionitis caused by a pure Eikenella infection. As in our case, each of the women in the case reports had clinically silent infections and only presented with preterm labor. Most of the women were found to have elevated white blood cell counts in the absence of fever or alterations in other vital signs. In each case, the fetal membranes were intact. Two of the cases resulted in fatal infection of the neonates. Of note, three of the women were mentioned to be the recipients of oral intercourse throughout their pregnancies.
One of the reported cases involved a woman whose partner had a tongue piercing and it was noted that they engaged in daily oral sex during the pregnancy. The authors speculated that the tongue piercing played a role in the development of chorioamnionitis by either ascending vaginal infection or hematogenous spread caused by trauma from the tongue ring.
It is not known if a similar history was present in this case. The patient was treated with ampicillin and gentamycin and discharged following delivery. She is currently doing well. The infant has had no signs of infection, but at the time of this writing he is being treated in the neonatal intensive care unit for sequelae of prematurity.
References:
Garnier F, Masson G, Bedu A, et al. Maternofetal infections due to Eikenella corrodens. J Med Microbiol 2009; 58, 273-275.
Jadhav A, Belfort M, Dildy G. Eikenella corrodens chorioamnionitis: modes of infection? Am J Obstet Gynecol 2009; 200, e4-5.
-Britni Bryant, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
