Case History:
Two weeks after returning from a camping vacation in Cape Cod, a 58 year old man presented to the emergency room with six days of fatigue, fever, chills, arthralgia, myalgia, mild right upper quadrant pain, and a frontal headache. Clinical workup revealed worsening leukopenia, thrombocytopenia, and elevated transaminases when compared to preliminary testing done by the patient’s primary care provider at the onset of his symptoms. His preliminary workup was also negative for Lyme antibody, EBV and CMV IgM, and viral hepatitis markers. At no point did the patient notice a skin rash or a tick anywhere on his person.
Differential Diagnosis:
- Lyme Disease
- Anaplasmosis
- Ehrlichiosis
- Babesiosis
- Rocky Mountain Spotted Fever
- Viral Meningitis
- Bacterial Meningitis
- Leptospirosis

Laboratory Identification:
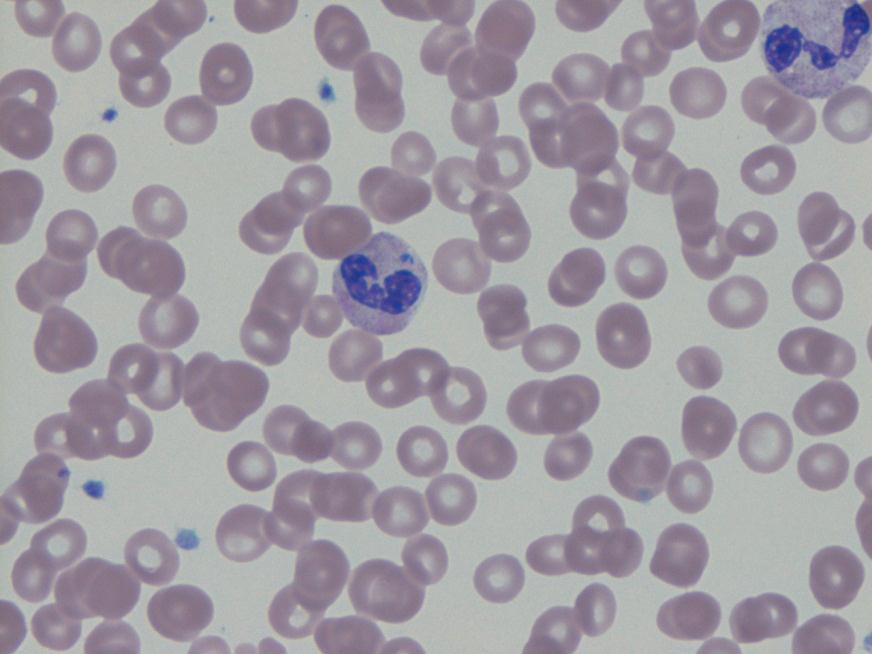
Anaplasma phagocytophilium was initially identified by PCR. Retrospectively, the blood smears originally examined for Babesia by both hematology and parasitology were reviewed. Both slides showed multiple granulocytes with intracytoplasmic morulae.
Discussion
Anaplasma phagocytophilium is the bacterium responsible for the tick-borne disease known as human granulocytic anaplasmosis. Anaplasma is transmitted to humans primarily through the bite of an infected Ixodes scapularis, the same species of tick which transmits Borrelia burgdorferi (Lyme disease) and Babesia spp. (human babesiosis). Anaplasmosis, Lyme disease, and babesiosis therefore share roughly the same geographical distribution in the United States with northeastern and upper midwestern states reporting the most cases.
Anaplasmosis most commonly presents about 1-2 weeks after a tick bite with the sudden onset of a variety of non-specific symptoms including fever, chills, headache, malaise, myalgia, nausea, and abdominal pain. Anaplasmosis, unlike other tick-borne diseases, rarely causes a rash. Routine blood tests may show thrombocytopenia, leukopenia, or elevated liver enzymes in some patients. Severe clinical presentations, more common in immunosuppressed patients, may include difficulty breathing, hemorrhage, renal failure or neurological problems. Anaplasmosis is estimated to be fatal in less than 1% of cases.
A routine blood smear is the quickest method for establishing an early presumptive diagnosis. Microscopic examination of the smear may reveal microcolonies of Anaplasma known as morulae within the cytoplasm of infected granulocytes. Ehrlichia, in contrast, will preferentially target and form morulae within monocytes. Because not all patients with anaplasmosis have visible morulae, this test is diagnostically insensitive and should be followed by further testing.
Confirmatory serologic testing for anaplasmosis includes an indirect immunofluorescence assay using an Anaplasma phagocytophilum antigen. For the highest sensitivity, this test should be performed on paired serum samples collected at least 2 weeks apart with the first sample taken as early in the disease as possible. A positive test will demonstrate a four-fold rise in antibody titers. Although it is a very sensitive detection method when run with paired samples, the lengthy testing time is less than ideal for patients requiring hospitalization for their disease.
A PCR assay on a sample of whole blood, although only available at a few reference laboratories, is the most efficient and accurate way to detect Anaplasma during the acute phase of the illness. The sample used for PCR testing should be taken before the initiation of antibiotic therapy as it causes the sensitivity of this test to rapidly decline.
Doxycycline is the first line treatment for adults and children of all ages with anaplasmosis as recommended by both the CDC and the AAP Committee on Infectious Diseases. Patients should be treated for at least 3 days after the fever subsides. Standard duration of treatment is 7 to 14 days. Therapy should be initiated immediately when there is a high clinical suspicion of anaplasmosis. A physician should never wait for the results of confirmatory testing to begin treatment. Most patients see improvement within 24-48 hours of treatment and non-response to doxycycline may indicate a different disease process.
Anaplasmosis, like many other tick-borne diseases, is a nationally reportable disease. All cases should be reported to local and state health departments as well as the CDC.
-Elaine Amoresano, MD, is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
