I walked into the autopsy suite, trembling and drenched in sweat, even though the atmospheric temperature was as cool as it could ever be. It was my second autopsy experience as a pathology resident and I could not make out exactly how I was feeling. My first session had exposed me to the critical role of pathologists in solving complex clinical puzzles and had left me shaken for days. And, I still wasn’t sure how the second session was going to be. But, one thing I was sure of was the fact that I still felt uncomfortable.
Not uncomfortable because of the task that had been given to us to find out the cause of death of the person I was going to meet. But I felt very uneasy with the fact that I did not know what to expect, yet again. The first session had been that of a middle-aged woman. This was going to be a case of a young man. Two different scenarios and diagnoses. I did not know what to expect. My stomach turned and churned and I could also feel my heart thumping loudly in my chest.
I looked up at my senior resident, with my attending physician observing our every move. He looked very comfortable with what we were about to do. He seemed to approach the entire situation like it was a routine procedure for him. I questioned myself, “would I ever get comfortable with doing autopsies like him?”
I listened attentively as the senior resident walked me through the process of performing an autopsy and what our duties as pathologists was supposed to be. I tried to listen as my senior colleague who was obviously very familiar with the process gave me a detailed lecture. I felt my mind wandering away, even though it seemed as though I was paying attention to what he was saying. My attention drifted back and forth as I couldn’t help thinking about so many other things including the complexities surrounding life and death.
As we went through the organs and finally began working on the lungs and heart were his primary pathologies were supposed to be, I was amazed at the pathology I was being exposed to. His bilateral lungs were severely fibrotic, encased with numerous calcified nodules that eventually turned out to be non-caseating granulomas. He also had calcified hilar nodules also confirmed histopathologically as non-caseating granulomas and his heart was markedly enlarged, with hypertrophy of biventricular walls, more prominent on the right side. His pulmonary arteries also showed signs of severe vascular disease with hyalinization and fibrosis. He had disseminated sarcoidosis, with his heart and lungs more severely affected. The sarcoid granulomas had spared the other organs and had domiciled in the lungs, with downstream effects on the heart. He fit the stereotypical case of cor-pulmonale-right sided heart failure from severe lung disease. The facts of the case suddenly began to make a lot of sense to me. I thus had a better understanding of why the patient had progressed so rapidly with his disease course with a fatal outcome.
I realized later that all my prior apprehension about performing the autopsy had been replaced by an interesting curiosity to find out more about his disease. My initial trepidation about performing that autopsy was quickly replaced by a determination to answer the “why” question. I became more involved and present with the procedure that by the time we left the autopsy suite, I thought I had learned something new that day.
That experience of being able to solve a clinical puzzle from autopsy findings made a huge impact on me. Therefore, the role of pathology and laboratory medicine in the advancement of medicine and patient care can never be overstated.
-Evi Abada, MD, MS is a Resident Physician in anatomic and clinical pathology at the Wayne State University School of Medicine/Detroit Medical Center in Michigan. She earned her Masters of Science in International Health Policy and Management from Brandeis University in Massachusetts, and is a global health advocate. Dr. Abada has been appointed to serve on the ASCP’s Resident’s Council and was named one of ASCP’S 40 under Forty honorees for the year 2020. You can follow her on twitter @EviAbadaMD.
The SARS-CoV-2 virus continues to cause increased infections and deaths around the world with considerable impact on clinical and laboratory medicine communities. Meanwhile, medical students and the medical community are also undertaking the yearly tribulation of residency interview season. Following the May announcement by the Coalition for Physician Accountability’s Work Group on Medical Students,1 the 2020 interview season will be entirely conducted utilizing virtual interviews. In pointed response to this change in format, residency programs rapidly scrambled to bolster websites, increase their social media presence, add virtual tours and prepare for the virtual interview format prior to the start of interview season. Now, at the midpoint of interview season, it is evident that some burdens of traditional on-site interviews are indeed being alleviated. Whether or not online resident socials and virtual tours can sufficiently substitute for all aspects of on-site visits and if the promise of increased spread of geographic and cultural diversity can be realized remains to be accurately assessed. The survival of the virtual format may even depend on this assessment.
The average cost of traditional on-site pathology interviews has continued to increase for medical students from a per person average of $3400 in 2015 to $4000 in 2020.2 Much of this expense comes from travel/transportation while some pathology programs provided accommodations. Additionally, interview season required about 20 total days away from medical school. To cover these expenses, about half (49%) of medical students borrow money for interviews . Not surprisingly, the majority of them agree that travel (79%) and lodging (65%) are overly burdensome components of interview season.2 Beyond accounting, the salient impact of these time and financial investments is that they were influencing the majority (58%) of interview decisions.
While the rising time and financial burdens of traditional on-site residency interviews were well-known and there was and continues to be a myriad of ideas3 on how to best address these concerns and the match overall, a small burgeoning literature on virtual resident interviews was available prior to the pandemic that showed promise for addressing these concerns.4,5 That is, in the 2020 – 2021 residency interview season, medical students are estimated to spend about 3.5 hours on an average virtual interview day instead of the 8 hour day of a traditional interview and through the elimination of travel time they may spend 7 less days on the interview trail. Thus, the cost of interviewing is also projected to be skeletonized to that of necessary professional clothing and computer hardware. Additional promising data from this small body of research suggests that 85% of virtual interviewees were satisfied with their understanding of the program and their ability to present themselves to residency programs.6 Furthermore, the fact that the residency program’s rank list showed no significant impact based on whether candidates interviewed virtually or in-person suggests that residency programs may feel capable of fairly assessing candidates.7
Beyond time and financial savings for pathology residency applicants and the assessment of candidates by residency programs and vice versa, the measurability of additional outcomes may be critical to the continuation of virtual resident interviews. In particular, there is great interest in online social events and interview day resident panels as a sufficient substitute for the naturally evolving casual conversations that occur during the dinners, lunches and tours available with on-site visits. Also, whether or not these socials combined with interviews with a small subset of faculty can accurately portray a pathology residency program’s culture. In prior surveys that compared in-person, virtual or a combined approach to interviews, candidates always favored in-person assessment when given the choice. The present circumstance will perhaps be the best attempt at an unbiased assessment of the perception of culture through virtual interviews. Last but not least, given the turbulent nature of race relations and culture in the United States over the last year combined with the ability of applicants to virtually interview without travel or financial restrictions, it will be absolutely critical to understand if virtual interviews portend to increase the spread of geographic and cultural diversity among applicants to pathology residency programs. That is, if current trends in resident recruitment can be altered from the current rate of 40 – 60% intraregional resident matriculation or whether the needs of financial and family assistance and/or intraregional familiarity are insurmountable.8 For if the potential for greater diversity is attainable in a significant manner that can be perpetuated into the future, it will be hard to argue for a return to the traditional format. That said, there will likely be bias in the data as an increasing number of pathology residency programs have heard the call to arms and are marching towards diversity, inclusion and equity through greater promotion, recruitment and retention efforts.9
In a tumultuous year that has included race relations reminiscent of the Civil Rights Era combined with a total number of worldwide pandemic deaths similar to the 1957 or 1968 influenza pandemics, medicine continues its steady progression toward improved healthcare and education for all. Following the May 2020 recommendations to implement virtual residency interviews, pathology residency programs moved expeditiously to bolster their websites, increase their social media presence, add virtual tours and prepare for the virtual interview format. Amid this tumult, the virtual interview format has already served to lessen the burdens of time and cost while also serving the practical needs of interview assessments for both medical students and residency programs. Yet, only time and methodical assessment will tell if the virtual interview format eliminates the impact of these burdens on residency decisions, allows both parties to adequately assess cultural fit and if the format and its advantages are here to stay. Regardless, it is imperative that the emphasis on diversity, inclusion and equity remains irrespective of future format.
References
The Coalition for Physician Accountability’s Work Group on Medical Students in the Class of 2021 Moving Across Institutions for Post Graduate Training Final Report and Recommendations for Medical Education Institutions of LCME-Accredited, U.S. Osteopathic, and Non-U.S. Medical School Applicants.
Pourmand, A., Lee, H., Fair, M., Maloney, K. & Caggiula, A. Feasibility and usability of tele-interview for medical residency interview. Western Journal of Emergency Medicine 19, 80–86 (2018).
Hammoud, M. M., Andrews, J. & Skochelak, S. E. Improving the Residency Application and Selection Process: An Optional Early Result Acceptance Program. JAMA – Journal of the American Medical Association 323, 503–504 (2020).
Chandler, N. M., Litz, C. N., Chang, H. L. & Danielson, P. D. Efficacy of Videoconference Interviews in the Pediatric Surgery Match. J. Surg. Educ. 76, 420–426 (2019).
Vining, C. C. et al. Virtual Surgical Fellowship Recruitment During COVID-19 and Its Implications for Resident/Fellow Recruitment in the Future. Ann. Surg. Oncol. 1 (2020). doi:10.1245/s10434-020-08623-2
Healy, W. L. & Bedair, H. Videoconference Interviews for an Adult Reconstruction Fellowship: Lessons Learned. Journal of Bone and Joint Surgery – American Volume 99, E114 (2017).
Vadi, M. G. et al. Comparison of web-based and face-to-face interviews for application to an anesthesiology training program: a pilot study. Int. J. Med. Educ. 7, 102–108 (2016).
Shappell, C. N., Farnan, J. M., McConville, J. F. & Martin, S. K. Geographic Trends for United States Allopathic Seniors Participating in the Residency Match: a Descriptive Analysis. J. Gen. Intern. Med. 34, 179–181 (2019).
Ware, A. D. et al. The “Race” Toward Diversity, Inclusion, and Equity in Pathology: The Johns Hopkins Experience. Acad. Pathol. 6, (2019).
-Josh Klonoski, MD, PhD, is a chief resident at the University of Utah, Salt Lake City, Utah, with a focus in neuroinfectious disease and global health. He has completed the first year of a neuropathology fellowship (out of sequence) and is in his final year of an anatomical and clinical pathology residency. Dr. Klonoski will return to the second neuropathology fellowship year in 2021 – 2022 and apply for a mentored clinical scientist research career development award (K08). The focus of his laboratory research is influenza and active projects include flu pneumonia, super-infections, encephalitis and oncolytic virotherapy.
If you’re as “plugged in” to the pathology and laboratory medicine community as I am, then you’ve been absolutely swimming in the explosion of new content and novel delivery this past year alone! A lot of it is a result of our unfortunate pandemic circumstance, but the pathology media-train has been gaining speed for quite a while now. Whether you’re a podcast addict, an enthusiastic virtual annual meeting participant (which is still open!), or if you’ve spent way too much time on Path Twitter, I’m right there with you!
I’ve talked here before about the power and impact of social media in our community, and I could drone on and on about its impressive potential and warn you about pitfalls, give you tips, or just celebrate success stories. But that’s boring. You may or may not have a social media presence, in which case I’d either be pandering to the choir, or putting you sound asleep. Well, I didn’t match into anesthesia, so let me give you the readers’ (tweeters’?) digest. ASCP has (yet again) taken a huge stride in making a presence in today’s increasingly digital age. Catalyzed by many things—pandemic included—many of the projects I have heard about among ASCP colleagues have started to magically materialize; enter the podcast. Among podcast media, ASCP’s Inside the Lab absolutely nails the archetype of what good podcasting is today! It’s a wonderfully curated series, highlighting super relevant topics, and is hosted by a fantastic team. But that’s not all! (wait, this sounds like a commercial, I’m drafting an email about promotional royalties right now…) Kidding. Sort of. Along with the topics, discussions, and guest panelists in the 7 episodes thus far, you can get continuing education credits!
Let me stop there. For emphasis. Imagine you’re driving to work. Sipping your coffee, sitting through traffic on the Dan Ryan Expressway (to those not in Chicago, we name them—we can talk more about this later). You suddenly remember you need CME/CMLE credits for your continuing ed maintenance. Great, you’ll just go hunting online for some boring QA/QC module about something somewhat related to your interests. Or… you could pop in those air pods and turn this podcast on for 1 AMA PRA credit a piece! Leave the murder mystery podcast for the drive home and spend the morning Inside the Lab! But I promised the readers’ digest, right? The following are highlights from a few of the currently available episodes for your listening and CE registering pleasure…
Image 2. Can’t have a good show, without good hosts. Dr. Milner, Dr. Mulder, and Kelly Swails are just that: excellent hosts and fantastic conversationalists who bring up interesting topics that go deeper into pathology and laboratory medicine. It makes for easy listening, easier CE, and provides the listener with a nice peek Inside the Lab. (Oh man, see what I did there?)
Hosted by Dr. Danny Milner (ASCP Chief Medical Officer and Global Health Champion), Dr. Lotte Mulder (ASCP Leadership and Empowerment extraordinaire), and Lablogatory’s very own Kelly Swails (digital managing editor in publications); the podcast has featured numerous amazing guests and topics ranging from testing logistics and interprofessional collaboration, to burnout and (obviously) COVID.
Episode 1: Disparities in COVID Cases Among Minorities
The inaugural episode featured Dr. Von Samedi (Associate Professor of Pathology at the University of Colorado School of Medicine), Dr. Valerie Fitzhugh (Associate Professor/Interim Chair of Pathology and Laboratory Medicine at Rutgers), and ASCP Social Media teammate Aaron Odegard (Infectious Disease MLS at Baptist Health Jacksonville). The inaugural topic (not a softball by any measure): how Black, Latinx, and minorities have suffered the brunt of COVID worse than other demographics. They discussed how COVID, at large, has uncovered swaths of long-standing, problematic disparities, and failures of our healthcare system. I gave a lecture on this topic when I was in New York as part of a CDC-funded, public health training seminar back in April of this (super long) year and things haven’t gotten any better—in fact from April to August when this episode aired, cases absolutely skyrocketed, especially in minority populations. The discussion’s bottom line: our community stands at a crossroads of education and delivery of results to both change the paradigm and improve the system. Good stuff. Listen here.
Episode 3: Online Teaching and Learning in Pathology and Laboratory Medicine
This cutting-edge episode featured our hosts talking to Dr. Sara Wobker (Assistant Professor in Pathology and Laboratory Medicine at UNC Chapel Hill), Dr. Natalie Banet (Assistant Professor of Pathology and Laboratory Medicine at Brown University), and Dr. Richard Davis (Regional Director of Microbiology for Providence Health Care in WA). The topic: how the pandemic has shunted all educational efforts into zoom meetings, virtual conferences, and online classes. Maybe this was happening already? The panelists talked about the old guard of education and the new way online learning has provided dynamic, flexible options for various students of all learning styles. Limitations, however, are clear when addressing pathology education—it’s not so easy to go virtual overnight and you can see the growing pains in every laboratory department. When you try to deliver old lessons across new platforms, things don’t work. So, in order to maintain relevance, engagement, and success educators must take into consideration different types of students, social determinants of learning, cultural backgrounds, accessibility, and inclusion for all. Highly relevant today. Listen here.
Episode 6: Pathology Research and Publication
Finally, I’ll end with a more recent episode. This one featured a panel that included (among their many other academic and clinical roles) Dr. Steven Kroft (Editor-in-Chief of the American Journal of Clinical Pathology), Dr. Roger Bertholf (Editor-in-Chief of Laboratory Medicine), and Dr. Sanjay Mukhopadyay (Associate Editor of the American Journal of Clinical Pathology). The topic for these well-published leaders in our field: how important it is to maintain a scientific standard, and how to get your paper published—yes you! They all talked about peer review, editing, submitting, and being able to tell whether paper’s are “good.” A seemingly subjective measure, but apropos of the year we’ve had which was filled with so many “bad” pieces of scientific literature. The benefits and limitations of peer-review are something we all have come to scrutinize as the digital age puts out clinical content ad nauseum on our social media feeds. But they all assert that one thing should be preserved as the future of scientific publication unfolds: the ability to create a standard by which professional societies, and medical subgroups and communities, collect and assess the science behind our work with purpose, accuracy, efficacy, and efficiency. It behooves editors as well as writers to enter a process that, ultimately, aims to improve the system as a whole—for the benefit of patients everywhere. Exactly how we are #StrongerTogether. Check it out here.
Image 3. You’re still here. It’s over. Go home. Go. Go listen to the podcast. Get your CE!
Check out these and the rest of the available episodes at www.ascp.org/insidethelab, Apple’s app store, Spotify, Google play, or wherever you listen to podcasts!
Thanks for reading, now go listen!
See you next time!
–Constantine E. Kanakis MD, MSc, MLS(ASCP)CM is a first-year resident physician in the Pathology and Laboratory Medicine Department at Loyola University Medical Center in Chicago with interests in hematopathology, transfusion medicine, bioethics, public health, and graphic medicine. He is a certified CAP inspector, holds an ASCP LMU certificate, and xxx. He was named on the 2017 ASCP Forty Under 40 list, The Pathologist magazine’s 2020 Power List and serves on ASCP’s Commission for Continuing Professional Development, Social Media Committee, and Patient Champions Advisory Board. He was featured in several online forums during the peak of the COVID pandemic discussing laboratory-related testing considerations, delivered a TEDx talk called “Unrecognizable Medicine,” and sits on the Auxiliary Board of the American Red Cross in Illinois. Dr. Kanakis is active on social media; follow him at @CEKanakisMD.
There are well over a hundred different cells types in the human body, and all those that have the ability to proliferate physiologically have the potential to succumb to uncontrolled cell division and thus generate a neoplasm. The tumors we most frequently encounter, like epithelial or hematologic disorders, are due to the higher proliferative rate of those cell types and the increased likelihood of an aberration or something going awry, i.e. mutations.2 Though we do come across many sarcomas and other mesenchymal tumors, this case study features a tumor derived from a cell type and structure that is rarely featured in cytology texts (an assumption, as I couldn’t find any information in the available prints within my department).
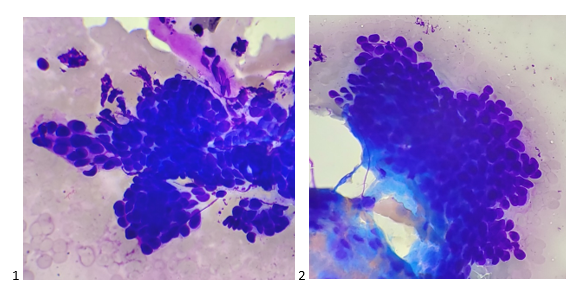
A 54 year old male patient presented to gastroenterology for severe cholecystitis. After undergoing a laparoscopic cholecystectomy, the pain subsided, but the patient was encouraged to follow up with a colonoscopy and upper endoscopy (EGD) due to his age. On the EGD, the gastroenterologist identified Barrett’s esophagus as well as a small, oval intramural lesion in the greater curvature of the gastric antrum, measuring 1.6 centimeters. The gastroenterologist was sharing the patient’s history with me when he described the endoscopic ultrasound findings of a well-defined hypoechoic and heterogenous lesion appearing to originate from the muscularis propria. His differential diagnoses based on imaging included a GIST, leiomyoma, or glomus tumor. The gastroenterologist did mention that the likelihood of this being a GIST or leiomyoma was very low. Despite lack of vascular structures visualized on Doppler imaging, the needle passes which I received to make air-dried Diff-Quik-stained smears were exceptionally bloody both grossly and microscopically.
I called my pathologist on cytology service for the day, informed him of the history presented to me by the gastroenterologist, and upon seeing the “rare atypical cells” through our telepathology platform, I hear him say, “a glomus tumor? Hmm, yes, it could be a glomus tumor.” You know that feeling when you’ve asked someone to repeat themselves three times and you still didn’t comprehend them, so out of courtesy, you pretend to know what they said and express understanding? Yet internally you are confused beyond repair?
I repeated back to the gastroenterologist, “he said it could be a glomus tumor!” Here comes the inner dialogue – what on earth is a glomus tumor? Why am I trying so hard to not look like an idiot right now? It’s okay to not know things, especially rare tumors that you’ve never come across. I have no idea what this tumor is, where it originates, what it consists of, this looks like a cohesive neuroendocrine tumor to me or even a basaloid squamous cell carcinoma. Obviously, it’s representative of the lesion, but I have no idea what a glomus (should I be pronouncing it with a long “o” or a short “o”?) is.
After screening the Pap-stained smears and H&E Cell Block sections the next morning, the cells still had cuboidal cells with features similar to a neuroendocrine tumor to me. The best I could call it was a neoplasm with neuroendocrine features before leaving the case with the pathologist on service to order immunostains.
IHC returned that afternoon, showing the neoplastic cells to be positive for SMA, focal weakly positive for synaptophysin, and negative for PanCK, CD34, desmin, chromogranin, CD45, DOG-1, HMB-45, and S-100 protein. Between the immunostains and the morphology findings, the case was signed out as a glomus tumor. Additional immunostains were performed showing the tumor cells are positive for vimentin and have a Ki-67 proliferation index of only 1%. When the tumor was resected two months after the initial FNA, pathology reported the findings as a 1.0 centimeter glomus tumor that was completely excised.
This tumor arises from the glomus body, which is a normal arteriovenous shunt that aids in regulation of temperature and blood flow in the body. Surrounded by smooth muscle tissue, the glomus body contracts and relaxes, closing and opening the shunt between the efferent venules and the afferent arteriole to pull blood flow away from the periphery and back into the body’s core or to allow heat dissipation. Glomus tumors are most often found in the dermis of the fingertips and toes, especially under nail beds due to the pain and cold sensitivity from exposure to cold.1,5 Glomus bodies are also found in the stomach as a thermoregulator (think cold food/liquids entering the digestive system), and account for 1% of mesenchymal gastric tumors.4 Most glomus tumors are benign and rarely undergo malignant transformation, and complete excision of these tumors typically provides immediate relief with little to no chance of recurrence.1,3
References
Fazwi, R., Chandran, P. A., & Ahmad, T. S. (2011). Glomus Tumour: A Retrospective Review of 15 Years Experience in A Single Institution. Malays Orthop J.,5(3), 8-12. doi:10.5704/MOJ.1111.007
Holly, J. M. P., Zeng, L., & Perks, C. M. (2013). Epithelial cancers in the post-genomic era: should we reconsider our lifestyle? Cancer and Metastasis Reviews, 32(3–4), 673–705. https://doi.org/10.1007/s10555-013-9445-5
Nascimento, E. F. R., Fonte, F. P., Mendonça, R. L., Nonose, R., de Souza, C. A. F., & Martinez, C. A. R. (2011). Glomus Tumor of the Stomach: A Rare Cause of Upper Gastrointestinal Bleeding. Case Reports in Surgery, 2011, 1–5. https://doi.org/10.1155/2011/371082
Papadelis, A., Brooks, C. J., & Albaran, R. G. (2016). Gastric glomus tumor. Journal of Surgical Case Reports, 2016(11), rjw183. https://doi.org/10.1093/jscr/rjw183
Uddin, M. M., Biswas, S. K., Rahman, M. H., Karmakar, N. C., Rahman, M. M., Alam, S. A. U., & Mondal, A. R. (2017). Sub-ungual Glomus Tumor: Study of 20 Cases. Faridpur Medical College Journal, 12(2), 64–67. https://doi.org/10.3329/fmcj.v12i2.34230
-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
A 31 year old woman, gravida 1 para 0, 35 weeks pregnant, arrived in the emergency room via ambulance following a fall down the stairs. The ER ordered a CBC, Type and Screen and a Kleihauer-Betke (KB) test and sent blood to the lab. The KB result was positive with 1.1 % fetal cells. Hypothetically, if this was an exam question, you might be asked, “How many doses of Rhogam should be administered?” But, before you grab your calculators, let’s explore that a bit.
Hemolytic Disease of the Fetus and Newborn (HDFN) has been described since the early 1600s, before blood groups were recognized. In the early 1900s, pioneers in blood banking, Landsteiner and Weiner, discovered the ABO and Rh blood groups, and, later, the Rh system became associated with HDFN. However, the antibody related etiology and pathogenesis of HDFN was not recognized until the late 1930s. Thus, the disease was written about in memoirs of midwives and physicians as early as 1609, but the mechanism involved was not described for another 300 years. The KB test was developed in 1957 by Enno Kleihauer and Klaus Betke to quantitate fetal maternal hemorrhage (FMH). The KB test allows physicians to diagnose and monitor and to initiate therapy to prevent the effects of HDFN. Finally, considered one of the most significant successes in medicine, prophylaxis for Rh HDFN, Rh immune globulin (RhIg), became available in 1968. The KB test is used to quantitate FMH in RhD negative mothers and the results can be used to calculate dosage for RhIg to prevent immunization. The KB test became one of the earliest examples of using a laboratory test to determine the appropriate dosage of a drug.1
KB testing has traditionally been used for RhD negative women to detect FMH and to determine the appropriate dose of RhIg to prevent immunization. In an RhD negative woman, we are concerned with immunization if the baby and mother are not antigenically similar. An RhD negative mother is given a prophylactic dose of RhIg at 28 weeks gestation. After delivery, when a newborn has a positive DAT and the fetal screen is positive, a quantitative test is needed to determine the appropriate dose of RhIg. In prenatal maternal trauma, there can also be a fetal bleed. Much as in childbirth, in a trauma, the baby’s blood can enter the mother’s circulation. This indicates placental hemorrhage and can be a prediction of preterm labor. In prenatal maternal trauma, the KB test has been used as aid in diagnosis and prognosis of HDFN, preterm labor and fetal demise. It can be used to determine if there has been a fetal bleed, and if so, to determine how much RhIg should be administered.
But, did you know that the KB test can also be used to determine FMH in RhD positive mothers? This is considered an alternative usage of the test. In the labs where I did KB tests, most fetal screens in Blood Bank were held until the following morning and performed on day shift. So, any KB tests on postpartum patients were also mostly done on day shift. I worked 2nd shift, and it was not uncommon to see KB tests ordered on RhD positive women. In fact, most of the KB tests ordered on 2nd and 3rd shift were from the ER and on RhD positive mothers. With RhD positive mothers, providers are not concerned with the mother producing anti-D, so RhIg is not a concern. Therefore, the answer to the hypothetical question posed above, is that this mother did not need any RhIg because, by checking the lab results it would be noted that this woman was Rh positive with a negative antibody screen.
A study performed in 2004 at the Shock Trauma Center, University of Maryland in Baltimore, reported that pregnant trauma patients with positive KB tests often had pre term contractions All patients in their study who experienced preterm contractions had positive KB tests. None of the patients with negative KB tests had uterine contractions. The conclusion was that “Kleihauer-Betke testing accurately predicts the risk of preterm labor after maternal trauma. Clinical assessment does not.” 2 They additionally concluded that, with a negative KB test, electronic fetal monitoring could safely be reduced. The major statement of the study, which has been incorporated into practice guidelines was that KB testing is important for all pregnant trauma patients, regardless of Rh status.2,3
In 2019 the College of American Pathologists Transfusion, Apheresis and Cellular Therapy Committee sent a survey with their proficiency testing program to determine how many participating laboratories perform KB tests on Rh positive pregnant females. 52% of the labs who responded noted that they performed quantitative fetal hemoglobin testing for RhD positive women, and about 39% reported performing more than 20 tests a year. The CAP group also reviewed literature detailing 16 observational studies and concluded that the literature supporting relying on the KB as a predictor of fetal distress was lacking evidence and nonconclusive. Despite the fact that doctors are ordering these and many laboratories are still performing this test STAT on RhD positive mothers, different guidelines for practice are mixed regarding if and how the KB should be used in these RhD positive trauma patients. Furthermore, many labs responded on the survey that doctors considered these results very important but that the labs were not sure how the results helped guide management of the mother or fetus.4
One of the problems some of these guidelines cite is that the KB test may not be rapid enough to use in trauma situations. Now, I have to start by saying that KB tests are probably no tech’s favorite test. The last hospital I worked at did KB tests in Hematology. Before that I worked at a hospital where we did KB tests in Blood Bank. There seems to be no way to avoid them! I would have to agree that a KB is not at all rapid. The test is both time sensitive, always ordered STAT, and very time consuming. Hands on time is considerable. I’ve gotten 2 in one night, on 2nd shift with only 4 or 5 techs manning the whole lab, and that makes for a busy night! Add a trauma or 2 to the mix, or a few units to wash for the NICU and you know why “Kleihaur-Betke” are not our favorite words.
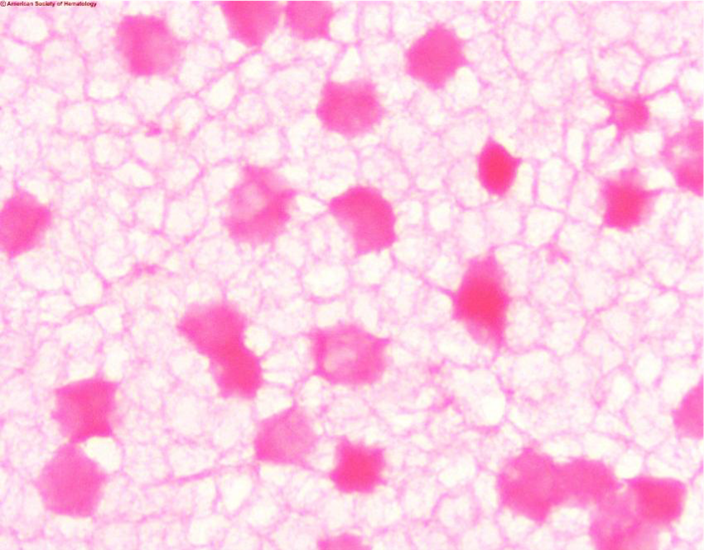
Another concern is that the KB test is marketed as a quantitative test. The problem with this is that it is not very precise due to technical difficulty. In the KB acid elution test the mother’s blood is treated with acid and then stained and counterstained. Fetal cells contain HbF which is resistant to acid and these cells will remain bright pink. The mother’s cells, which are primarily HbA, will appear as faint ‘ghost’ cells. 2000 cells are counted and the percent of fetal cells is determined. The test is complicated and needs precision in staining, counting and calculations. A slide that’s too thick, poor timing of steps, slides that are not adequately dried, or fetal cells that fail to stain can all affect results and cause false negative results. In pregnant women HbF may be increased, and in women with hemoglobinopathies such as sickle cell anemia and thalassemia Hb-F can be increased, leading to false positive results. As well, late in pregnancy it would be considered normal to have some fetal cells in the mother’s circulation. Thus, both false negative and false positive KB results are not uncommon, and a positive report on a KB test may not accurately predict fetal distress.
Image 1. Kleihauer-Betke stain showing dark ink fetal cells and ‘ghost’ like pale maternal cells
In the CAP survey article, it was noted that, of participating labs, about 96% did KB tests and 4% use flow cytometry.4 Flow cytometry is accurate, sensitive and reliable for HbF determination. Flow cytometry uses antibodies directed against fetal hemoglobin and antibodies directed against adult RBCs. A clear separation of populations can be identified and quantitated. Despite the fact that it is well known that flow cytometry is a much more precise test for FMH, many laboratories continue to do KB testing. This is likely due to the fact that only a small percentage of labs have flow cytometers. If, in trauma situations, physicians want HbF determination with a “fast” turnaround time, KB testing can be done in house with no equipment necessary. This is not fast, but would, in most circumstances, be faster than sending a test to a reference lab.
The KB test has historically been validated and used to estimate the total amount of FMH, and the results used to calculate if additional doses of RhIg are indicated. The test has high specificity for HbF but can be subjective. Precision between techs and even with the same tech repeating the test can be relatively low. Because of this, the formula used to calculate RhIg dosage has a factor built in to make up for any imprecision. An alternate usage of the test, and the one used in this case example, is to predict outcomes and guide treatment in maternal trauma victims, regardless of Rh status.
While there is some controversy on using the KB test in these cases, it is none the less still recommended by many authors and included in medical guidelines.5 Providers are using the KB test more and more for assessing placental hemorrhage in cases of trauma and premature labor. Though immunophenotyping by flow cytometry has a greater accuracy, the KB test can give reliable results at a lower cost and with a faster turnaround time.
As always, this blog led me off on several tangents while writing. When I have an idea for a blog, I start with a case study or an interesting sample I have seen in the lab. The case study itself is the easy part, then I start researching and reading articles about the disorder, test or phenomenon that I am writing about. Often, when I read one article, I ask myself another question and say, “what if…?” and that leads to another article and another and another. Days later I can still find myself reading articles and chasing after more information. I love my job, I love being a Medical Laboratory Scientist and educator, and in true form of the curious MLS, I always want to investigate and never want to stop learning. Thus, this simple case about an alternative usage of Kleihauer-Betke (KB) test kept developing as I wrote. As a side note, it was interesting to see that the studies have had different conclusions and the guidelines for this use of the KB test have swayed over the years. It will be interesting to see what the future will bring. I have seen some articles about adding the HbF determination to hematology analyzers—wouldn’t that be nice!
References
Reali G. Forty years of anti-D immunoprophylaxis. Blood Transfus. 2007;5(1):3-6. doi:10.2450/2007.0b18-06
Muench MV, Baschat AA, Reddy UM, Mighty HE, Weiner CP, Scalea TM, et al. Kleinhauer-betke testing is important in all cases of maternal trauma. J Trauma 2004;57(5):1094-8.
Michael V. Muench, Joseph C. Canterino, Trauma in Pregnancy, Obstetrics and Gynecology Clinics of North America, Volume 34, Issue 3, 2007, Pages 555-583.
Matthew S. Karafin, Chad Glisch, et al, for the College of American Pathologists, Transfusion, Apheresis, and Cellular Therapy Committee; Use of Fetal Hemoglobin Quantitation for Rh-Positive Pregnant Females: A National Survey and Review of the Literature. Arch Pathol Lab Med 1 December 2019; 143 (12): 1539–1544.
-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
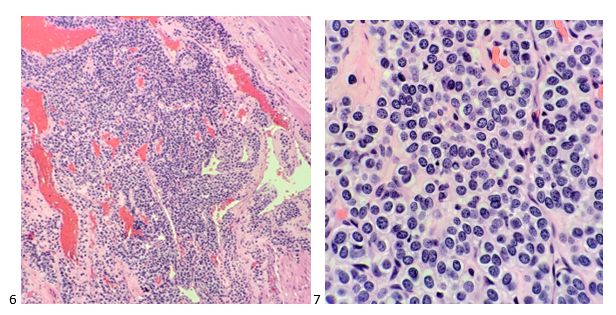
A 50 year old male with a significant past medical history of poorly controlled type 2 diabetes mellitus, hypertension, hyperlipidemia, smoking tobacco abuse and obstructive sleep apnea was referred to our institution’s pulmonology clinic for cavitary lung mass. The lung mass was incidentally discovered on chest x-ray and has been clinically stable on serial imaging for over two years; however, a previous extensive laboratory workup including computed tomography (CT) guided biopsy was unrevealing to its etiology. The patient was noted to be largely asymptomatic at his initial office visit; repeat diagnostic workup was ordered. CT chest imaging revealed a 2.8 x 1.9 x 2.0 cm cavitary lung mass in the posterior left lower lobe that was unchanged compared to outside CT imaging from approximately 4 months prior.
Image 1. Cross section (left) and Sagittal (right) views from CT chest without contrast revealed a 2.8 cm transverse by 1.9 cm anteroposterior by 2.0 cm craniocaudal stable mass-like opacity in the left lower lobe superior segment broadly abutting the posterior pleura with a tiny internal focus of cavitation.
Given the chronicity of the lung mass, atypical infection (Nocardia, endemic fungi, mycobacterium) and primary pulmonary cancer were highest on the differential diagnosis. Blood tests including endemic fungal serologies, QuantiFERON-TB Gold, cryptococcal antigen, galactomannan and Fungitell (1-3)-B-d glucan assay were negative. Given the unrevealing non-invasive workup, a repeat CT guided biopsy was performed and core biopsy samples were sent for AFB, fungal and Nocardia cultures as well as for histopathological examination.
Histopathology revealed necrotizing granulomatous inflammation with empty spherules of Coccidioides suggestive of a remote infection of long duration (Images 2, 3). Additionally, no microorganisms were isolated from cultures. Based on these findings, an infectious disease (ID) consult was placed. The patient remained asymptomatic and revealed a long history of residing within areas of the Southwestern United States endemic to Coccidioides species (sp.) during his ID office visit. Repeat Coccidioides complement fixation was positive for IgG (Titer: 1:4) with negative IgM by immunodiffusion testing. Urine Coccidioides antigen tested by quantitative sandwich enzyme immunoassay was negative. These findings likely represent past history of coccidiomycosis and not active infection. Antifungal therapy was deferred due to the patient’s asymptomatic status. The patient was monitored with close clinical follow up and continued serial imaging.
Histopathology Images
Image 2. Hematoxylin and eosin stained sections of formalin fixed paraffin embedded (FFPE) tissue from core biopsy of cavitary lung mass. Necrotizing granulomatous inflammation at 40X (A) and 100X (B) with empty spherules of Coccidioides (C, D) at 600X.Image 3. Special stains performed of formalin fixed paraffin embedded (FFPE) tissue from core biopsy of cavitary lung mass highlighting empty spherules. Grocott’s methenamine silver stain at 100X (A) and 400X (B). Periodic Acid Schiff for Fungus stain at 600X (C).
Discussion
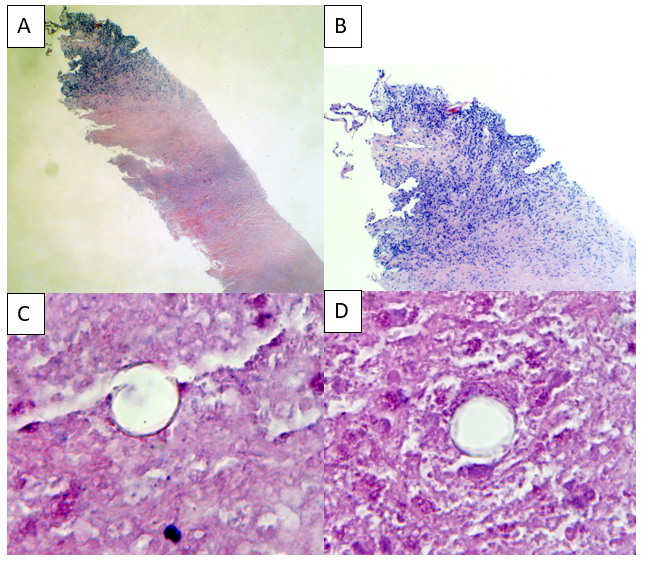
Coccidioides sp. are dimorphic fungi with a mycelial (saprophytic) phase in the environment and a spherule (parasitic) phase in its host.1 It is the cause of coccidiomycosis, also known as valley fever, desert fever or San Joaquin fever, which has a wide range of clinical presentations from subclinical manifestations (~60%) to an influenza-like illness followed by skin lesions to the most pathological form, disseminated disease.1 It can also cause the development of cavitary lung masses, as described in this case.1 It is endemic to the Southwestern region of the United States where it prefers dry, arid conditions.2 Infections normally occur by inhalation of infective arthroconidia, which have matured from mycelium, following disruption of soil.1 Once inside the host, lungs spherules containing endospores develop (Image 4).1 These spherules rupture releasing the endospores which can continue to develop into spherules to maintain a continuous parasitic cycle or can be exhaled into the environment to continue its saprophytic phase.1
Image 4. High magnification images of hematoxylin and eosin stained sections of formalin fixed paraffin embedded (FFPE) lung tissue revealing multiple spherules containing endospores (left) consistent with active Coccidioides infection and a giant ruptured spherule releasing endospores (right) that will continue to propagate Coccidioides infection.
Two morphologically indistinct species exist (C. immitis and C. posadasii) that can only be definitively identified by molecular methods.3C. immitis is predominantly found in central and southern California while C. posadasii can be found in other non-Californian southwestern US states and extending into western Texas and down throughout Mexico and South America.3 When cultured, it grows rapidly at both 25°C and 37°C into woolly white colonies that develop alternating barrel-shaped arthroconidia that can be seen on tape prep with lactophenol blue.4
References
Donovan FM, Shubitz L, Powell D, Orbach M, Frelinger J, Galgiani JM. 2019. Early Events in Coccidiomycosis. Clinical Microbiology Reviews, 33, e00112-19, DOI: 10.1128/CMR.00112-19
Hernandez H, Erives VH, Martinez LR. 2019. Coccidioidomycosis: Epidemiology, Fungal Pathogenesis and Therapeutic Development. Current Tropical Medicine Reports, 6, 132-144, DOI: 10.1007/s40475-019-00184-z
Kirkland TN, Fierer J. 2018. Coccidioides immitis and posadasii; a review of their biology, genomics, pathogenesis, and host immunity, Virulence, 9:1, 1426-1435, DOI: 10.1080/21505594.2018.1509667
Love GL, Ribes JA. 2018. Color Atlas of Mycology, An Illustrated Field Guide Based on Proficiency Testing. College of American Pathologists (CAP), p. 234-235
-John Markantonis is the current Medical Microbiology fellow at UT Southwestern and will be completing his Clinical Pathology residency in 2022. He is also interested in Transfusion Medicine and parasitic diseases.
-Dominick Cavuoti is a Professor at UT Southwestern and specializes in Infectious Diseases Pathology, Medical Microbiology and Cytology.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
A 20 year old Black male with a known history of HbS trait went to the primary care office for a pre-surgical evaluation for elective laparoscopic cholecystectomy for symptomatic cholelithiasis. All physical exam findings were negative. The patient had blood work completed and was found to have mild anemia with microcytosis. On previous imaging, the spleen was noted to be slightly enlarged. Further workup included a peripheral blood smear, finding target cells, microspherocytes, folded cells, and rod-shaped Hb C crystals (see image below). No sickled RBCs were noted.
Image 1. Peripheral blood smear with anemia, increased polychromatphilic RBCs, numerous target cells and rare HbC crystals
Discussion
Hemoglobin C disease is an intrinsic red cell disorder caused by Hemoglobin C (Hb C). Hb C is a variant of normal Hemoglobin A (Hb A) that results from a missense mutation in the β-globin protein, replacing the glutamic acid at position 6 with a lysine molecule. The disease can be either in the homozygous state (Hb CC) or in the heterozygous states (Hb AC or Hb SC). The origin of this mutation was traced back to West Africa and is found to confer protection against severe manifestations of malaria. In the United States, the Hb C allele is prevalent in about 1-2% of the African American population. There is an equal incidence between gender, and the incidence of the homozygous disease (i.e., Hb CC) is only 0.02%. Nevertheless, these statistics may be under-representative, since the disease is generally asymptomatic.
Heterozygous individuals with Hb AC usually show no symptoms, while homozygous individuals with Hb CC can have mild hemolytic anemia, jaundice, and splenomegaly. When Hb C is combined with other hemoglobinopathies, such as Hemoglobin S (Hb S), more serious complications can result. Hb S is similar to HbC in that it arises from a missense mutation; ie, a valine is substituted for the glutamic acid at the 6th position on the β-globin protein. As a result of this mutation, HbS abnormally polymerizes when in the presence of low oxygen tension, leaving the red blood cells (RBCs) rigid and irregularly shaped. Sickle cell disease (SCD) typically is a result of homozygous Hb S mutations (i.e., Hb SS), but the disease can also come from Hb SC.
All clinical features of Hb SS can be seen in Hb SC, including painful vaso-occlusive crises, chronic hemolytic anemia, stroke, acute chest syndrome, etc. Nevertheless, Hb SC is generally a milder disease. The complications from HbSC disease are less severe and less frequent when compared to Hb SS. Fortunately, unlike those with Hb SS disease, patients with Hb SC disease do not experience autosplenectomy, but they can develop splenomegaly. There are two complications that occur in HbSC disease occur more frequently than in HbSS disease, and they include proliferative sickle cell retinopathy and avascular necrosis of the femoral head (the latter case presents especially in peripartum women). Therefore, patients with HbSC disease should follow up with ophthalmology and obstetrics to monitor these complications. Furthermore, patients with Hb SC disease can vary in the severity of symptoms and the resulting complications. For example, some patients may develop a severe anemia and require blood transfusions; whereas, other patients are minimally affected by the disease. Overall, patients with Hb SC disease tend to have a better life expectancy compared to those with Hb SS disease. Patients with Hb SS disease have an average life expectancy of 40 years, while those with Hb SC disease are expected to live into their 60s and 70s. In contrast to Hb SS and Hb SC disease, Hb CC disease does not have an increase in mortality. As mentioned earlier, Hb CC disease results only in mild anemia, asymptomatic splenomegaly, and largely absent clinical symptoms.
Pathologic features of Hb SC and Hb CC diseases can be seen on a peripheral blood smear (PBS). Hb CC disease does not show sickled RBCs, while Hb SC can show sickled RBCs though very rarely. More importantly, Hb C is prone to polymerize into characteristic crystals. Depending on the zygosity of the individual, the crystals take on a defining shape. In heterozygous individuals (Hb SC), the crystals are found as irregular, amorphous, or bent appearing, and the RBCs can take on a “spiked and hooked” appearance. In homozygous individuals (Hb CC), the crystals are elongate, straight, and uniformly dense (as seen in the case above). In addition to crystals, the PBS shows numerous target cells, scattered folded cells, and microspherocytes.
Ancillary studies for diagnosis of these diseases include Hb variant analysis, such as electrophoresis and high-pressure liquid chromatography. Cellulose acetate (alkaline) electrophoresis is a standard method used to separate Hb A, Hb A2, Hb F, Hb C, Hb S, and other variants according to charge. Some hemoglobin variants comigrate using this described method, so citrate agar (acid) electrophoresis can be used additionally to distinguish between these variants. In Hb CC disease, analysis shows nearly all Hb C with small amounts of Hb F (i.e., fetal hemoglobin) and HbA2 (i.e., a normal variant of Hb A, in which the hemoglobin molecule is made up of 2 α chains and 2 δ chains). In Hb SC disease, analysis demonstrates almost equal amounts of Hb S and Hb C.
References
Aster JC, Pozdnyakova O, Kutok JL. Hematopathology: A Volume in the High Yield Pathology Series. Philadelphia, PA: Saunders, an imprint of Elsevier Inc.; 2013.
Gao J, Monaghan SA. Hematopathology. Chapter 1: Red Blood Cell/Hemoglobin Disorders. 3rd edition. Philadelphia, PA: Elsevier; 2018.
Karna B, Jha SK, Al Zaabi E. Hemoglobin C Disease. 2020 Jun 9. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan–. PMID: 32644469.
Mitton BA. Hemoglobin C Disease. Medscape, 9 Nov. 2019, emedicine.medscape.com/article/200853-overview.
Saunthararajah Y, Vichinsky EP. Hematology: Basic Principles and Practice. Chapter 42: Sickle Cell Disease: Clinical Features and Management. Philadelphia, PA: Elsevier; 2018.
-Amy Brady is a 4th-year medical student at the Philadelphia College of Osteopathic Medicine. She is currently applying to AP/CP pathology residency programs. Follow her on Twitter @amybrady517.
-Kamran Mirza, MD PhD is an Associate Professor of Pathology and Laboratory Medicine and Medical Education, and the Vice-Chair of Education in the Department of Pathology at Loyola University Chicago Stritch School of Medicine. Follow him on Twitter @KMirza.