In general, there are two reasons employees in the laboratory should care about proper waste disposal. Improper disposal is expensive. Laboratorians like raises, bonuses, and updated equipment, but there is less money for those things when paper items are tossed into sharps containers or when used gloves go into red bag trash containers. Labs in many states also risk large fines if items with biohazard symbols are disposed of into regular trash containers. The other reason to care about trash disposal involves the environment. Regulated Medical Waste (red bag trash and sharps) has to be treated, and some of it is incinerated while some ends up in special biohazard landfills. Both of those are things we want less of in our environment.
As a lab safety professional, you may know of several other reasons to implement and maintain proper lab waste segregation, but in my years of safety training, money and the environment are the two that tend to hit home with staff. There are multiple waste streams generated in the lab setting, and while management in some departments may choose to offer only biohazard waste receptacles for everything, the safety savvy professional knows this is wasteful and perhaps a bit lazy. With proper education and training, laboratorians are capable of goo trash segregation that meets the regulations and meets best practice standards.
Appropriate trash segregation in the lab requires knowledge about what waste goes into what type of container, and it requires availability and proper placement of those containers. If a processing department only uses red bag trash cans, for example, then much of the non-hazardous waste will end up there. Assess the laboratory areas for proper placement of all necessary types of waste receptacles.
In one lab, it was discovered that staff was throwing out urine containers with embedded needles into red bag trash containers. Why? There simply were no sharps containers in the area. It was a simple fix to move containers nearby, but no one was paying attention, and there could have been an unnecessary needle stick exposure. In another lab staff emptied urine sample cups into the sink and tossed them into regular trash bins. From a waste standpoint, that was fine, but because there was patient information on the container labels, HIPAA violations occurred.
Many venipuncture sample tubes used today are plastic, and they cannot be broken to create sharp edges. Given that, those items could be disposed of into biohazard trash bags. That can save a lab some money by reducing the volume of sharps containers used (they are more expensive to handle). However, glass specimen tubes are still available for purchase. Be sure to check for these in your racks before throwing out all lab tubes into a plastic bag. A broken tube can cause a very unfortunate exposure event.
Place patient information and extra labels into bins for shredding if available. Teach staff that in most cases it is acceptable to place used disposable lab coats and gloves into regular trash receptacles provided they are not visibly bloody. Other items can go into the regular waste stream such as plastic transfer pipettes, gauze pads, and paper towels (again, provided there is no blood visible on them).
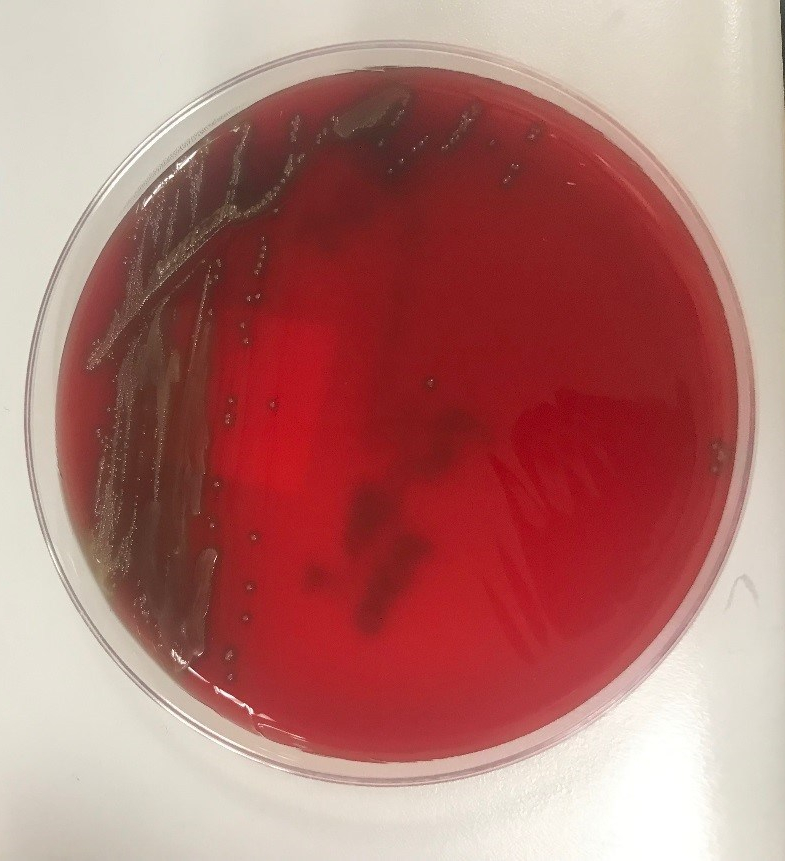
If items can be broken to create a sharp edge, they should be disposed of into a sharps container. That includes specimen cups made of hard plastic, sharp pipette tips, and any glass item. Agar plates and wooden applicator sticks should also go into a sharps container. Remember, if the item breaks while a trash bag is handled, an employee may become exposed, and the incident would need to be treated as an unknown source exposure, something that should always be avoided.
Make sure staff know the proper disposal of chemical waste as well. Never pour chemical waste down the drain unless your facility has a permit to do so. Place chemical waste containers in appropriate locations and label them according to EPA regulations. Provide proper training for employees who sign waste manifests when hazardous waste is hauled away from the lab. If you take the easy route and combine all of your laboratory waste, you would be responsible for both increased departmental expenses and for unnecessarily adding bio-waste to the environment. Talk regularly to your group of trained lab scientists about proper waste segregation, use signage as reminders, and assess their lab waste knowledge regularly. Proper waste management takes work. Mistakes can be made easily, and some of them can cause injury and invoke heavy fines. Invest in a robust laboratory waste management program to avoid those issues and to create a safety savvy example for others.

–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.