
I will continue this month along the thread of last month’s post, which addressed the controversy surrounding South African female mid-distance runner Caster Semenya. Caster has won many international mid-distance races (400-800m), but she has been suspected of naturally producing higher levels of testosterone.
Since last month, I’ve learned the reason for the higher testosterone is uncertain: it could be due to natural production (hyperandrogenism) or rumors of her being intersex1. Regardless, what I will discuss here is how the proposed actions of the International Olympic Committee would be expected to affect Semenya’s performance. Specifically, how would lowering testosterone levels affect her athletic performance?
Last month, we saw that muscle mass might be expected to decrease, but this may not affect athletic performance significantly.
Another important effect of testosterone is on red blood cell levels including hemoglobin, which by carrying oxygen to muscle is a central part of calculating VO2max. VO2max is maximal oxygen consumption. This is strongly linked to performance in cardiovascular athletic events.
Mid-distance running requires a large cardiovascular capacity. Maybe not the same level of Tour-de-France long distance bikers in the Alps, but still substantial. As a runner that feels pretty proud at having run a sub-3 minute 800m, I can say Caster’s feat of running it in less than 2 minutes is incomprehensible. From the burning feeling in my lungs and thudding, maximum heart rate at the end of the half-mile, I can attest that this event requires substantial cardiovascular efficiency.
Maximal oxygen consumption (VO2max) by exercising skeletal muscle is principally limited most by cardiac output and oxygen-carrying hemoglobin levels. This has been shown quite convincingly in a series of experiments in the 1950’s-70’s2,3 that probably wouldn’t be approved by the IRBs of today charged to protect research subject rights.
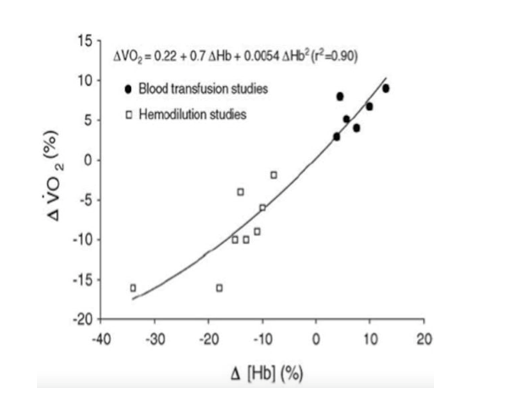
First, transfusing blood increased hemoglobin concentration and similarly the VO2max and exercise endurance of participants. (This practice was exploited most notably later on in the Tour de France). In other studies3, blood was removed from participants before assessing their exercise tolerance (10% loss of hemoglobin à 13% reduction in VO2max). Another study removed 400mL, 800mL and 1,200mL over several days, which decreased hemoglobin by 10%, 15%, and 18% respectively. There was a concomitant decrease in endurance time (-13%, -21%, -30%) and VO2max as well (-6%, -10%, -16%)3. A summary of blood transfusion and hemodilution studies is shown in Figure 1 from Otto JM et al4.
In transgender women (gender incongruent with sex assigned male at birth), hormone therapy to increase estrogen levels (oral estradiol) and block testosterone (anti-androgen: spironolactone) reduces hemoglobin by 9% on average (from 15.2 g/dL to 13.9 g/dL)5. I would expect a smaller decrease for Semenya as she will likely not get a full dose hormone regimen used for transgender transition and because her testosterone levels wouldn’t be as high as biologic males’. However, she would still be expected to have lower hemoglobin- similar to donating a half or whole unit of blood. If hemoglobin decreased even just 5%, that could affect her performance substantially when the difference between competitors boils down to seconds in mid-distance races.
Arguably, forced blood donation could produce the same effects as testosterone-lowering therapy. But it would be far too dramatic to suggest something like bloodletting by the International Olympic Committee.
In the end, I don’t feel qualified to say what should be done in this case. All I can say is that I don’t think lowering Caster Semanya’s testosterone levels will have the intended effect of decreasing muscle mass. On the other hand, it would decrease hemoglobin levels tempering her performance. But who should determine the point where her hormone levels should be? There is such a strong biologic connection between hormone levels and physiology that manipulating them for athletic fairness could be akin to playing puppeteer.
References
- North, Anna. ““I am a woman and I am fast”: what Caster Semenya’s story says about gender and race in sports” Vox. May 3, 2019
- BALKE B, GRILLO GP, KONECCI EB, LUFT UC. Work capacity after blood donation. J Appl Physiol. 1954 Nov; 7(3):231-8.
- Ekblom B, Goldbarg AN, Gullbring B. Response to exercise after blood loss and reinfusion. J Appl Physiol. 1972 Aug; 33(2):175-80.
- Otto JM, Montgomery HE, Richards T. Haemoglobin concentration and mass as determinants of exercise performance and of surgical outcome. Extrem Physiol Med. 2013; 2: 33.
- SoRelle JA, Jiao R, Gao E et al. Impact of Hormone Therapy on Laboratory Values in Transgender Patients. Clin Chem. 2019; 65(1): 170-179.

-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
