67 year old patient with a history of uterine carcinoma (leiomyosarcoma), presented with pancytopenia and history of B-12 deficiency. CBC showed
- WBC 4.1 K/ul
- RBC *2.37 M/ul
- Hgb *7.2 g/dl
- MCV 91.1 fl
- MCH 30.4 pg
- MCHC 33.3 %
- Platelets *25 K/ul
Peripheral blood differential count showed 3.5 % bands, 68.5 % Neutrophils, 3.5 % Eosinophils, 11.5 % Lymphocytes and 13.0 % Monocytes
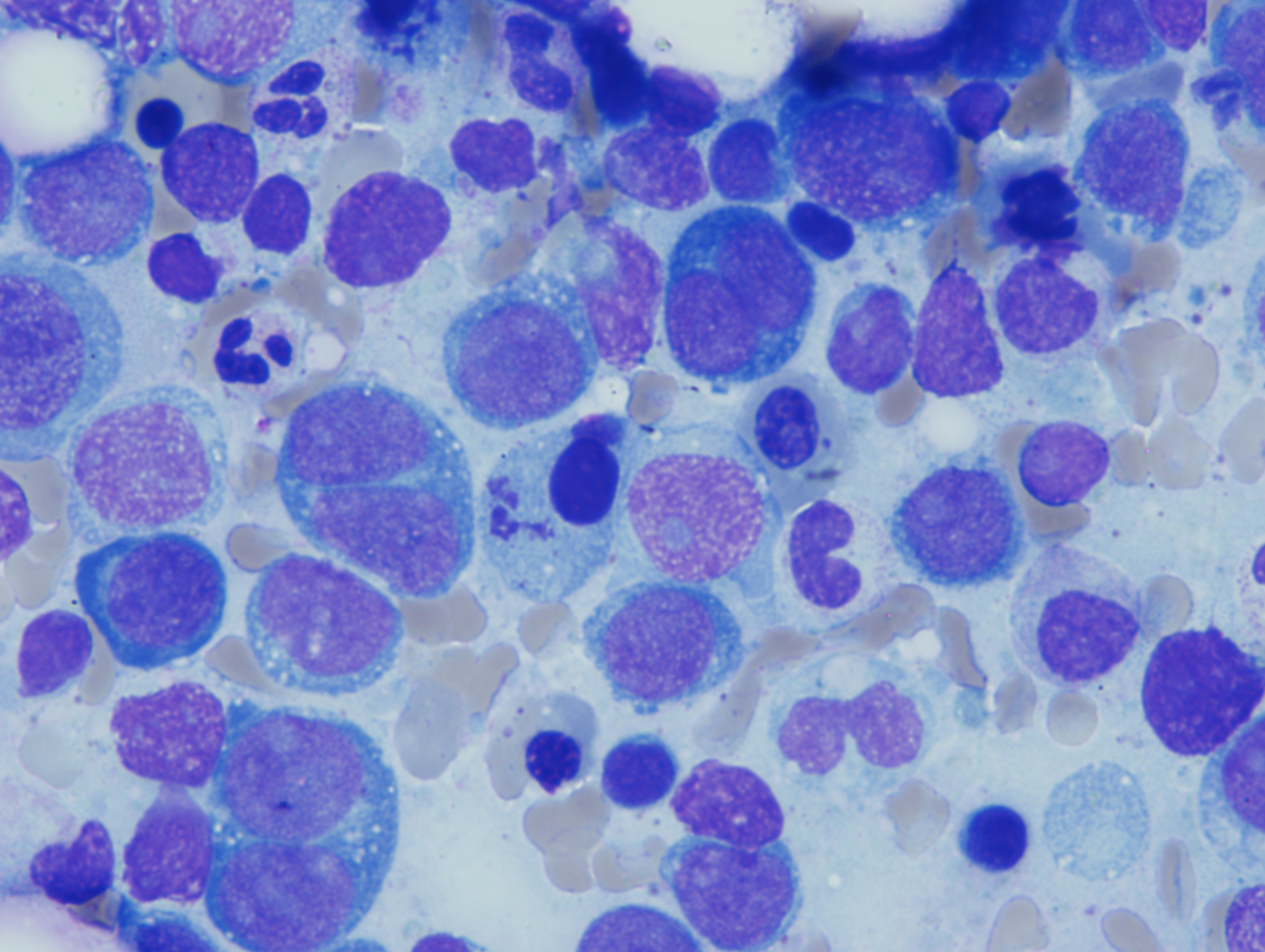
Bone marrow differential count of the bone marrow showed 65.0 % Erythroid Precursors with 48.4% erythroblasts and 7% myeloblasts
Several erythroblasts were seen, which often had overlapping morphological features with myeloblasts. Erythroblasts had slightly coarser nuclear chromatin compared to myeloblasts and often had deeply basophilic vacuolated cytoplasm. Erythroid maturation was markedly megaloblastic /dysplastic and left shifted with marked preponderance of erythroblasts. Dysplastic forms characterized by presence of precursors with irregular nuclear borders along with few multinucleated forms and gigantoblasts were present.
Cells counted as myeloblasts had high N/C ratio, finer nuclear chromatin with occasionally distinct 1 to 2 nucleoli and scant cytoplasm.

Discussion:
The current WHO classification subtypes acute erythroid leukemia into two categories based on the presence or absence of significant myeloid component.
Erythroleukemia or Erythroid/Myeloid (FAB subtype A – M6a) comprises of more than 50% erythroid precursors among all nucleated cell population of bone marrow and more than 20% myeloblasts among non erythroid cells.
Pure erythroid leukemia (FAB subtype B – M6b) comprises of more than 80% immature cells of erythroid lineage with no evidence of a significant myeloid component
The most common reactive process that can mimic acute erythroid leukemia is megaloblastic anemia caused by vitamin B12 and folate deficiency. Features associated with pernicious anemia are hemolysis with increased mean corpuscular volume (MCV), hypersegmented neutrophils, leukopenia and thrombocytopenia increased LDH and urobilinogen. Bone marrow findings show hypercellular marrow witn marked erythroid hyperplasia. Other non-neoplastic diseases mimicking acute erythroid leukemia are post-chemotherapy recovery, parvovirus infection, drug effect, heavy metal intoxication and congenital dyserythropoiesis. A detailed clinical history, laboratory work up, peripheral blood and bone marrow examination, cytochemical, immunoshistochemical, flow cytometry, cytogenetic and molecular studies are required for the diagnosis of acute erythroid leukemia.
The oncologist was contacted and it was confirmed that B12 was repleted before the bone marrow study was performed. Diagnosis of acute erythroid /myeloid leukemia was only made after it was confirmed with the oncologist that patient was not B12 deficient at the time of the study.

-Neerja Vajpayee, MD, is an Associate Professor of Pathology at the SUNY Upstate Medical University, Syracuse, NY. She enjoys teaching hematology to residents, fellows and laboratory technologists.