Dr. Diamond from the Washington University School of Medicine talked with Lab Medicine about all things Zika Virus: a brief history of the virus, modes of transmission, and the implications for laboratory professionals and pathologists.
Tag: microbiology
Microbiology Case Study: An 84 Year Old Man with Weakness and Back Pain
An 84 year old man with atrial fibrillation, coronary artery disease status post bypass surgery, and type II diabetes with chronic peripheral neuropathy presented to the ED with weakness, multiple falls, back pain, chills, and confusion. He was found to have a fever of 102o F. A workup for sepsis was performed but no source of infection was identified. Blood cultures were drawn and the patient was started on broad spectrum antibiotics. Fevers, chills, and confusion improved but patient continued to have back pain. A CT scan showed a pathologic fracture of L3 vertebrae, presumed to be secondary to infection with adjacent myositis.
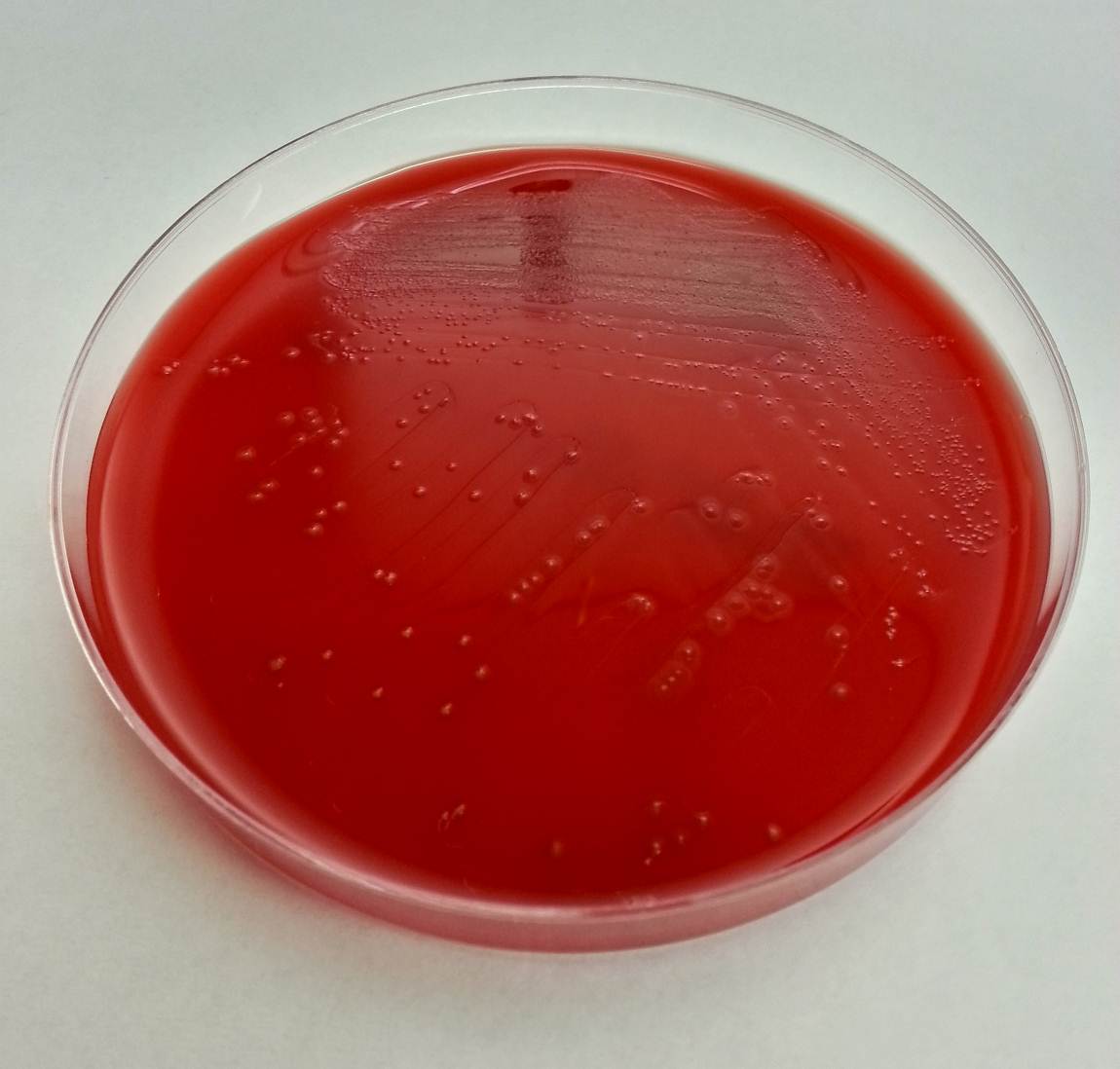
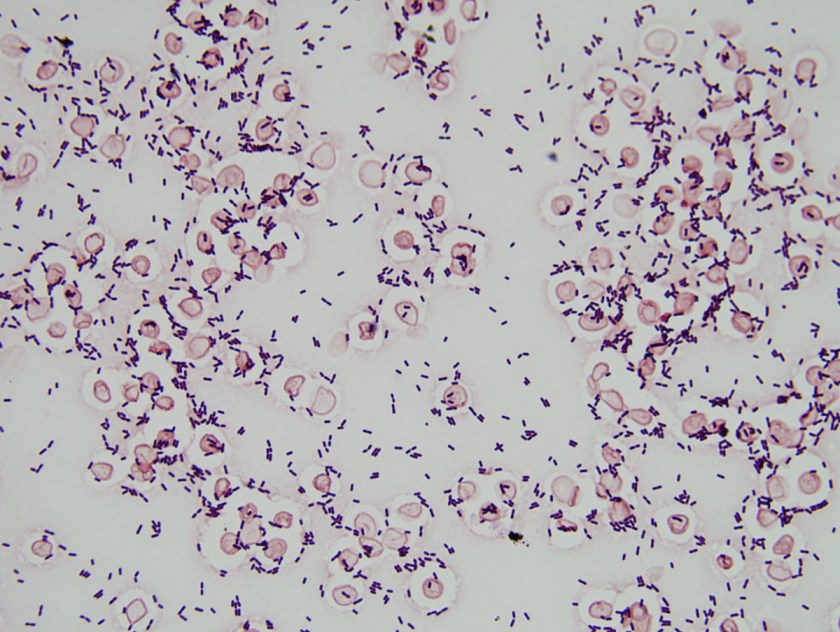
Multiple blood culture bottles were positive for the organism with the following Gram smear morphology and colony morphology on blood agar.


Laboratory Identification:
Gram smear showed Gram negative cocobacilli. The colonies were gray-white on blood agar, colorless on MacConkey and oxidase negative. The organism was identified as Yersinia pseudotuberculosis by MALDI-ToF and confirmed by VITEK.
Discussion:
Yersinia pseudotuberculosis is a gram negative bacillus that belongs to the Enterobacteriaceae family and therefore ferments glucose, is oxidase negative, and can reduce nitrates to nitrites. This bacterium is endemic in a wide variety of animals and is presumed to be a possible foodborne pathogen due to similarities to Yersinia enterocolitica. There have been reported cases of outbreaks associated with milk and iceberg lettuce sprayed with untreated water. Growth is optimal at 25-32o C, but can grow at 4o C. Infection is rare but typically causes enterocolitis and ileitis. Children may present with mesenteric lymphadenitis, which may mimic acute appendicitis. Sepsis is rare but is associated with those with underlying disorders such as cirrhosis, hemochromatosis, and diabetes. Reported mortality rates may be as high as 75% despite proper antibiotic treatment.
In this patient, it was determined that the most likely source of infection was consumption of raw milk. Due to presumed vertebral and paravertebral soft tissue involvement, he was treated with six weeks of IV ceftriaxone.
-Joanna Conant, MD is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Microbiology Case Study: Young Girl with Community-Acquired Pneumonia
A young girl presented to the emergency department with 6 days of cough, congestion, and intermittent fever up to 102°F. Respiratory viral testing, blood cultures, and a chest x-ray were ordered. The patient was found to be RSV positive and sent home with oral steroids. Two days later she presented the emergency department once again with worsening respiratory symptoms and a positive blood culture with the following organism (Figure 1).

Our patient developed a Streptococcus pneumoniae superinfection and bacteremia in conjunction with RSV pneumonia.
Identification
S. pneumoniae is a Gram-positive cocci that forms “lancet” shaped pairs on Gram stain (Figure 1). Due to pretreatment with antibiotics, our Gram stain shows some pairs, but many Gram variable chains of cocci as well. S. pneumoniae grows as alpha hemolytic colonies on 5% sheep blood, chocolate, and CAN (colistin nalidixic acid) agar in 12-18 hours, where it forms umbelicated colonies with a characteristic navel-like depression in the middle due to autolysins produced by the bacterium. Some serotypes of S. pneumoniae, primarily serotype 3, have a mucoid phenotype seen in Figure 3. S. pneumoniae is a member of the Streptococcus mitis group, but due to its pathogenic potential it has always been singled out. This is accomplished using two biochemical tests: bile solubility testing with 10% deoxycholate, which dissolves colonies of S. pneumoniae but not those of other Viridans group streptococci, and optochin disc testing, to which S. pneumoniae is sensitive while other Virdians group streptococci are resistant (Figures 2 and 3). Many molecular assays have trouble differentiating S. pneumoniae from S. mitis group due to their similarities on a nucleotide and protein level, so biochemical testing is still a mainstay of organism identification.


Clinical Significance
S. pneumoniae is known to cause a variety of clinical manifestations in children, from community acquired pneumonia and acute otitis media to bacteremia and meningitis. S. pneumoniae is also a colonizer of the upper respiratory tract; approximately 21% of children in developed countries and 90% of children in developing countries are asymptotically colonized. Due to the high rates of S. pneumoniae colonization in children, direct urine antigen testing is inappropriate, as it cannot distinguish asymptomatic carriage from invasive disease. S. pneumoniae direct antigen detection from CSF has been shown to have < 30% sensitivity and offers no benefit over a routine cytospin Gram stain.
Vaccination in children
Around 2000 the first S. pneumoniae vaccine became available. PCV7 was a heptavalent conjugate vaccine which provided protection from the 7 most common S. pneumoniae serotypes known to cause invasive disease (4, 6B, 9V, 14, 18C, 19F, and 23F). Routine vaccination of children was a huge success which reduced the incidence of invasive pneumococcal disease attributed to vaccine strains by 99%. An indirect benefit of the PCV7 vaccine was that adults >65 years of age saw a 92% decrease in invasive pneumococcal disease caused by PCV7 serotypes, despite not being vaccinated themselves, because of reduced transmission of S. pneumoniae from children to adults. Due to the selective pressure of the vaccine, non-vaccine serotypes of S. pneumoniae such as 19A subsequently became the predominant causes of invasive streptococcal disease. In 2010, a 13-valent pneumococcal conjugate vaccine (PCV13) was FDA approved. It includes all seven S. pneumoniae serotypes contained in PCV7, plus six additional serotypes (1, 3, 5, 6A, 7F, and 19A). PCV13 provides coverage against 2/3 of all serotypes responsible for invasive pneumococcal disease in children under 5 years of age.
Follow up
The patient had an uneventful hospital stay. All subsequent blood cultures were negative and susceptibility testing found the patient’s S. pneumoniae isolate to be susceptible to penicillin, cefotaxime, and clindamycin. The patient and was discharged home after 24 hours of observation with a 7 day course of amoxicillin.
References:
- Manual of Clinical Microbiology, 11th edition
- Pediatric Red Book, 2015 Report of the Committee on Infectious Diseases, 30th edition

-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
Mycobacterium chimaera Infections in Cardiac Surgery Patients
A group of physicians from the University of Iowa have started a dialogue about Mycobacterium chimaera infections in patients who have undergone cardiac surgery. It seems as though the bacteria finds its way to the patients via a heater-cooler device used during their procedure. If you’re a micro tech or a pathologist and you come across a cardiac patient who has a fever of unknown origin, night sweats, loss of energy, and failure to gain weight, M. chimaera is something to keep in mind.
You can read more about this issue in the original blog post from the Iowa infectious disease doctors, Maryn McKenna’s write up over at Nat Geo, and the CDC guidance paper.
Microbiology Case Study: 45 Year Old Woman with Subarachnoid Hemorrhage
Case History:
A 45 year-old woman was hospitalized for a bilateral subarachnoid hemorrhage with right-sided intraventricular hemorrhage secondary to a basilar artery aneurysm. On hospital day 2, after endovascular coiling of her aneurysm, she developed seizure-like activity. She was found to have new bilateral thalamic and brainstem infarcts with increased hydrocephalus and had an external ventricular drain placed.
She showed some minimal neurological improvements over the next 2 weeks until hospital day 17 when her mental status acutely declined and she developed a fever, leukocytosis, and meningeal signs. 8cc of cloudy, yellow fluid was collected via lumbar puncture. Analysis of the fluid showed pleocytosis (cell count of 54K) with a neutrophil predominance and markedly elevated protein.




Laboratory Identification:
Initial review of the spinal fluid gram stain showed many polymorphonuclear leukocytes and what appeared to be paired gram negative cocci suspicious for Neisseria meningitidis. However, many organisms lacked the more characteristic “kidney-bean” shape. Further inspection of the gram stain revealed many gram negative organisms which more closely resembled bacilli. Given the patient’s history and clinical course, it was determined the pathological agent was most likely a gram negative coccobacillus. On culture, the bacteria formed smooth, round, opaque colonies on Blood and Chocolate agar and was lactose non-fermenting on MacConkey agar. The bacterial colonies were also oxidase negative.
Mass spectrometry identified the organism as Acinetobacter radioresistens.
Rare gram positive appearing organisms of similar shape were also located on the gram stain. This demonstrates that Acinetobacter is known to occasionally retain the crystal violet stain leading to cases of initial misidentification.
Discussion:
Acinetobacter radioresistens is one of about 30 species of bacteria included in the Acinetobacter genus. Acinetobacter is characterized as a gram negative, aerobic coccobacillus which is non-motile, non-fermentative, and oxidase-negative. It grows well on standard aerobic media and typically forms smooth, round, mucoid colonies at 37°C. Acinetobacter is a water organism which preferentially colonizes aquatic, humid, and tropical environments; perhaps accounting for the increased incidence of Acinetobacter infections between the months of July and October.
While there have been reported cases of community-acquired Acinetobacter pneumonia in Southeast Asia and Australia, in most areas of the world Acinetobacter is known primarily as an agent of nosocomial infections. Studies show that an estimated 33% of healthcare workers are colonized with Acinetobacter and that it is one of the most prevalent bacteria isolated from the white coats of medical students. Despite its ubiquity in hospitals, Acinetobacter infections are relatively rare. Many patients may be colonized with it, but Acinetobacter only usually causes disease in immunocompromised and/or critically-ill patients with long hospitalizations. At particular risk are ventilated patients supported with multiple lines, drains, and catheters. Acinetobacter is reported as the pathological agent in a small percent of ventilator-associated pneumonias, central line-associated bloodstream infections, catheter-associated urinary tract infections, and surgical site infections. It is also recognized as a cause of nosocomial meningitis in neurosurgical patients with external ventricular drains, especially those with a history of intracranial hemorrhage and recent prior antibiotic therapy.
Acinetobacter infections are of particular concern because several species demonstrate resistance to many antimicrobials. Acinetobacter baumanni, the species responsible for the majority of Acinetobacter infections, has demonstrated resistance to 1st-3rd generation cephalosporins, macrolides, penicillins, and aminoglycosides. Because these infections are robust and difficult to treat, patients with Acinetobacter infections have a 25-75% mortality risk depending on the site of their infection and their baseline cardiopulmonary and immune status. Currently, carbapenems are considered the gold standard treatment.
-Elaine Amoresano, MD, is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Microbiology Case Study: Immunocompromised 65 Year Old Man
Case History:
A 65 year old man presents to the emergency room with acute onset back pain. Of note, the man was diagnosed with Burkitt’s lymphoma two months prior and had recently received a course of chemotherapy. During the workup for his back pain, a chest CT is obtained and reveals a 2 cm pulmonary nodule in the left upper lobe with a surrounding “groundglass halo” highly suspicious for invasive fungal involvement. A fine needle aspiration (FNA) of the nodule is performed and tissue is sent for histopathologic examination as well as bacterial and fungal culture.

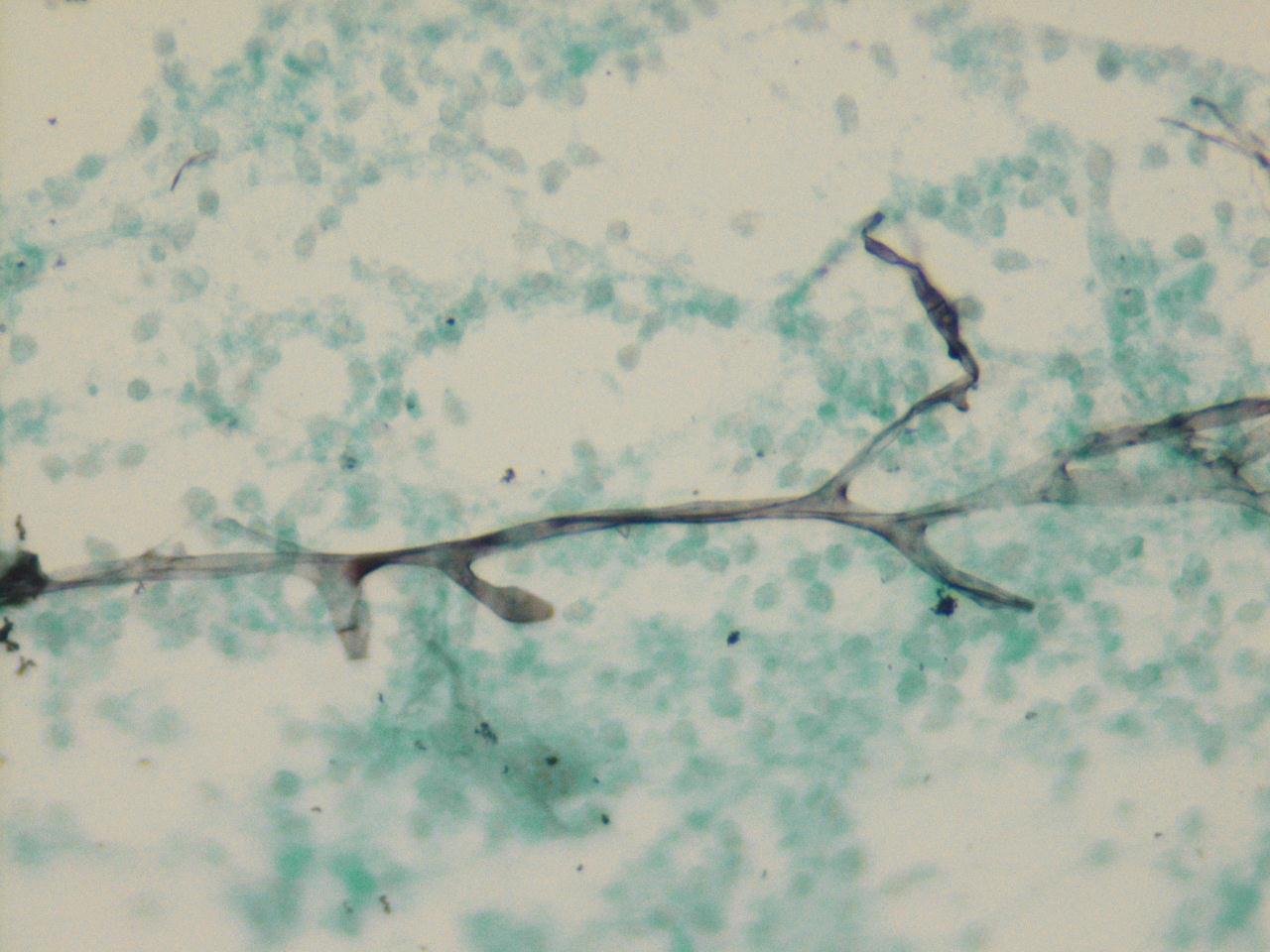

Laboratory Identification:
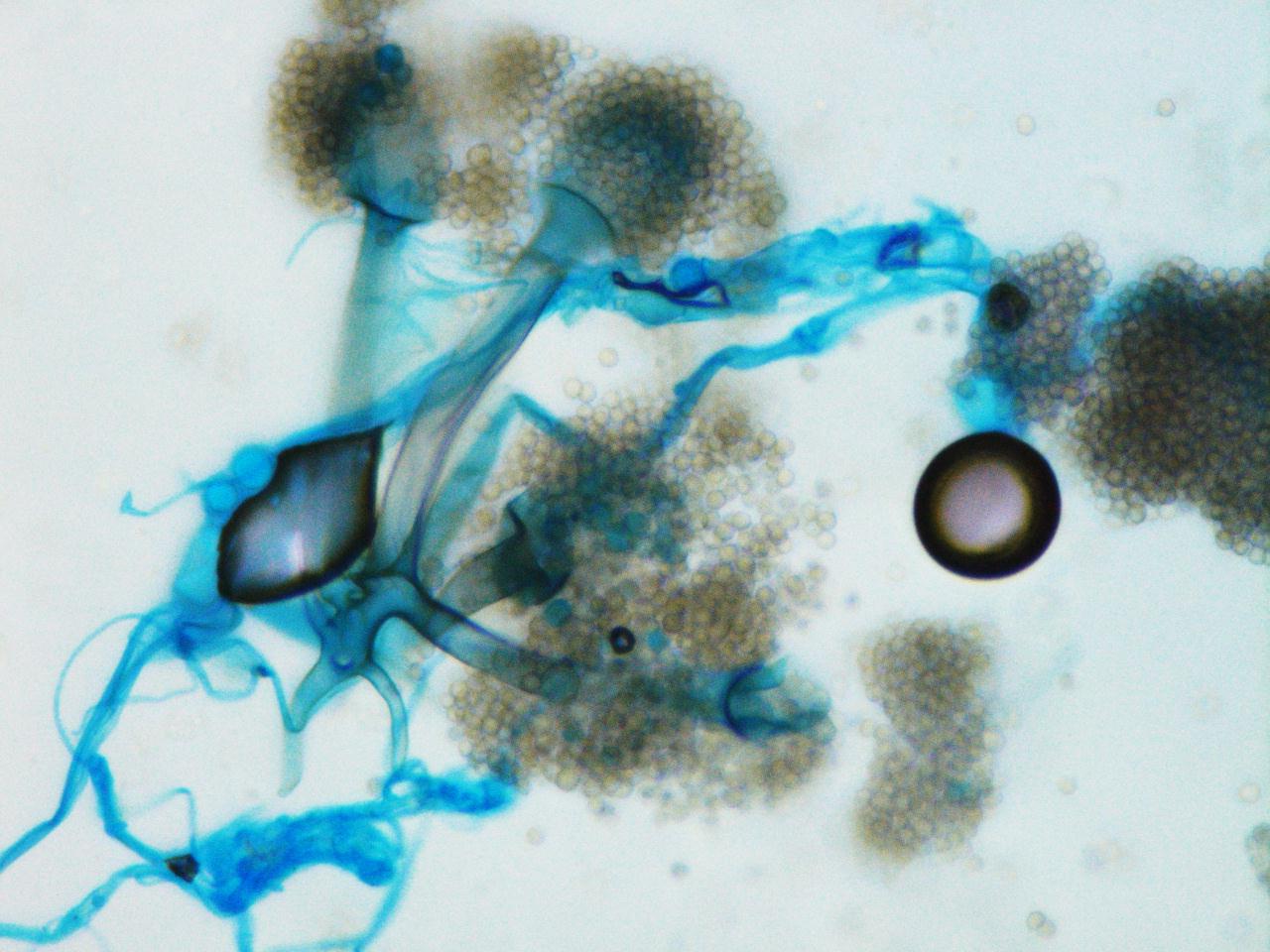
One rapidly growing white colony was identified that became grey over time. The colony was a “lid-lifter” that began pushing at the lid after only a few days. Microscopically, the organisms had broad hyphae with single and branching sporangiophores. At the ends of the sporangiophores there were pyriform, or pear-shaped, sporangia sitting atop funnel-shaped apophyses. Rhizoids were found to be internodal, or arising from the hyphae between the sporangiophores. Based on this morphology, the fungal organisms were identified as Lichtheimia corymbifera complex (formally Absidia corymbifera).
Discussion:
Lichtheimia corymbifera is an organism within the phylum Zygomycota and is one of two pathogenic species in the genus Lichtheimia. This organism is known as an uncommon cause of Zygomycosis and is only implicated in approximately 5% of cases. As in most cases of Zygomycosis, exemplified in our patient, Lichtheimia corymbifera most often affects immunocompromised patients. It is ubiquitous in the environment and is associated with decaying plant matter and soil. Disease is caused by inhalation of spores.
Important points for laboratory identification:
Lichtheimia
- Growth at 35-37°C (capable of growth up to 50°C)
- Inhibited by media containing cycloheximide
- Internodal rhizoids
- Pyriform sporangia
- Apophysis
Compared to other common Zygomycetes:
Mucor
- No rhizoids
- Round sporangia
- No apophysis
Rhizopus
- Nodal rhizoids (directly opposite of the sporangiophores)
- Round sporangia
- No apophysis
-Britni Bryant, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Microbiology Case Study: 4 Year Old Girl with Diarrhea
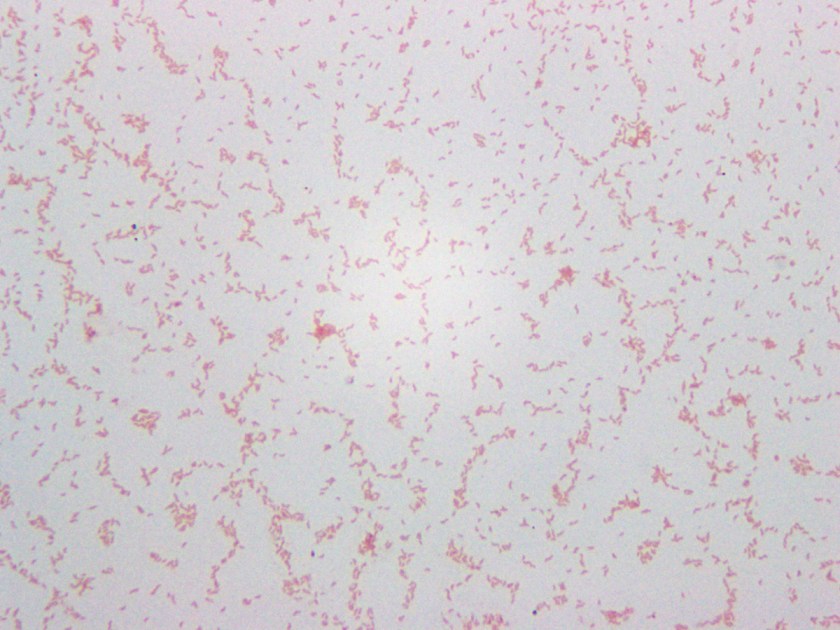
A 4-year-old girl with no past medical history had been feeling unwell for one day following a barbecue she had attended a few days prior. Her symptoms worsened to include colicky abdominal pain and bloody diarrhea, with as many as eight bowel movements per day. This persisted for the following two days; thereafter, she presented to the hospital also complaining of fever, nausea, and vomiting. She was found to be dehydrated and pale on exam, and was admitted for intravenous rehydration. Fecal leukocyte testing and stool cultures were sent. A Gram stain of the pathogen isolated from stool culture is shown in Figure 1.
An infectious etiology is highly suspected given this patient’s presentation, leading to work-up with fecal leukocytes and stool cultures. The presence of fecal leukocytes, which was positive in this patient, is a strong indicator of inflammatory diarrhea. Bacterial stool culture allows for detection of Salmonella, Shigella, Campylobacter, E. coli O157:H7, Yersinia, Aeromonas, and Plesiomonas.
Many different culture mediums are used to isolate bacterial gastrointestinal pathogens. In addition to the routine 5% sheep blood agar and MacConkey agar, a case of infectious diarrhea requires further workup to rule out the above mentioned pathogens. Sorbitol-MacConkey agar is a variant of traditional MacConkey agar, and is used to detect E. Coli O157:H7, which differs from other E. coli strains by its inability to ferment sorbitol, thus forming colorless colonies on this media. Xylose lysine deoxycholate (XLD) and hektoen enteric (HE) agars are utilized for the selection and differentiation between Salmonella and Shigella. A sweep of bacteria growing on the blood agar plate and subsequent oxidase testing is used for detection of Aeromonas and Plesiomonas, which are oxidase positive organisms unlike normal fecal flora which is oxidase negative. Cefsulodin-irgasan-novobiocin (CIN) agar is used for the selection and differentiation of Yersinia, which utilizes inhibitory substances (cefsulodin, irgasan, novobiocin, bile salts, and crystal violet) to prevent the growth of most bacteria. The agar also contains a pH indicator that turns red or pink when mannitol is fermented; with Yersinia having a characteristic ‘bull’s eye’ colonies with red centers and clear edges. CIN is incubated at room temperature for 48 hours. Finally, Campy CVA agar is a selective media for Campylobacter containing antimicrobial agents cefoperazone, vancomycin, and amphotericin B (CVA) which inhibit normal fecal flora. This media is incubated at 42°C under microaerophilic conditions, which support the growth of Campylobacter jejuni and C. coli.
Our patient’s culture grew gray, non-hemolytic colonies on Campy CVA agar (Figure 2). The organism was identified as Campylobacter jejuni by MALDI-TOF MS (matrix-assisted laser desorption/ionization, time of flight mass spectrometry).

Campylobacter are gram-negative, microaerophilic, curved or spiral rods in the family Campylobacteriaceae. They are widely distributed in animals and infection is most often transmitted by contaminated foods, particularly undercooked chicken. The species most commonly associated with human infections are C. jejuni and C. coli, with C. jejuni accounting for the large majority. Infection with C. jejuni has been linked with subsequent development of Guillain-Barre syndrome two to three weeks following the initial illness. Our patient improved following two days of IV fluids and antibiotics with no subsequent follow up after discharge.
References:
Manual of Clinical Microbiology, 11th edition
-Said Albahra, MD, 1st year Anatomic and Clinical Pathology resident at the University of Texas Southwestern Medical Center.
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
Microbiology Case Study: 58 Year Old Man with Fatigue and Chills
Case History:
Two weeks after returning from a camping vacation in Cape Cod, a 58 year old man presented to the emergency room with six days of fatigue, fever, chills, arthralgia, myalgia, mild right upper quadrant pain, and a frontal headache. Clinical workup revealed worsening leukopenia, thrombocytopenia, and elevated transaminases when compared to preliminary testing done by the patient’s primary care provider at the onset of his symptoms. His preliminary workup was also negative for Lyme antibody, EBV and CMV IgM, and viral hepatitis markers. At no point did the patient notice a skin rash or a tick anywhere on his person.
Differential Diagnosis:
- Lyme Disease
- Anaplasmosis
- Ehrlichiosis
- Babesiosis
- Rocky Mountain Spotted Fever
- Viral Meningitis
- Bacterial Meningitis
- Leptospirosis

Laboratory Identification:
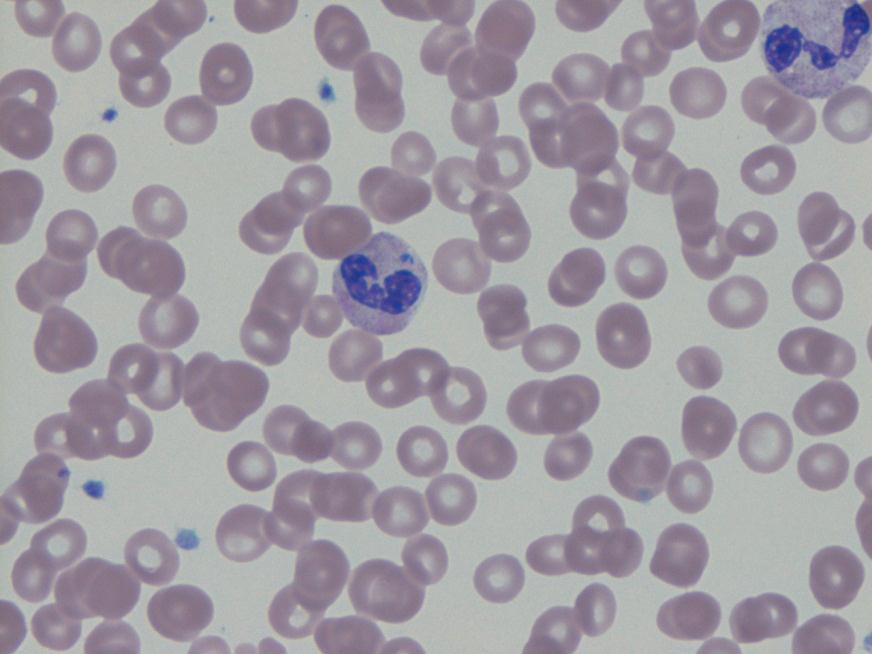
Anaplasma phagocytophilium was initially identified by PCR. Retrospectively, the blood smears originally examined for Babesia by both hematology and parasitology were reviewed. Both slides showed multiple granulocytes with intracytoplasmic morulae.
Discussion
Anaplasma phagocytophilium is the bacterium responsible for the tick-borne disease known as human granulocytic anaplasmosis. Anaplasma is transmitted to humans primarily through the bite of an infected Ixodes scapularis, the same species of tick which transmits Borrelia burgdorferi (Lyme disease) and Babesia spp. (human babesiosis). Anaplasmosis, Lyme disease, and babesiosis therefore share roughly the same geographical distribution in the United States with northeastern and upper midwestern states reporting the most cases.
Anaplasmosis most commonly presents about 1-2 weeks after a tick bite with the sudden onset of a variety of non-specific symptoms including fever, chills, headache, malaise, myalgia, nausea, and abdominal pain. Anaplasmosis, unlike other tick-borne diseases, rarely causes a rash. Routine blood tests may show thrombocytopenia, leukopenia, or elevated liver enzymes in some patients. Severe clinical presentations, more common in immunosuppressed patients, may include difficulty breathing, hemorrhage, renal failure or neurological problems. Anaplasmosis is estimated to be fatal in less than 1% of cases.
A routine blood smear is the quickest method for establishing an early presumptive diagnosis. Microscopic examination of the smear may reveal microcolonies of Anaplasma known as morulae within the cytoplasm of infected granulocytes. Ehrlichia, in contrast, will preferentially target and form morulae within monocytes. Because not all patients with anaplasmosis have visible morulae, this test is diagnostically insensitive and should be followed by further testing.
Confirmatory serologic testing for anaplasmosis includes an indirect immunofluorescence assay using an Anaplasma phagocytophilum antigen. For the highest sensitivity, this test should be performed on paired serum samples collected at least 2 weeks apart with the first sample taken as early in the disease as possible. A positive test will demonstrate a four-fold rise in antibody titers. Although it is a very sensitive detection method when run with paired samples, the lengthy testing time is less than ideal for patients requiring hospitalization for their disease.
A PCR assay on a sample of whole blood, although only available at a few reference laboratories, is the most efficient and accurate way to detect Anaplasma during the acute phase of the illness. The sample used for PCR testing should be taken before the initiation of antibiotic therapy as it causes the sensitivity of this test to rapidly decline.
Doxycycline is the first line treatment for adults and children of all ages with anaplasmosis as recommended by both the CDC and the AAP Committee on Infectious Diseases. Patients should be treated for at least 3 days after the fever subsides. Standard duration of treatment is 7 to 14 days. Therapy should be initiated immediately when there is a high clinical suspicion of anaplasmosis. A physician should never wait for the results of confirmatory testing to begin treatment. Most patients see improvement within 24-48 hours of treatment and non-response to doxycycline may indicate a different disease process.
Anaplasmosis, like many other tick-borne diseases, is a nationally reportable disease. All cases should be reported to local and state health departments as well as the CDC.
-Elaine Amoresano, MD, is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Microbiology Case Study: 29 Year Old in Preterm Labor at 30 Weeks Gestation
Case History:
A 29 year old woman presents to the hospital with contractions at 30 weeks gestation. This is her first pregnancy and it was previously uncomplicated. She did not experience loss of fluid or vaginal bleeding and did not have a history of recent illness or fever. A swab for group B Streptococcus (GBS) was collected and the patient was started on prophylactic penicillin. Clinical evaluation revealed evidence of acute infection with an elevated C-reactive protein and an increased white blood cell count with 97% neutrophils. Amniocentesis was performed and the amniotic fluid was sent to the laboratory for Gram Stain and culture.
Labor was allowed to progress and the infant was delivered vaginally. Cultures of cerebrospinal fluid and blood from the neonate were negative. The placenta was sent for histologic evaluation.


Laboratory Identification:
The laboratory workup revealed a gram negative bacillus with rounded ends that grew small grey to pale yellow colonies on blood and chocolate agars. The colonies had three regions; a raised central region, a refractile flat region, and an outer rougher spreading region. The colonies had a distinct bleach-like smell. There was no growth on MacConkey agar. The organisms were oxidase positive, catalase and indole negative. Mass spectrometry was utilized to identify the organism as Eikenella corrodens.
Discussion:
Eikenella corrodens is a component of normal mouth and upper respiratory tract flora. It is most notable for causing head and neck infections, periodontal disease, and as a significant player in “fight bite” infections. “Fight bite” results when a clenched fist hits another person’s mouth and the teeth cause lacerations to the hitter’s hand, which can subsequently lead to infection. Eikenella is implicated approximately 25% of the time in these types of infections. Only on very rare occasion is Eikenella known to cause gynecologic infections. Endometritis or cervicitis may infrequently be caused by colonization of an intrauterine contraceptive device (IUD) by Eikenella. And rarely, Eikenella is implicated as the isolated bacteria in cases of acute chorioamnionitis.
In the medical literature there are currently only 8 reported cases of chorioamnionitis caused by a pure Eikenella infection. As in our case, each of the women in the case reports had clinically silent infections and only presented with preterm labor. Most of the women were found to have elevated white blood cell counts in the absence of fever or alterations in other vital signs. In each case, the fetal membranes were intact. Two of the cases resulted in fatal infection of the neonates. Of note, three of the women were mentioned to be the recipients of oral intercourse throughout their pregnancies.
One of the reported cases involved a woman whose partner had a tongue piercing and it was noted that they engaged in daily oral sex during the pregnancy. The authors speculated that the tongue piercing played a role in the development of chorioamnionitis by either ascending vaginal infection or hematogenous spread caused by trauma from the tongue ring.
It is not known if a similar history was present in this case. The patient was treated with ampicillin and gentamycin and discharged following delivery. She is currently doing well. The infant has had no signs of infection, but at the time of this writing he is being treated in the neonatal intensive care unit for sequelae of prematurity.
References:
Garnier F, Masson G, Bedu A, et al. Maternofetal infections due to Eikenella corrodens. J Med Microbiol 2009; 58, 273-275.
Jadhav A, Belfort M, Dildy G. Eikenella corrodens chorioamnionitis: modes of infection? Am J Obstet Gynecol 2009; 200, e4-5.
-Britni Bryant, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Microbiology Case Study: A Two-Week-Old Infant with Fever and Fussiness
A two week old infant presents to the ED with fever and fussiness. She was born at 37 weeks gestation after an uncomplicated vaginal birth. Her mother reports she was in good health during her pregnancy and there are no family sick contacts since the infant was brought home from the hospital. In the ED, the infant was febrile and had a bulging fontanel. Blood and CSF were sent to the microbiology laboratory for culture. The following organism was isolated from blood and CSF specimens.

The organism isolated was Listeria monocytogenes.
L. monocytogenes is a short, Gram-positive bacilli on Gram stain (Image 1). In the microbiology laboratory, L. monocytogenes grows on 5% sheep blood, chocolate, and colistin naladixic acid (CNA) agars. The bacteria form small colonies of 1-2 mm after 24 hours of incubation at 35-37⁰C. On sheep blood agar these colonies have a narrow zone of b-hemolysis, which is very subtle. To highlight the hemolysis, the blood agar plate must be held up to a light source (Image 2) or colonies can be removed to reveal hemolysis of the agar directly below the growing bacterial colony. L. monocytogenes is catalase, Voges-Proskauer, and methyl red positive but oxidase and urea negative. It is also CAMP test positive using a S. aureus streak and has tumbling leaf motility. L. monocytogenes is routinely identified in our laboratory by MALDI-TOF MS. In addition, many rapid diagnostic panels such as the Nanosphere Verigene Gram-positive Blood Culture Assay (Northbrook, IL, USA) and Biofire FilmArray Blood Culture Identification Panel (Salt Lake City, UT, USA) include a target for rapid identification of Listeria spp./L. monocytogenes from positive blood culture.
L. monocytogenes can grow at a wide range of temperatures between 0-50⁰C. Its ability to grow at 4⁰C allows the organism to persist and replicate under refrigerated conditions on food products such as meat, vegetables, raw milk, and cheeses. For the same reason, L. monocytogenes is also a concern for contamination of refrigerated blood products.
It is estimated that 1-5% of healthy adults are asymptomatically colonized with L. monocytogenes. The organism is most often contracted by consuming contaminated foods, which causes a mild gastrointestinal illness in otherwise healthy hosts. L. monocytogenes infection in pregnant women can present as a mild, self-limited, influenza-like illness Infection and 1/3 of women report no symptoms at all. The bacteria from infected mothers are able to cross the placenta, resulting in transmission to the fetus in utero or infants can be infected during the birthing process.
L. monocytogenes infections that occur within the first 7 days of life are characterized as early-onset. Patients often present with symptoms of preterm birth, pneumonia, and sepsis. Patients may also have an erythematous rash with small papules histologically described as “granulomatosis infantisepticum.” Late-onset infection occurs between 8-30 days of life with patients most often presenting with sepsis and meningitis. Both neonatal presentations are reported to have a high mortality rate—14-56% for early-onset and 25% for late-onset infection. Luckily, invasive neonatal L. monocytogenes infections have been declining over the past decades and are now a rare occurrence in newborns. These days, invasive listeriosis is more common in immunocompromised patients with defects in cell-mediated immunity. In 2013, the last year for which there is data, the CDC reported 633 cases of invasive listeriosis, but only 68 (11%) were pregnancy-associated. These infants had a 76% survival rate. More information about Listeria epidemiology in pregnant and non-pregnant populations can be found at the CDC website http://www.cdc.gov/listeria/pdf/listeria-annual-summary-2013-508c.pdf.
L. monocytogenes is intrinsically resistant to cephalosporins. Ampicillin is considered the “gold standard” for treatment. The addition of an aminoglycoside for synergy is often used in practice, but a retrospective cohort study showed it had no effect on reducing infant mortality. Trimethoprim-sulfamethoxazole, quinolones, or vancomycin can be used to treat penicillin allergic patients. Newer Gram-positive antibiotics including linezolid, daptomycin, and tigecycline have also shown clinical efficacy against L. monocytogenes infections.
References:
Manual of Clinical Microbiology, 11th edition
Pediatric Red Book, 2015 Report of the Committee on Infectious Diseases, 30th edition
Centers for Disease Control and Prevention listeriosis website http://www.cdc.gov/listeria/
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
