A two week old infant presents to the ED with fever and fussiness. She was born at 37 weeks gestation after an uncomplicated vaginal birth. Her mother reports she was in good health during her pregnancy and there are no family sick contacts since the infant was brought home from the hospital. In the ED, the infant was febrile and had a bulging fontanel. Blood and CSF were sent to the microbiology laboratory for culture. The following organism was isolated from blood and CSF specimens.

The organism isolated was Listeria monocytogenes.
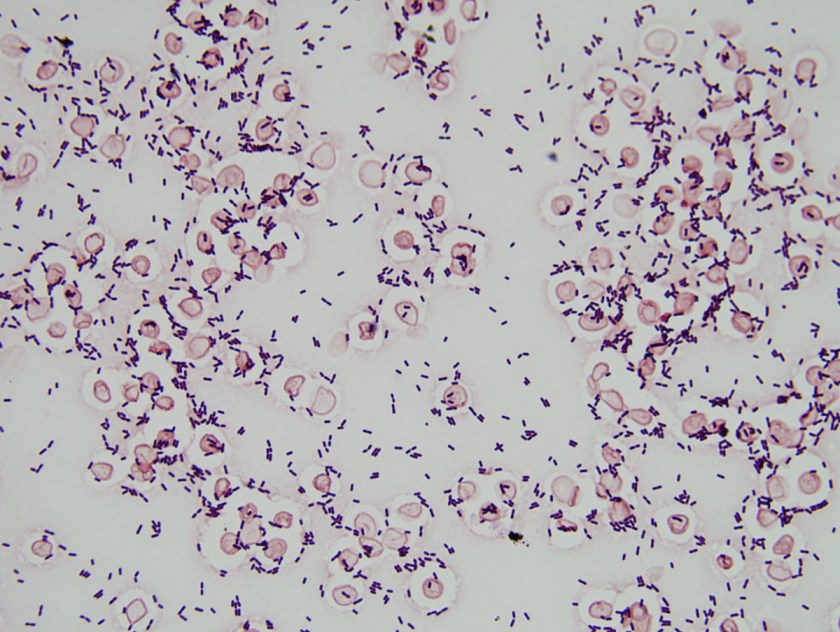
L. monocytogenes is a short, Gram-positive bacilli on Gram stain (Image 1). In the microbiology laboratory, L. monocytogenes grows on 5% sheep blood, chocolate, and colistin naladixic acid (CNA) agars. The bacteria form small colonies of 1-2 mm after 24 hours of incubation at 35-37⁰C. On sheep blood agar these colonies have a narrow zone of b-hemolysis, which is very subtle. To highlight the hemolysis, the blood agar plate must be held up to a light source (Image 2) or colonies can be removed to reveal hemolysis of the agar directly below the growing bacterial colony. L. monocytogenes is catalase, Voges-Proskauer, and methyl red positive but oxidase and urea negative. It is also CAMP test positive using a S. aureus streak and has tumbling leaf motility. L. monocytogenes is routinely identified in our laboratory by MALDI-TOF MS. In addition, many rapid diagnostic panels such as the Nanosphere Verigene Gram-positive Blood Culture Assay (Northbrook, IL, USA) and Biofire FilmArray Blood Culture Identification Panel (Salt Lake City, UT, USA) include a target for rapid identification of Listeria spp./L. monocytogenes from positive blood culture.
L. monocytogenes can grow at a wide range of temperatures between 0-50⁰C. Its ability to grow at 4⁰C allows the organism to persist and replicate under refrigerated conditions on food products such as meat, vegetables, raw milk, and cheeses. For the same reason, L. monocytogenes is also a concern for contamination of refrigerated blood products.
It is estimated that 1-5% of healthy adults are asymptomatically colonized with L. monocytogenes. The organism is most often contracted by consuming contaminated foods, which causes a mild gastrointestinal illness in otherwise healthy hosts. L. monocytogenes infection in pregnant women can present as a mild, self-limited, influenza-like illness Infection and 1/3 of women report no symptoms at all. The bacteria from infected mothers are able to cross the placenta, resulting in transmission to the fetus in utero or infants can be infected during the birthing process.
L. monocytogenes infections that occur within the first 7 days of life are characterized as early-onset. Patients often present with symptoms of preterm birth, pneumonia, and sepsis. Patients may also have an erythematous rash with small papules histologically described as “granulomatosis infantisepticum.” Late-onset infection occurs between 8-30 days of life with patients most often presenting with sepsis and meningitis. Both neonatal presentations are reported to have a high mortality rate—14-56% for early-onset and 25% for late-onset infection. Luckily, invasive neonatal L. monocytogenes infections have been declining over the past decades and are now a rare occurrence in newborns. These days, invasive listeriosis is more common in immunocompromised patients with defects in cell-mediated immunity. In 2013, the last year for which there is data, the CDC reported 633 cases of invasive listeriosis, but only 68 (11%) were pregnancy-associated. These infants had a 76% survival rate. More information about Listeria epidemiology in pregnant and non-pregnant populations can be found at the CDC website http://www.cdc.gov/listeria/pdf/listeria-annual-summary-2013-508c.pdf.
L. monocytogenes is intrinsically resistant to cephalosporins. Ampicillin is considered the “gold standard” for treatment. The addition of an aminoglycoside for synergy is often used in practice, but a retrospective cohort study showed it had no effect on reducing infant mortality. Trimethoprim-sulfamethoxazole, quinolones, or vancomycin can be used to treat penicillin allergic patients. Newer Gram-positive antibiotics including linezolid, daptomycin, and tigecycline have also shown clinical efficacy against L. monocytogenes infections.
References:
Manual of Clinical Microbiology, 11th edition
Pediatric Red Book, 2015 Report of the Committee on Infectious Diseases, 30th edition
Centers for Disease Control and Prevention listeriosis website http://www.cdc.gov/listeria/

-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.

Was the mother placenta culured for recovery of organism.
It was not. The patient didn’t present until two weeks after birth and since both the pregnancy and birth were uncomplicated, the placenta was not sent for culture or histopathology.