A 68 year old female presented to our institution with complaints of lower right quadrant abdominal pain but an absence of nausea, vomiting, diarrhea and fever. The patient noted she thought she had a worm in her stool and submitted three stool samples for an ova and parasite exam. While the three stool samples were negative for worms and eggs, two of the three samples were positive for the organism seen below. The patient was treated with a regimen of metronidazole for ten days, and a repeat ova and parasite exam after treatment was negative for the parasite. The patient presented again three months later with similar complaints of abdominal pain, resulting in another ova and parasite exam which was again positive for the same organism.
Figure 1. Blastocystis spp. organism found in the most recent ova and parasite exam.Figure 2. Another Blastocystis spp. organism found in the most recent ova and parasite exam (circled in red). The organism is in the vacuole form, with three nuclei visible on the periphery.
Originally discovered in 1911, Blastocystis species are anaerobic protozoan parasites commonly found in the human gastrointestinal tract.2 In addition to being found in humans, Blastocystis spp. has also been found in a variety of animals, with at least nine different genotypes described in literature.4 While historically these organism have been referred to as Blastocystis hominis when found in humans, genotyping and molecular studies have revealed immense genetic diversity in organisms isolated from humans, resulting in a more general designation of Blastocystis spp.1 These organisms have been observed worldwide, stemming from contaminated food, water and soil and transmitted in a fecal-oral route.2 Recently, there has been much debate as to whether the parasite is truly pathogenic or commensal due to the presentation of both symptomatic and asymptomatic patients found carrying this parasite.4
Despite debate on the pathogenicity of Blastocystis spp., potential signs and symptoms from symptomatic patients have been documented. Such symptoms could include watery diarrhea, nausea, abdominal pain, bloating, excessive gas, loss of appetite, weight loss, and fatigue, among other symptoms.3 Diagnosis heavily relies on stool specimens using light microscopy to examine direct smears, with the vacuolar form of the parasite most commonly observed.1 In addition to the vacuolar form, granular, amoeboid and cyst forms have also been described in literature.4 The parasite itself lacks a cell wall, but contains mitochondria, Golgi apparatuses, and both smooth and rough ER.2 The vacuolar form, observed in Figure 1 and Figure 2, contains a large (5-40 mm) central vacuole-like body which compresses the nuclei to periphery of the cell.2
Treatment is typically not needed if the patient remains asymptomatic.3 However, for individuals who present with symptomatic infection, a regimen of metronidazole or tinidazole is recommended.3 It is important to note that due to the controversial nature of Blastocystis spp. as a pathogenic parasite, additional pathogens or causes of disease should first be ruled out prior to treatment.2
4 Wawrzyniak, I., Poirier, P., Viscogliosi, E., Dionigia, M., Texier, C., Delbac, F., & Alaoui, H. E. (2013). Blastocystis, an unrecognized parasite: an overview of pathogenesis and diagnosis. Therapeutic advances in infectious disease, 1(5), 167–178. https://doi.org/10.1177/2049936113504754
-Maggie King is a Masters Student in the Department of Pathology and Laboratory Medicine at The University of Vermont Larner College of Medicine.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
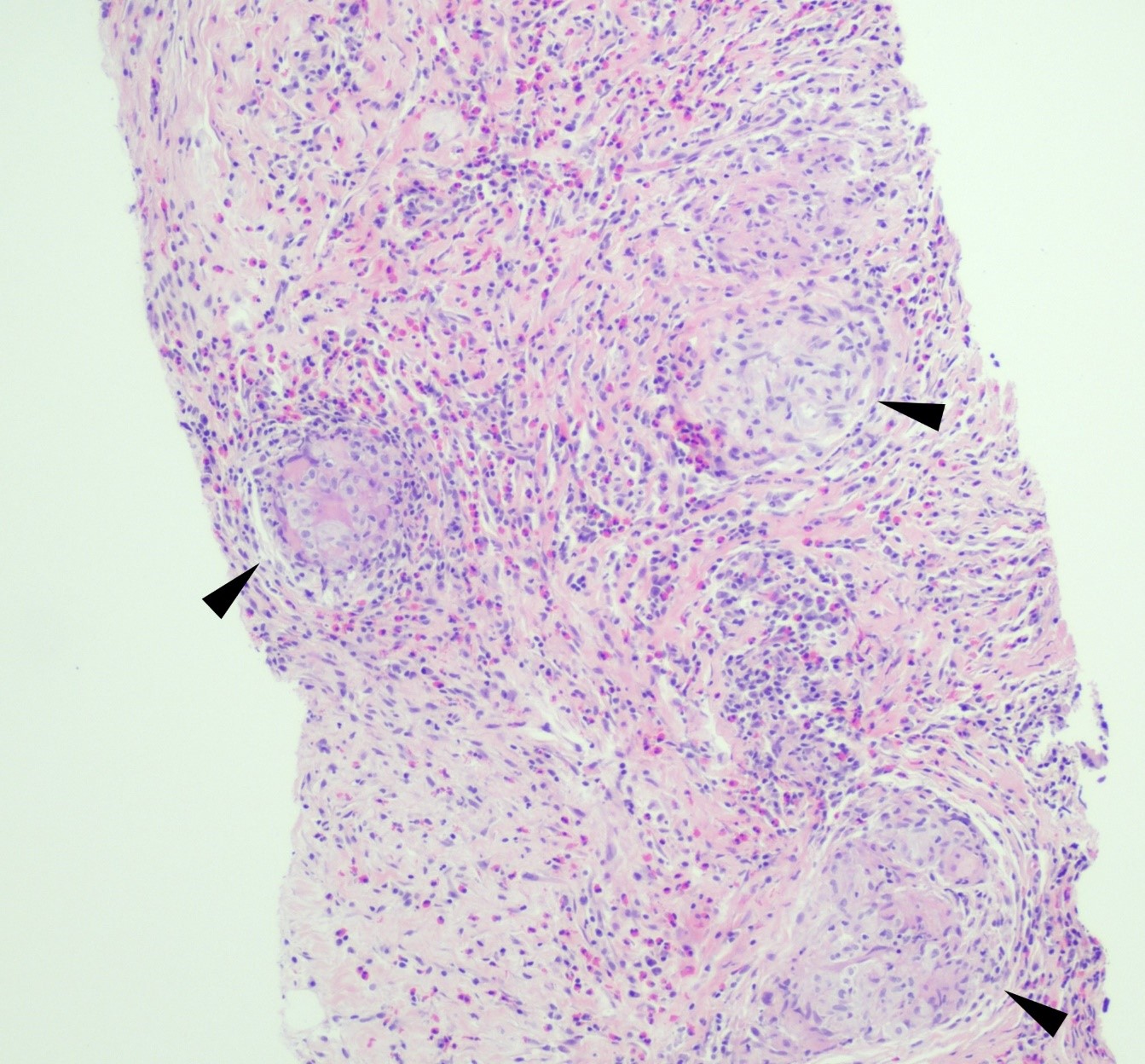
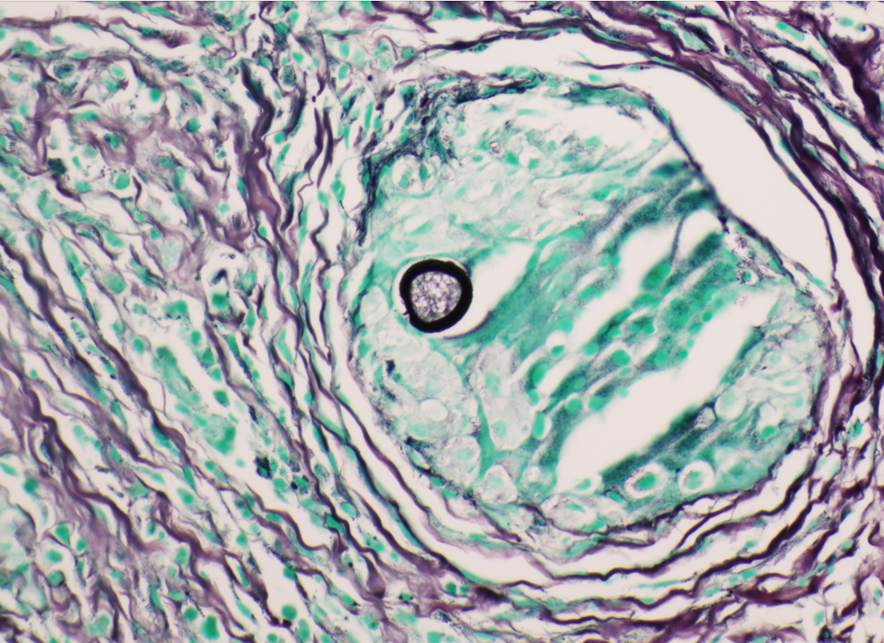
A 59 year old female presented with a one-month history of generalized abdominal pain, difficulty breathing, and early satiety. She was previously seen at an external facility and found to have liver hypointensity and abdominal distension which were concerning for liver cancer. Social history included travel to Sacramento and California deserts for hiking in the last few months. CT of the abdomen and pelvis demonstrated extensive peritoneal carcinomatosis with no primary etiology and a right hepatic lobe focus. MRI revealed diffuse omental caking and peritoneal thickening consistent with peritoneal carcinomatosis. Hepatic lesions also seen on MRI were consistent with hemangiomas. Laboratory evaluation was positive for Hepatitis B virus infection along with elevated liver enzymes (AST and ALT), CA-125, and normal levels of CEA. Paracentesis was performed removing 3 liters of yellow, cloudy fluid. Cytology demonstrated benign mesothelial cells, macrophages, and mixed inflammatory cells with a lymphocytic predominance in the peritoneal fluid. No malignant cells were identified. Initial aerobic, anaerobic, mycobacterial, and fungal cultures were negative. Serum Cryptococcus neoformans antigen testing was also negative. Ultrasound-guided core biopsy of the omental mass was performed; however, tissue was not sent for culture. Histopathology revealed granulomatous inflammation with eosinophilic infiltrate (Figure 1). A singular spherule was highlighted by GMS stain (Figure 2). Fungal serology via complement fixation for Coccidioides was positive (titer: 1:8) while Blastomyces, Histoplasma, and Aspergillus serologies were negative. The patient was subsequently managed on fluconazole.
Figure 1. Core biopsy of omental tissue revealing granulomatous inflammation and diffuse eosinophilic infiltrate in a background of chronic inflammation, lymphocytes and fibrosis. Arrows indicate granuloma formation (H&E, 100x).Figure 2.Core biopsy of omental tissue revealing a spherule with its thick wall containing endospores in a granuloma (GMS, 400x).
Discussion
Coccidioidomycosis is caused by the thermally dimorphic fungus Coccidioides that is endemic to the Southwestern United States, Mexico, and some regions in Central and South America. In endemic regions, farm workers, construction workers, military personnel, archaeologists, excavators, inmates, and correctional facility officers are most affected.1 Individuals with significant exposure to the outdoors in endemic regions may be disproportionately affected. Multiple species of Coccidioides can cause disease and geographic distribution is changing2; however, the clinical presentation and approach to treatment of coccidioidomycosis are the same.
The pathophysiology of Coccidioides infection requires inhalation of arthroconidia which may result in pulmonary disease. Once inhaled, the organism forms an endospore-filled spherule in host tissue. Mature spherules rupture and disseminate endospores into surrounding tissue, which can then undergo additional replication cycles within the host. Symptomatic pulmonary disease appears to be related to fungal burden and usually presents with fever, fatigue, cough, pleurisy, and dyspnea, or less commonly peripheral eosinophilia and high erythrocyte sedimentation rate.3 Extrapulmonary disease, also known as disseminated coccidioidomycosis, is observed in <1% of cases. Extrapulmonary spread may develop in the meninges, skin, bone, or joints via hematogenous or lymphatic spread. Rarer sites of disease include the peritoneum, glandular tissue, visceral organs, bone marrow, reproductive organs, the pericardium, kidney, and the bladder.3,4
The gold standard for diagnosis of coccidioidomycosis is culture; however, histopathology may yield definitive diagnosis, especially in cases where culture was not obtained. Following histopathological examination, polymerase chain reaction (PCR) from a variety of sources may also confirm the diagnosis, especially in cases without supporting clinical or laboratory data to suggest coccidioidomycosis.5 When culture is performed, Coccidioides is recovered in its environmental, or mold form. This phase is highly infectious and can pose a significant biosafety hazard; therefore, laboratory personnel should be appropriately notified when Coccidioides is suspected, especially since Coccidioides sp. can grow on solid media within the timeframe of conventional bacterial cultures.3 Serology can be used as an adjuvant test methodology in suspected cases. Serology may be performed on blood samples, CSF, joint, or pleural fluid and measured by immunodiffusion (ID), enzyme-linked immunoassay (EIA), or complement fixation (CF). ID uses gelatin as the medium in which antibodies are placed in one well and Coccidioides antigens are placed in another. Where the two meet through diffusion, a band will form from precipitated immune complexes. ID tests for both IgG and IgM antibodies.6 EIA, in contrast, uses enzyme-labeled antibodies to detect patientantibody complexed with bound antigen. CF incubates Coccidioides antigens with patient serum that has been heated (to inactivate endogenous complement). Following incubation, fresh, non-human serum containing complement is added. If immune complexes have formed between patient antibodies and the antigens, then the fresh serum complement will affix to those complexes and indicator red blood cells will remain intact when added. A positive result will have a suspension of intact red blood cells that can be titered. A negative test will result in lysed red blood cells. CF tests for IgG antibodies.6Coccidioides antigen assays may be used to test the urine, blood, and CSF of patients with extrapulmonary disease. In immunocompromised hosts, serology may be negative, and coccidioidal antigen assay may be performed. Clinical management commonly involves long-term antifungal therapy with or without surgical intervention for high-risk individuals.4
Mazi PB, Sahrmann JM, Olsen MA, Coler-Reilly A, Rauseo AM, Pullen M, Zuniga-Moya JC, Powderly WG, Spec A. The Geographic Distribution of Dimorphic Mycoses in the United States for the Modern Era. Clin Infect Dis. 2023 Apr 3;76(7):1295-1301. doi: 10.1093/cid/ciac882. PMID: 36366776; PMCID: PMC10319749.
Proia L. Chapter 28: The Dimorphic Mycoses. In: Spec A, Escota G, Chrisler C, Davies B., eds. Comprehensive Review of Infectious Diseases. > ed. Elsevier; 2020: 411-423.
Johnson RH, Sharma R, Kuran R, Fong I, Heidari A. Coccidioidomycosis: a review. J Investig Med. 2021;69(2):316-323. doi:10.1136/jim-2020-001655.
Binnicker MJ, Buckwalter SP, Eisberner JJ, Stewart RA, McCullough AE, Wohlfiel SL, Wengenack NL. Detection of Coccidioides species in clinical specimens by real-time PCR. J Clin Microbiol. 2007 Jan;45(1):173-8. doi: 10.1128/JCM.01776-06.
-Evelyn Ilori, MD, PhD is a third-year AP/CP resident at University of Texas Southwestern Medical Center in Dallas, Texas.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
Often in casual conversation (and even in medical records) all open skin wounds are called “lacerations,” despite the fact that this term has a fairly narrow definition. Forensic pathologists need to be very particular about using correct terminology for injuries. Different types of injuries correspond to different mechanisms of injury, which can have real consequences for an ongoing investigation. Excluding gunshot wounds, (a separate wound type that requires its own blog post), the other main categories of trauma are blunt and sharp force injuries. Blunt injuries are inflicted by dull objects, whereas sharp force injuries are inflicted by a blade or other edged object. Chop wounds, less commonly encountered in practice, have features of both.
Blunt Force Injuries
There are three cutaneous manifestations of blunt impacts. An abrasion is the equivalent of a scrape, wherein the superficial skin layer is removed. A contusion refers to a bruise, in which there is hemorrhage in the skin and subcutaneous tissue. Finally, lacerations occur when the skin and underlying tissues are crushed and tear apart from each other, resulting in an open wound. Neurovascular bundles in the subcutaneous tissue have high resistance to crushing forces and remain intact, resulting in characteristic “tissue bridging” within the wound depths. The edges of lacerations are often abraded, as well. Because blunt force injuries result from direct application of force, the object involved can impart a pattern onto the skin, or deposit potential trace evidence (hair, fibers, paint chips). It’s always important to look for patterns and try to correlate injuries with scene findings. If a patterned (or suspected patterned) injury is found at autopsy, scale photographs must be taken with a specific ruler (the ABFO ruler), to produce scale photographs for comparison if the object is found.
Deaths related to blunt force injuries can be accidental, suicidal, or homicidal in nature, and cover a wide variety of situations. Motor vehicle accidents, falls or jumps from heights, and homicidal beatings are all situations where the cause of death is blunt force injuries. Each of these situations have particular wound patterns that forensic pathologists are trained to recognize.
Sharp Force Injuries
Sharp injuries can be divided into stab wounds or incised/cutting wounds. The difference is wound dimensions: stab wounds are deeper than they are long, and incised wounds are longer than they are deep. In contrast to lacerations, sharp forces cleanly transect all tissues including neurovascular bundles, meaning stab and incised wounds show no tissue bridging. As mentioned in the first paragraph, distinguishing a laceration from a cut made with a blade can be critical. Mis-identifying a laceration as a “cut” or “stab,” or vice versa, may send law enforcement down the wrong path. Similar to blunt force, deaths by sharp force can be accidental, suicidal, or homicidal, although in my experience accidental deaths by sharp force are extremely rare.
These categories make the definitions sound clear-cut (no pun intended), but it’s important to keep in mind that in actual practice, as with everything else in medicine, unusual situations occur. ‘Chop’ wounds have features of both sharp and blunt force and are typically inflicted by a heavy object with an edge (like an axe or propeller blade). As one example, a beating with a hatchet or machete may cause sharp, blunt, or chop wounds, depending on the sharpness of the blade and what part of the weapon impacts the body. Even when an unusual object is used as a weapon, recognizing the different components of a wound and any patterns imparted on the skin can help guide an investigation.
This decedent was an ejected passenger in a motor vehicle accident. The large abrasions over the arm involve one surface of the extremity and have a faint internal pattern of parallel lines, consistent with “brush burns” or “road rash.”This patterned contusion on the back of a pedestrian run over by a truck matches the tire tread pattern of the vehicle.This is a classic example of a laceration. Note the bands of intact tissue which span the width of the wound (the “tissue bridging”) which are characteristic of lacerations.A typical stab wound. Note the cleanly transected wound edges, and the absence of tissue bridging. The squared-off margin on the right, in contrast to the left side of the wound, suggests this was a single-edged blade.
-Alison Krywanczyk, MD, FASCP, is currently a Deputy Medical Examiner at the Cuyahoga County Medical Examiner’s Office.
Jamie, the manager of a large metropolitan hospital lab, has many responsibilities. She must spend most of her time in the office, on the phone, or in meetings. She does find time to come out to speak with the employees, but only for a second to check on things or maybe make a request. During a recent safety audit, Jamie received feedback that several employees were seen working in the lab without using the proper PPE. One tech was working the bench without gloves, one individual had their lab coat on but not buttoned, and one auditor noticed that no one in the lab was wearing face or eye protection. This came as a shock to Jamie, she had never noticed this before. This doesn’t necessarily mean that Jamie is a bad manager, it could be that she was so focused on daily operation issues and she failed to notice other problems.
We have all heard the term “nose blind.” It’s when a person is around a bad smell so frequently that they become oblivious to its presence, and this can actually happen with vision as well. Have you ever heard the phrase, “you can’t see the forest for the trees,” or maybe the term “snow blind?” This phenomenon occurs when someone is concentrating so hard on one problem they may miss a more serious safety issue directly in front of them. Lucky for us, we have a tool to help those safety issues stand out. We have our “Safety Eyes!”
Ok, so what exactly are Safety Eyes? Are they some kind of new eye protection device that fit directly on your eyes? Are they indestructible eyes? Not exactly. Safety Eyes is a term used to describe the ability to spot current or potential safety issues more easily. It is the ability to walk into a room and immediately scan the environment for safety issues. This ability doesn’t just magically develop, it takes time and effort to master, and once you have it, you will begin to notice issues without even trying.
There are methods you can use to develop your safety eyes. Like any other sense, it is important to practice using it frequently so that its use becomes second nature to you. Think about this in terms of a wine sommelier. A sommelier may train for several years to acclimate their nose and palate in order to detect various nuances in different types of wine. It is through experience and exposure to many different types of wine that they are able to pick up on the slightest hint of a flavor or scent. This same repeated exposure works for sharpening your Safety Eyes as well. It is probably unlikely that you have a Safety Unicorn in your lab who can pick up on potential safety issues on their first day on the job. To become better at seeing safety issues, perform periodic rounding in the department and look for specific safety issues. Start by covering one specific safety area such as PPE use, waste management or fire safety. Your ability to quickly notice issues in these areas will sharpen, and you will be able to expand your newly honed power to other areas.
By developing your Safety Eyes, you will become more aware of various types of safety issues and where they are most likely to be encountered. It is easy to become “nose blind” to safety issues in a lab where you work every day. Start by simply using a checklist to focus specifically on one new safety area and soon the issues that may have been there all along will be more easily detected. Now that you can see the forest, you can make those important changes which will improve your overall lab safety culture!
-Jason P. Nagy, PhD, MLS(ASCP)CM is a Lab Safety Coordinator for Sentara Healthcare, a hospital system with laboratories throughout Virginia and North Carolina. He is an experienced Technical Specialist with a background in biotechnology, molecular biology, clinical labs, and most recently, a focus in laboratory safety.
A 34 year old male presented to the emergency department (ED) with acute onset abdominal pain, nausea, vomiting, persistent fever, and chills. His physical examination at that time was consistent with appendicitis. Patient was treated with Zosyn for broad coverage. Imaging showed a normal appendix. Three days later after blood was drawn, his blood cultures flagged positive for gram negative, elongated, thin rods. Growth was determined to be Fusobacterium mortiferum by MALDI-TOF. Ampicillin/sulbactam was started and patient was given Amoxicillin/clavulanic acid for outpatient treatment. Further follow-up of the patient showed normal white blood count and normal urinalysis. Repeat blood cultures were negative.
Images of Gram stain demonstrating long, slender, gram negative rods (top) and bacterial growth on anaerobic plate (bottom) from positive blood culture bottle.
Discussion
Fusobacteria are anaerobic, gram negative, spindle-shaped rods with pointed ends. They are part of the upper respiratory and gastrointestinal flora in humans but can cause diseases ranging from tonsillitis to septic shock.1Fusobacterium nucleatum and necrophorum are commonly isolated in human diseases, although other species such as Fusobacterium mortiferum, as described in our case, have occasionally been documented as a secondary cause of septicemia 2 or bacteremia 1 and in rare instances implicated in the development of thyroid abscess.3
F. nucleatum is a member of oropharyngeal flora and unsurprisingly involved in gingival and periodontal diseases.4 It has been also described as the most likely cause of extra-oral infections among oral anaerobes.5F. nucleatum has been detected in various fetal and placental tissues associated with adverse pregnancy outcomes, such as preeclampsia, chorioamnionitis and preterm rupture of membranes.6 Recent studies have reported this species to be abundant in colon, esophageal carcinoma, pancreatic and breast cancers. It is associated with poor prognosis in colon, rectal, pancreatic and esophageal cancers by promoting pro-tumorigenic immune microenvironment and reduction in the number of tumor-infiltrating lymphocytes.7, 10 One of the proposed theories is the involvement of the Fap2 virulence factor that has been described to inhibit tumor cell clearance in colorectal cancer cells.8 The other commonly isolated species is F. necrophorum, which is associated with oropharyngeal infection followed by septic thrombophlebitis of the internal jugular vein with sepsis and metastatic diseases typically involving the lungs. This syndrome is known as Lemiere’s disease first described in 1936 by Andre Lemierre. F. necrophorum usually causes infection in young, otherwise healthy adults in contrast to F. nucleatum1 which is associated more with the elderly population. According to Afra et al most of the mortality cases were due to F. nucleatum as opposed to F. necrophrum. This could be attributed to co-morbidities in elderly patients with positive F. nucleatum cultures.
Fusobacterium species can be identified using mass spectrometry MALDI-TOF. Typically, Fusobacterium species are resistant to vancomycin, but susceptible to colistin and kanamycin disk identification tests; however, F. nucleatum is susceptible to all three drugs. F. mortiferum and F. varium grow in the presence of bile. F. necrophorum shows positive indole and negative nitrate testing. Sequencing of the 16S RNA gene and 16S-23S rRNA gene spacer region can be used to determine the different species3,9
Fusobacterium species are usually susceptible to penicillin, clindamycin, metronidazole, and chloramphenicol and resistant to macrolides. F. nucleatum and F. necrophorum may produce beta-lactamases.3 In rare cases, surgical intervention is warranted for abscess formation.
References
Afra K, Laupland K, Leal J, Lloyd T, Gregson D. Incidence, risk factors, and outcomes of fusobacterium species bacteremia. BMC Infect Dis. 2013;13(1). doi: 10.1186/1471-2334-13-264.
Stavreas NP, Amanatidou CD, Hatzimanolis EG, et al. Thyroid abscess due to a mixed anaerobic infection with fusobacterium mortiferum. J Clin Microbiol. 2005;43(12):6202. doi: 10.1128/jcm.43.12.6202-6204.2005.
Moore WE, Moore LV. The bacteria of periodontal diseases. Periodontol 2000. 1994 Jun;5:66-77. doi: 10.1111/j.1600-0757.1994.tb00019.x. PMID: 9673163.
Bolstad AI, Jensen HB, Bakken V. Taxonomy, biology, and periodontal aspects of Fusobacterium nucleatum. Clin Microbiol Rev. 1996 Jan;9(1):55-71. doi: 10.1128/CMR.9.1.55. PMID: 8665477; PMCID: PMC172882.
Han YW. Fusobacterium nucleatum: A commensal-turned pathogen. Current Opinion in Microbiology. 2015;23:141. doi: 10.1016/j.mib.2014.11.013.
Alon‐maimon T, Mandelboim OO, Bachrach G. Fusobacterium nucleatum and cancer. Periodontology 2000. 2000;89(1):166. doi: 10.1111/prd.12426.
Umaña A, Sanders BE, Yoo CC, Casasanta MA, Udayasuryan B, Verbridge SS, Slade DJ. Utilizing Whole Fusobacterium Genomes To Identify, Correct, and Characterize Potential Virulence Protein Families. J Bacteriol. 2019 Nov 5;201(23):e00273-19. doi: 10.1128/JB.00273-19. PMID: 31501282; PMCID: PMC6832068.
Garcia-Carretero R, Lopez-Lomba M, Carrasco-Fernandez B, Duran-Valle MT. Clinical features and outcomes of fusobacterium species infections in a ten-year follow-up. The Journal of Critical Care Medicine. 2017;3(4):141. doi: 10.1515/jccm-2017-0029.
Brennan CA, Garrett WS. Fusobacterium nucleatum — symbiont, opportunist and oncobacterium. Nat Rev Microbiol. 2018;17(3):156. doi: 10.1038/s41579-018-0129-6.
-Dr. Hayk Simonyan was born and raised in Yerevan, Armenia. He attended Yerevan State Medical University after Mkhitar Heratsi where he received his doctorate degree. He did his research at The George Washington University. His studies were focused on transcription factor activation in the SFO-PVN axis that leads to cardio-metabolic changes mediated by obesity, oxidative stress, and angiotensin-II. One of his other projects included collaboration with the National Cancer Institute, working on alternative treatment for glioblastoma multiforme. His academic interests include surgical pathology and molecular. In his spare time, Hayk enjoys spending time with family, playing soccer, tennis, and skiing. Hayk is pursuing AP/CP training.
-Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.
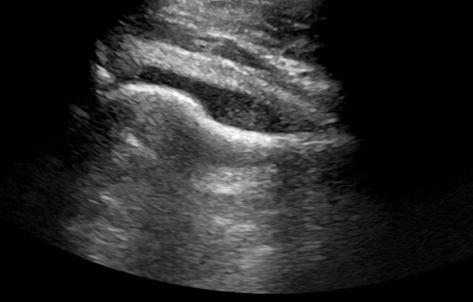
A young man presented to the emergency department with the primary complaint of severe right hip pain persisting for 2 days. This pain began after standing uncomfortably for hours at an event. His right hip was tender to palpation with some erythema and swelling. He had no recent fall or known injury. He denied recent fever, chills, aches, constipation, diarrhea, changes in urinary habits, chest pain, and shortness of breath. An ultrasound (US) of the right hip joint showed moderate amount of effusion (Image 1). Laboratory results also showed an elevated white blood cell count (WBC).
Image 1. US of the right hip joint showing moderate effusion.
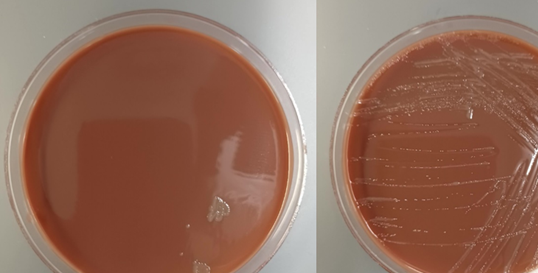
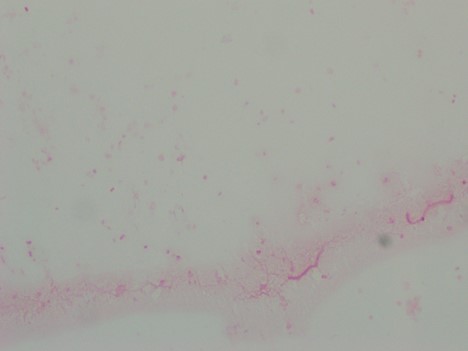
The patient underwent incision and drainage of his right hip to relieve the swelling, and samples were collected for Gram stain and aerobic and anaerobic bacterial culture. Blood was also collected from two separate sites for culture. The blood cultures showed no growth following 5 days of incubation. Gram stain of the effusion showed 4+ WBC with no organisms seen (Image 2). The joint fluid was set up for aerobic and anaerobic bacterial culture. Anaerobic bacterial culture showed no organism growth. However, a few small, grey-ish mucoid colonies grew in the first quadrant on Chocolate agar in the aerobic culture (Image 3). Gram stain was performed on one of the colonies (Image 4). MALDI-TOF confirmed the identification of Neisseria gonorrhoeae.
Image 2. Gram stain of effusion obtained from the right hip joint showing increased WBCs. Image 3: Left) Bacterial growth on the Chocolate agar plate. Right) Bacterial growth subcultured on another Chocolate agar plate.Image 4: Gram stain of one of the colonies that grew on the Chocolate agar. The Gram stain showed organisms shaped like coffee-beans.
Discussion
Neisseria gonorrhoeae is a fastidious, gram negative diplococci bacteria that can grow inside neutrophils after surviving phagocytosis. It is oxidase positive and aerobic, and generally transmitted through sexual contact such as vaginal, anal, or oral sex.1,2 After a gonococcal infection has resolved, the patient does not develop immunity to future infections from the bacteria. Reinfection is possible due to its ability to evade the immune system by varying its surface proteins, therefore making it appear novel to the immune system.3 Signs of septic arthritis include chills and fever, pain at the joint, inability to move infected joint, erythema, and swelling.4
Multiple factors increase the risk of septic arthritis, including a systemic blood-borne infection, IV drug use, osteoarthritis, past history of septic arthritis, rheumatoid arthritis, alcoholism, diabetes, HIV, lung or liver disorders, old age, and a suppressed immune system.4 Other forms of gonococcal infection are genitourinary infections, which are the most common, disseminated gonococcemia, and gonococcal ophthalmia neonatorum. Genitourinary infections can be particularly dangerous in women if left untreated, as this can lead to pelvic inflammatory disease that could result in infertility due to scarring of the fallopian tubes.5,6 Gonococcal infections of the eyes are one of the leading cause of blindness in neonates in the United States, but can be successfully prevented through treating the mother with antibiotics before birth and administration of eye drops to the baby at birth.7
Identification of N. gonorrhoeae can be done using Gram stain, aerobic bacterial culture on Chocolate or Modified Thayer-Martin (MTM) agar, or nucleic acid amplification test (NAAT). Testing can be done from a urethral swab, urine sample, or sample of body fluid from the area of suspected infection.8,9 Culture is slow with low recovery rates. In urogenital cases, where there is ample colonization of normal flora, genital flora may outgrow N. gonorrhoeae, reducing its recovery. MTM media is useful because it is a GC agar base that makes it selective for N. gonorrhoeae growth. It contains vancomycin, colistin, nystatin, and trimethoprim lactate, which suppresses growth of most other gramgnegative diplococci, gram negative bacilli, gram positive organisms, and yeast.10 The most common testing methodology for urogenital gonococcal infection is NAAT. Some FDA approved platforms also accept rectal or throat samples, however most only accept those from urogenital sources.11 Also, while NAAT is a quick and sensitive diagnostic test, it has the downside of not being able to distinguish between DNA obtained from living or dead bacteria.12
Intravenous (IV) or intramuscular (IM) ceftriaxone is the preferred treatment choice for N. gonorrhoeae infections. Alternatively, other third generation cephalosporins can be used as well, including cefotaxmine and ceftizoxime. Typically, patients with a beta-lactam allergy have been shown to tolerate ceftriaxone, and those who cannot should undergo desensitization due to its effectiveness against this infection. A single dose of azithromycin or a prescription of doxycycline taken twice daily for a week is usually added to the regimen to cover for a potential Chlamydia trachomatis co-infection. Patients presenting with purulent arthritis should also undergo drainage, either arthroscopically or through multiple joint aspirations.13,14
References:
Ryan, K. J., Ray, G., and Sherris, J. C. (2004). Sherris Medical Microbiology: An introduction to Infectious Diseases, 4th edition. McGraw-Hill Medical.
Levinson, W. (2014). Review of Medical Microbiology and Immunology, 13th edition. McGraw-Hill Medical.
Jennings, L. K. and Krywko. D. M. Pelvic Inflammatory Disease. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499959/.
Castro Ochoa, K. J. and Mendez, M. D. Ophthalmia Neonatorum. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551572/.
Ng, L.-K. and Martin, I. E. The Laboratory Diagnosis of Neisseria gonorrhoeae. Canadian Journal of Infectious Disease and Medical Microbiology. 2005; 16: 1-11. Article ID: 323082.
Van Der Pol, B., Ferrero, D. V., Buck-Barrington, L., Hook 3rd, E., Lenderman, C., Quinn, T., et al. Multicenter evaluation of the BDProbeTec ET system for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in urine specimens, female endocervical swabs, and male uerthral swabs. J Clin Microbiol. 2001; 39(3): 1008–16.
Workowski, K. A., Bachmann, L. H., Chang, P. A., Johnston, C. M., Muzny, C. A., Park, I., et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021; 70(4): 1-187.
Janssen, K. J., Hoebe, C. J., Dukers-Muijrers, N. H., Eppings, L., Lucchesi, M., and Wolffs. P. F. Viability-PCR Shows That NAAT Detects a High Proportion of DNA from Non-Viable Chlamydia trachomatis. PLoS One. 2016; 11(11): e0165920.
Guillot, X., Delattre, E., Prati, C., and Wendling, D. Destructive septic arthritis of the sternoclavicular joint due to Neisseria gonorrhoeae. Joint Bone Spine. 2012; 79(5): 519-20.
Zaia, B. E. and Soskin, P. N. Images in emergency medicine. Man with severe shoulder pain. Gonococcal arthritis of the shoulder. Ann Emerg Med. 2014; 63(5): 528-71.
-Marika L. Forsythe, MD is a PGY1 Pathology Resident at University of Chicago (NorthShore). Her academic interests include molecular diagnostics and its growing importance in the field of Pathology.
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
While SARS-CoV-2 testing may be dominating discussions, I wanted to highlight other important, but lesser known molecular microbiology tests, starting with BK virus.
About BKV
BK virus (BKV), a member of the Polyomaviridae family, has a tropism for uroepithelial cells and causes disease in immunosuppressed patients, particularly those who have undergone renal transplants.1,2,3 The vast majority of immunocompetent adults are infected with BKV, with estimates up to 90%, and the bulk of cases are entirely asymptomatic.1,3 The exact method of transmission is unknown,3,4 but respiratory transmission is hypothesized. BKV can remain latent after initial infection and can reactivate when immunosuppressed.4 Intermittent asymptomatic viral shedding in urine is particularly common in pregnant individuals or elderly individuals.2
In renal transplant patients, BKV can lead to significant damage to the transplanted kidney and graft failure.1 Polyomavirus-associated nephropathy (PVAN) can occur.2 In bone marrow transplant recipients, hemorrhagic cystitis can occur as a result of this virus.2 Other organ systems can be impacted although much more infrequently.4
The Lab’s Role in Diagnosis and Monitoring BKV
Given the profound impact on renal transplant patients in particular, these patients are routinely screened for BKV both in the blood and the urine. Importantly, BKV can be shed asymptomatically in the urine and thus correlation with BKV detection in the blood is essential. Molecular testing is the method of surveillance. There are currently no FDA approved assays for BKV so labs that perform testing use laboratory-developed tests with analyte specific reagents or research use-only kits.1
Quantification is necessary for monitoring. As with any quantitative assay, there must be at least one negative control, one high positive control, and one low positive control included per run. All controls should fall within the linear range of the assay. To monitor for amplification inhibition, an internal control should be included for each sample.1
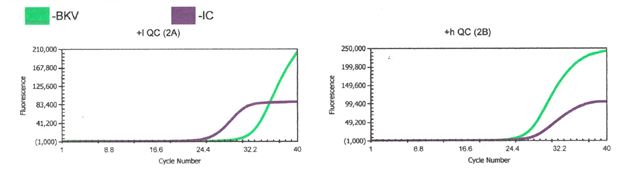
Image 1. Example of low (left) and high (right) positive controls.
We perform a BKV LDT assay here using Diasorin reagents and instrumentation. The green line is BKV target while the purple line is the internal control (IC). We run a low positive, high positive, and negative control with every run. Director review for all control and patient results is required. We use commercial BKV positive controls, which have established acceptable range that the quantification of controls must fall within for the run to be considered valid.
The Results and How They Impact Patient Care
Currently, there are no targeted treatments for BKV. In renal transplant individuals, modulation of immunosuppression is the main approach for managing BKV.3,4 A delicate balance must be achieved as reducing immunosuppression can lead to organ rejection while high levels of BKV can cause organ failure.
References
2016. 12.3 Molecular Methods for Identification of Cultured Microorganisms, Leber AL Clinical Microbiology Procedures Handbook, 4th Edition. ASM Press, Washington, DC. doi: 10.1128/9781683670438.CMPH.ch12.3
Gregory A. Storch and Richard S. Buller, 2019. Human Polyomaviruses, In: Carroll KC, Pfaller MA Manual of Clinical Microbiology, 12th Edition. ASM Press, Washington, DC. doi: 10.1128/9781683670438.MCM.ch108
Furmaga J, Kowalczyk M, Zapolski T, et al. BK Polyomavirus-Biology, Genomic Variation and Diagnosis. Viruses. 2021;13(8):1502. Published 2021 Jul 30. doi:10.3390/v13081502
Mark D. Reploeg, Gregory A. Storch, David B. Clifford, BK Virus: A Clinical Review, Clinical Infectious Diseases, Volume 33, Issue 2, 15 July 2001, Pages 191–202, https://doi.org/10.1086/321813
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
An 18 year old healthy female presented to the emergency department of a tertiary care hospital in Minnesota for headache, vomiting, and sore throat. She did not have any significant past medical history. Due to meningitis concerns, lumbar puncture and head computed tomography (CT) imaging were performed. The CT scan showed an accumulation of fluid in the posterior right frontal sinus with scattered mucosal thickening. However, her cerebrospinal fluid (CSF) profile was insignificant, with normal protein and glucose levels. CSF culture was ordered, and two sets of blood cultures were drawn.
Based on the examination and presenting symptoms, pharyngitis was suspected, and she was discharged with Amoxicillin (500mg Q6H for five days). However, her strep throat screening returned negative. Her blood culture was negative. CSF culture was also negative. Cryptococcal antigen and Enterovirus PCR were performed; however, both results were negative.
She returned to the ED two days later for a worsening headache and newly developed photophobia. Additional history revealed that she went swimming in a lake two weeks prior to her first presentation at the ED. Her CSF was sent for the Ova and Parasite (O&P) exam for suspicious parasitic meningitis. The CSF O&P test was negative. CSF PCR for amoeba was also performed at a reference laboratory, and the results came back positive with Balamuthia mandrillaris. The patient was then given flucytosine, fluconazole, and azithromycin.
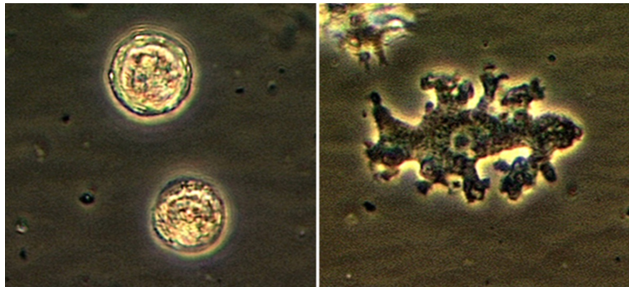
Figure 1. Photo Credit CDC: Balamuthia – free living parasite observed under light microscopy.
Discussion
Balamuthia mandrillaris belongs to a group of free-living amoebae, including Acanthamoeba species and Naegleriafowleri, that cause fatal encephalitis.1Balamuthia mandrillaris is the only known species of the genus Balamuthia that causes infections in humans. Encephalitis caused by B. mandrillaris is known as granulomatous amoebic encephalitis (GAE). GAE is characterized as a subacute to a chronic infection that can last several months to years.2 GAE differs from primary amoebic meningoencephalitis (PAM) caused by Naegleria fowleri, which typically causes an acute onset lasting a few days.
While ecological niches of B. mandrillaris are not well understood, they have been reported to be isolated from dust, soil, and water.r Both trophozoite and cyst forms can enter the body through the nasal passage or ulcerated/broken skin; however, the trophozoite stage causes associated disease manifestation and represents a diagnostic stage.2
Brain-eating amoebas are traditionally difficult to diagnose. Hematology and chemistry profiles of CSF of affected individuals are generally unremarkable, although, sometimes, increased monocytes and lymphocytes, along with increased protein levels, are seen in some cases of GAE.3
The most common method of laboratory diagnosis of B. mandrillaris is a microscopic examination of CSF wet mount (Figure 1) or via immunohistochemical staining of CSF or brain biopsy.1 With advancements in technology, species-specific nucleic acid amplification tests (NAAT) can be performed to diagnose B. mandrillaris infection accurately. However, there is no commercially available NAAT for the free-living amoeba. Only very few laboratories, such as State departments of health laboratories, Centers for Disease Control (CDC) and Prevention, or commercial reference laboratories, develop these tests as a laboratory-developed test (LDT). Histological assessment of biopsies from brain lesions may reveal tumor-like appearance or perivascular monocytic necrosis of affected areas.1 While there have been significant technological advancements, the prognosis stays at less than a 5% survival rate,6 with only roughly 25% of cases diagnosed antemortem. One possible reason for delayed laboratory diagnosis is the challenges in performing the microscopic examination in clinical microbiology laboratories since it requires expertise for accurate identification of the organism. Additionally, most clinical microbiology laboratories do not readily have an in-house LDT for free-living amoeba NAAT. Therefore, the turnaround time for diagnosing B. mandrillaris or any free-living amoeba is typically longer when specimens have to be sent out to reference laboratories.
Diagnosis of B. mandrillaris encephalitis solely based on clinical symptoms is often challenging due to similar presentation in other causes of infectious encephalitis. B.mandrillaris can affect both immunocompetent and immunocompromised individuals.1,3,4 The first B. mandrillaris case was reported in a deceased baboon in the San Diego Zoo in 1986.1 The majority of patients were diagnosed postmortem.1 While most B. mandrillaris infections are actively acquired through nasal passages or skin penetration, rare post-mortem cases of passive transfer of the organism from organ transplantation have been reported.6 With technological advancement, there have been successes in pre-mortem diagnoses in recent years.1,4 According to the known cases, individuals of Latin American origin are more likely to contract the disease; it is unknown if it is due to increased exposure or a genetic predisposition.1 Similar to other free-living amoebae, B. mandrillaris can be generally found in warmer climates or tropical regions. Of approximately two hundred cases reported worldwide, about 34 were reported in Latin America, from Mexico to Brazil, while some were from Japan, New Zealand, England, and other European countries. The Southwestern United States also contributes 30 cases, mostly in Arizona, Texas, and California.1 In the United States, there have only been 109 cases directly reported to CDC from 1974 to 2016.2,7 We believe that this is the first case of Balamuthia reported in Minnesota. The number of exact cases would be difficult to be determined due to misdiagnosis and rare occurrence of the disease or cases not reported to CDC or the state department of health.
While investigational drugs for B. mandrillaris GAE are in development, combination therapy of flucytosine, fluconazole, pentamidine, and azithromycin or clarithromycin has shown successes.2 Our patient was successfully treated with flucytosine, fluconazole, and azithromycin.
Kofman A, Guarner J. Free Living Amoebic Infections: Review. J Clin Microbiol. 2021 Jun 16:JCM0022821. doi: 10.1128/JCM.00228-21. Epub ahead of print. PMID: 34133896.
Pietrucha-Dilanchian, P., Chan, J. C., Castellano-Sanchez, A., Hirzel, A., Laowansiri, P., Tuda, C., Visvesvara, G. S., Qvarnstrom, Y., & Ratzan, K. R. (2011). Balamuthiamandrillaris And Acanthamoeba Amebic Encephalitis With Neurotoxoplasmosis Coinfection in a patient with Advanced HIV Infection. Journal of Clinical Microbiology, 50(3), 1128–1131.
Ong TYY, Khan NA, Siddiqui R. 2017. Brain-eating amoebae: predilection sites in the brain and disease outcome. J Clin Microbiol 55:1989 –1997. https://doi.org/10.1128/JCM. 02300-16.
Centers for Disease Control and Prevention. 2011. Balamuthia mandrillaris transmitted through organ transplantation—Mississippi, 2009. Am J Trans-plant 11:173–176. https://doi.org/10.1111/j.1600-6143.2010.03395_1.x.
Jennifer R Cope, Janet Landa, Hannah Nethercut, Sarah A Collier, Carol Glaser, Melanie Moser, Raghuveer Puttagunta, Jonathan S Yoder, Ibne K Ali, Sharon L Roy, The Epidemiology and Clinical Features of Balamuthia mandrillaris Disease in the United States, 1974–2016, Clinical Infectious Diseases, Volume 68, Issue 11, 1 June 2019, Pages 1815–1822, https://doi.org/10.1093/cid/ciy813
-Alejandro Soto, MLS (ASCP)CM is a junior medical technologist who is passionate about clinical microbiology.
-Phyu M. Thwe, Ph.D., D(ABMM), MLS(ASCP)CM is Microbiology Technical Director at Allina Health Laboratory in Minneapolis, MN. She completed her CPEP microbiology fellowship at the University of Texas Medical Branch in Galveston, TX. Her interest includes appropriate test utilization and extra-pulmonary tuberculosis.
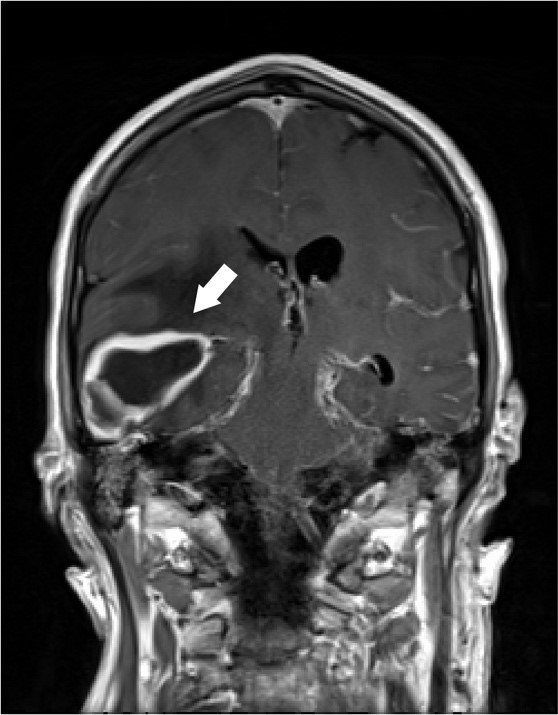
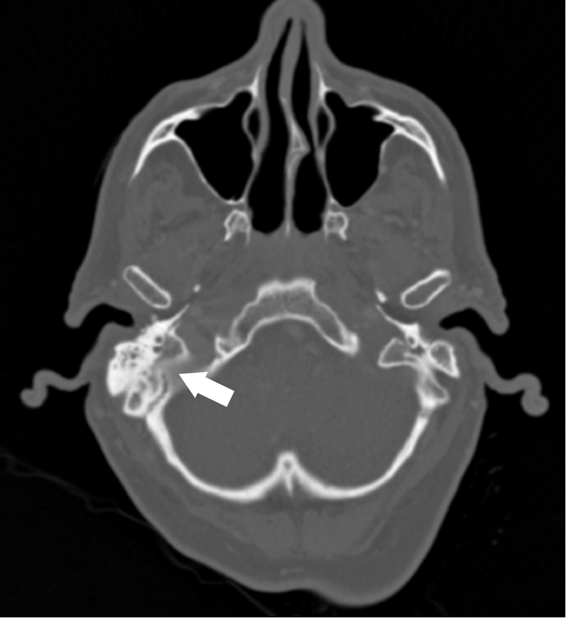
A 62 year old male with unknown past medical history was dropped off at the emergency department by EMS after being found altered with concern for IV drug use. On presentation he was febrile to 104.5o F, tachycardic, and although he was initially responsive, his mental status deteriorated. Labs were drawn and broad-spectrum antibiotic coverage with vancomycin, cefepime, and metronidazole was initiated in the ED. He then had a tonic-clonic seizure event and was given intravenous levetiracetam. A CT brain showed a right inferior temporal lobe lesion, initially interpreted as likely glioblastoma multiforme, causing subfalcine and uncal herniation. MRI revealed a ring-enhancing mass measuring 3 cm x 3 cm x 3 cm in the right temporal lobe with significant surrounding edema. CT of the temporal bones also revealed right mastoiditis (Figures 1 and 2).
Figure 1. Coronal T1 post-contrast MRI demonstrating the ring-enhancing mass in the right temporal lobe (arrow). Figure 2. CT of temporal bones with IV contrast demonstrating opacification of the right mastoid air cells and abnormal soft tissue within the epitympanum (arrow).
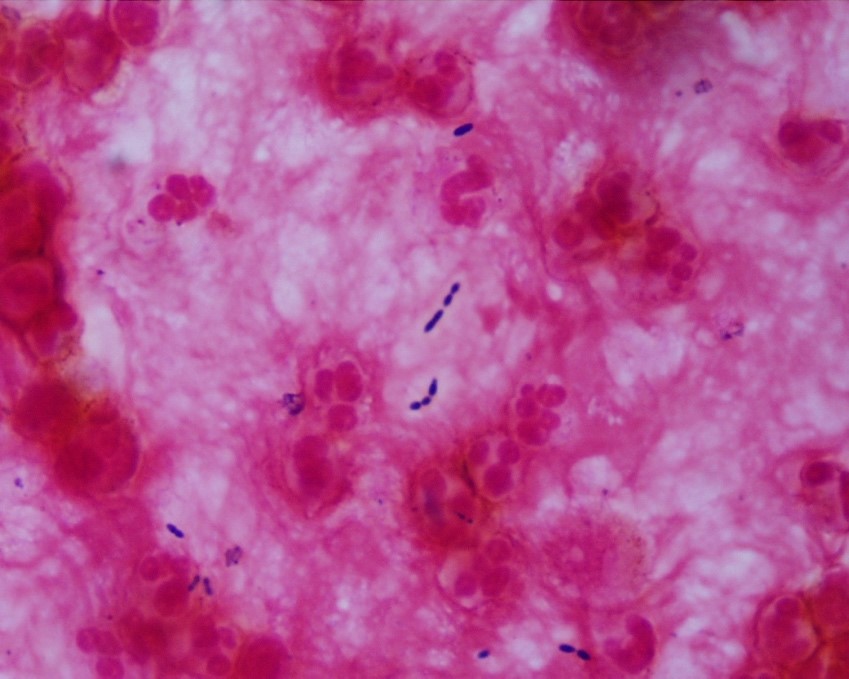
Neurosurgery evacuated 17 mL of fluid from the mass and a ventricular drain was placed. Gram stain of the evacuated fluid identified many white blood cells and few gram-positive cocci in pairs, chains and clusters (Figure 3). Postoperatively, the patient was mechanically ventilated and medicines were used to support his blood pressure in the ICU. Broad-spectrum antibiotics were continued for CNS penetration and activity against possible oral flora.
Figure 3. Representative Gram stain of the pus drained from the abscess. Multiple couplets of lancet-shaped gram positive organisms identified. Slight halo around the bacteria suggests the presence of a capsule.
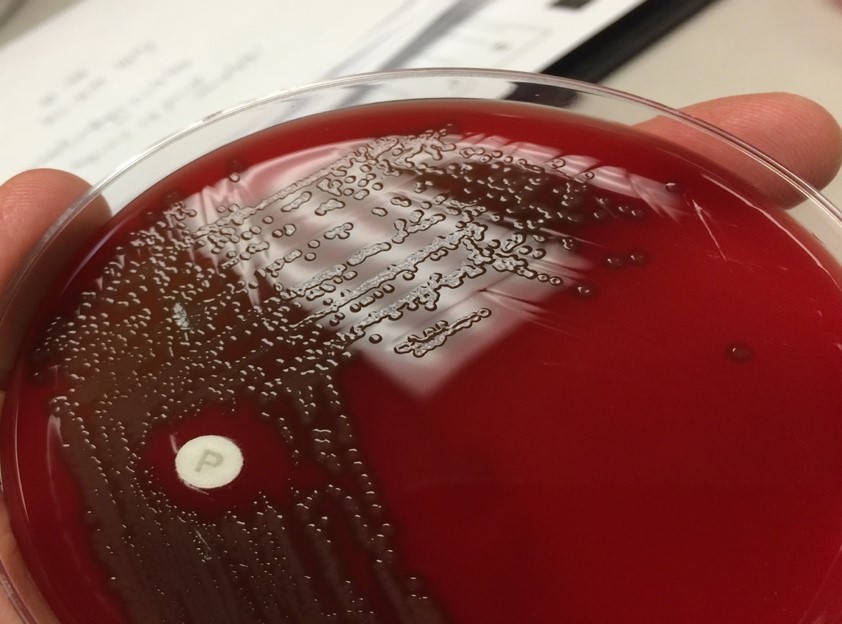
An aerobic culture of drained contents from the brain ultimately grew characteristic alpha-hemolytic colonies with central umbilication (Figure 4) which were subsequently identified by MALDI-TOF and optochin disk as Streptococcus pneumoniae. Admission blood cultures also grew Streptococcus pneumoniae with characteristic “bullet-” or “lancet-shaped” gram-positive cocci in pairs on Gram stain. Fungal and acid-fast bacillus cultures had no growth. Following susceptibility testing; antibiotic coverage was narrowed to IV Penicillin G.
Figure 4: Representative, archival image of a blood agar plate with alpha-hemolytic, centrally umbilicated colonies and optochin susceptibility (P disk).
The patient remained unresponsive and required continued intensive medical support. Although blood cultures were sterilized, he continued to have fevers and persistent leukocytosis. Gram stain of ventricular drainage re-demonstrated gram positive diplococci. The patient was transitioned to comfort care and expired on day 5 of hospitalization, the cause of death was sepsis.
Discussion
This case of a brain abscess demonstrates an unusual intracranial complication of Streptococcus pneumoniae. S. pneumoniae (or pneumococcus) is a commensal of the upper respiratory tract (URT) and important opportunistic pathogen. Up to 65% of children and less than 10% of adults are colonized by S. pneumoniae. Dissemination of S. pneumoniae beyond its niche in the nasal mucosa leads to a spectrum of disease including lobar pneumonia, meningitis, sepsis, sinus infections and middle ear infections.1 Local dissemination of S. pneumoniae to the central nervous system (CNS) is the most common intracranial complication of otitis media and mastoiditis. These patients can present with fulminant “otogenic” meningitis. About a third of these cases require myringotomy or mastoidectomy.2 Focal parenchymal brain infection by pneumococcus, however, is uncommon.
This patient presented with signs of mass effect due to a large temporal lobe abscess warranting emergent neurosurgery. Broadly, focal parenchymal brain infections arise either by hematogenous dissemination of organisms or contiguous spread from an adjacent infection. The age, immune status, and any underlying disease present in the patient help predict the pathogen. Brain imaging is also helpful. Hematogenous spread, usually from endocarditis, tends to produce multiple lesions at the grey-white matter junction,3 while direct seeding causes solitary lesions.4,5 In this older patient with a relatively intact immune system and a possible history of intravenous drug use, hematogenous spread of bacteria was considered. However, a large single lesion in the temporal lobe with a plausible adjacent nidus (opacified mastoid air cells) is most consistent with contiguous spread.
A wide range of organisms should be considered when evaluating brain abscesses, though S. pneumoniae is a relatively rare culprit. A meta-analysis of 9,699 patients with brain abscesses found that S. pneumoniae was isolated from only 2.4%.6 The most common organisms were streptococci of the viridans group (34%) and Staphylococcus spp., most commonly S. aureus (18%). Even among patients with otogenic intracranial abscesses, S. pneumoniae is rarely implicated. Interestingly, the pathogen most frequently isolated from otogenic brain abscesses is Proteus mirabilis.7,8
Once S. pneumoniae was identified, susceptibility testing was required to rule out acquired resistance to beta lactam and cephalosporin antibiotics, which is mediated by altered penicillin-binding proteins (PBPs).9 A more stringent susceptibility minimal inhibitory concentration (MIC) breakpoint applies to S. pneumoniae meningitis than other infections to account for drug distribution into the CNS.10 The hospital antibiogram reports that 97% of S. pneumoniae isolates are susceptible to Penicillin at MICs acceptable for treating non-meningitis infection but only 53% are susceptible at MICs for meningitis. Furthermore, 3.3% of all strains reported in the United States between 2001 and 2005 were also significantly resistant to ceftriaxone.11 This patient was covered by broad spectrum antibiotics until susceptibility testing demonstrated sensitivity to both penicillin and ceftriaxone.
References
1 Weiser, J. N., Ferreira, D. M. & Paton, J. C. Streptococcus pneumoniae: transmission, colonization and invasion. Nat Rev Microbiol16, 355-367, doi:10.1038/s41579-018-0001-8 (2018).
2 Kaplan, D. M., Gluck, O., Kraus, M., Slovik, Y. & Juwad, H. Acute bacterial meningitis caused by acute otitis media in adults: A series of 12 patients. Ear Nose Throat J96, 20-28 (2017).
3 Bakshi, R. et al. Cranial magnetic resonance imaging findings in bacterial endocarditis: the neuroimaging spectrum of septic brain embolization demonstrated in twelve patients. J Neuroimaging9, 78-84, doi:10.1111/jon19999278 (1999).
4 Brouwer, M. C., Tunkel, A. R., McKhann, G. M., 2nd & van de Beek, D. Brain abscess. N Engl J Med371, 447-456, doi:10.1056/NEJMra1301635 (2014).
5 Miller, J. M. et al. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiology. Clin Infect Dis67, e1-e94, doi:10.1093/cid/ciy381 (2018).
6 Brouwer, M. C., Coutinho, J. M. & van de Beek, D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology82, 806-813, doi:10.1212/WNL.0000000000000172 (2014).
7 Duarte, M. J. et al. Otogenic brain abscesses: A systematic review. Laryngoscope Investig Otolaryngol3, 198-208, doi:10.1002/lio2.150 (2018).
8 Kangsanarak, J., Fooanant, S., Ruckphaopunt, K., Navacharoen, N. & Teotrakul, S. Extracranial and intracranial complications of suppurative otitis media. Report of 102 cases. J Laryngol Otol107, 999-1004, doi:10.1017/s0022215100125095 (1993).
9 Chen, L. F., Chopra, T. & Kaye, K. S. Pathogens resistant to antibacterial agents. Infect Dis Clin North Am23, 817-845, vii, doi:10.1016/j.idc.2009.06.002 (2009).
10 Weinstein, M. P., Klugman, K. P. & Jones, R. N. Rationale for revised penicillin susceptibility breakpoints versus Streptococcus pneumoniae: coping with antimicrobial susceptibility in an era of resistance. Clin Infect Dis48, 1596-1600, doi:10.1086/598975 (2009).
11 Sahm, D. F. et al. Tracking resistance among bacterial respiratory tract pathogens: summary of findings of the TRUST Surveillance Initiative, 2001-2005. Postgrad Med120, 8-15, doi:10.3810/pgm.2008.09.suppl52.279 (2008).
–Miles Black, Ph.D. is a fourth-year medical student in the Medical Scientist Training Program at UT Southwestern Medical Center. His background is in enzyme biochemistry and Legionella pathogenesis.
–Denver Niles, MD is the Medical Microbiology fellow at UT Southwestern Medical Center. Prior to his Medical Microbiology fellowship, he completed pediatric infectious disease training at Baylor College of Medicine/Texas Children’s Hospital.
–Dominick Cavuoti, D.O. is a professor of Pathology at UT Southwestern Medical Center who specializes in Medical Microbiology, ID Pathology and Cytology.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
Pre-analytic factors contribute to over 70% of laboratory errors. The most common examples include missing test request, wrong/ missing ID, contamination from collection site, hemolyzed/ clotted/ insufficient sample, wrong container or wrong transport conditions.
In our NGS lab, pre-analytic factors rarely arise. Sometimes an incorrect slide was sent, so then the tumor and germline DNA don’t match. We do perform many rounds of PCR (total 30-35 cycles), so contamination of amplified PCR products could be a concern. Usually, our volume is low enough that contamination isn’t a significant issue and not one we have noticed.
Multiple mutations- A COVID-19 Hybrid?
In a batch of COVID-19 whole genome sequencing samples from early July, I noticed some interesting mutations. Mutations from the Alpha and Delta variants were showing up in the same specimen. At first I thought this could mean a hybrid virus. Another possibility was co-infection in the same patient. And lastly, the specimen could just be contaminated. The best way to resolve this issue is to check the “phase” of the viral variant sequencing reads. The phase refers to the single pieces of DNA that are read by the sequencer. They are normally short (75-150bp in length), but if you can see whether the variants occur on the same read or only on different reads it rules out the possibility of a hybrid virus.
Image 1. Hybrid (or chimeric) cat.
Determining the difference between a hybrid or 2 viral genomes
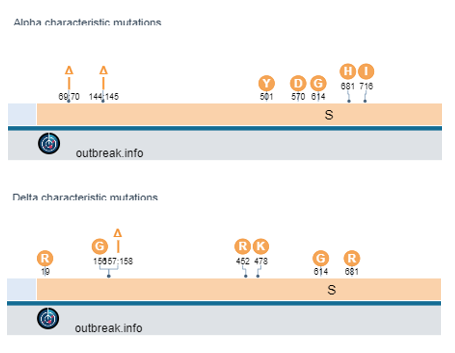
The difficulty is finding a location within both the Alpha and Delta variants that have mutations close to each other. One region exists near a deletion at amino acid 144 (Alpha) and amino acids 157-158 (Delta).
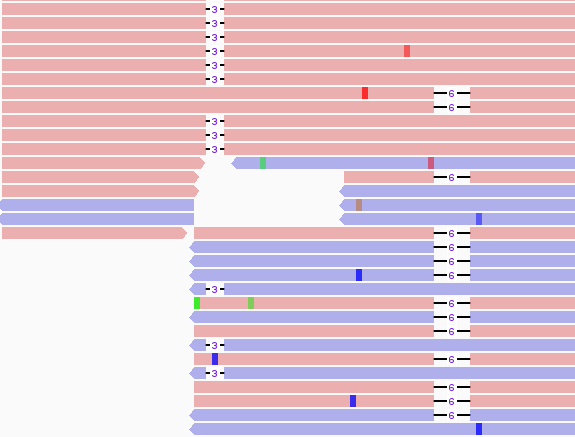
Figure 1. Characteristic mutations of Alpha (top) and Delta (bottom) variants. The deletions (triangle sign) are located close to each other, so were evaluated for phase. Figure 2. Integrated Genome View (IGV) display of mutations. 6 base pair deletion (bars next to 6) is characteristic of Delta while a 3 base pair deletion (bars next to 3) is characteristic of Alpha.
Tracing the source of the issue
As there were no overlaping reads with the 3 b.p. and 6 b.p. deletion, we concluded that this finding arose from 2 distinct viral genomes. As to whether the person was infected with both Alpha and Delta, we looked to the rest of our 96 well plate. A characteristic muation in Alpha spike protein is N501Y (it confers increased binding to ACE2R and increased infectivity). This mutation was found in several specimens of the Delta lineage, but in this case there was a much lower frequency of this variant compared to total reads. Also, several of the cases had high CT values to start with. Many of the contaminated samples also were near a variant that mapped strongly to Alpha and had a lower Ct value (CT=25). Mapping the location of the specmens to the plate showed close proximity to the authentic Alpha variant.
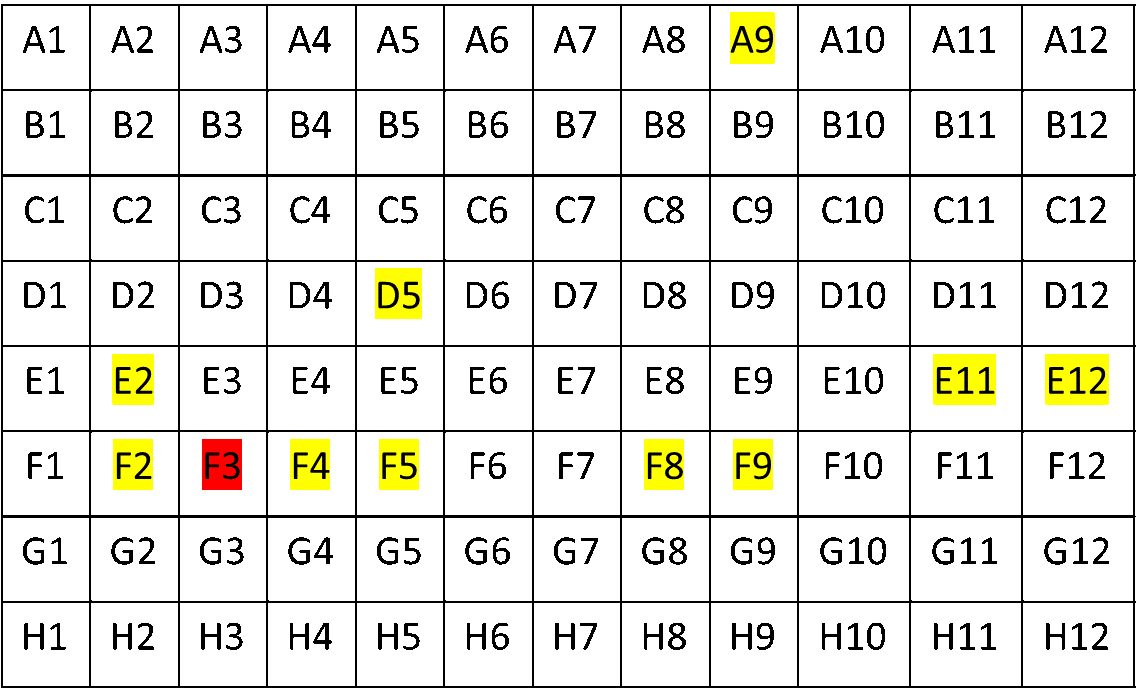
Figure 3. Red squares: PCR=B.1.1.7; others are PCR=B.1.1.7, but yellow highlighting indicates N501Y detected in WGS.
Luckily, before all WGS testing, we perform a targeted PCR, which I’ve mentioned in previous blog posts. This showed that only one sample (well F3) was B.1.1.7, and the rest were Delta variants. Thus we concluded we had experienced a case of contamination.
Since this time, we’ve had issues with the negative control having borderline positive levels of sequencing data that maps to Delta (now 100% of all cases and with low CT values). This is apparently a problem at multiple labs, but one that we are trying to address by looking at several root causes.
Pre-analytic concerns: Contamination sources
COVID-19 viral genome sequencing has found issues of contamination in several circumstances. We attribute this to a few reasons:
High viral load of some specimens (especially Delta)
Thin plastic covers that pop off easily, especially when taken out of the freezer
And a large volume of specimens being processed.
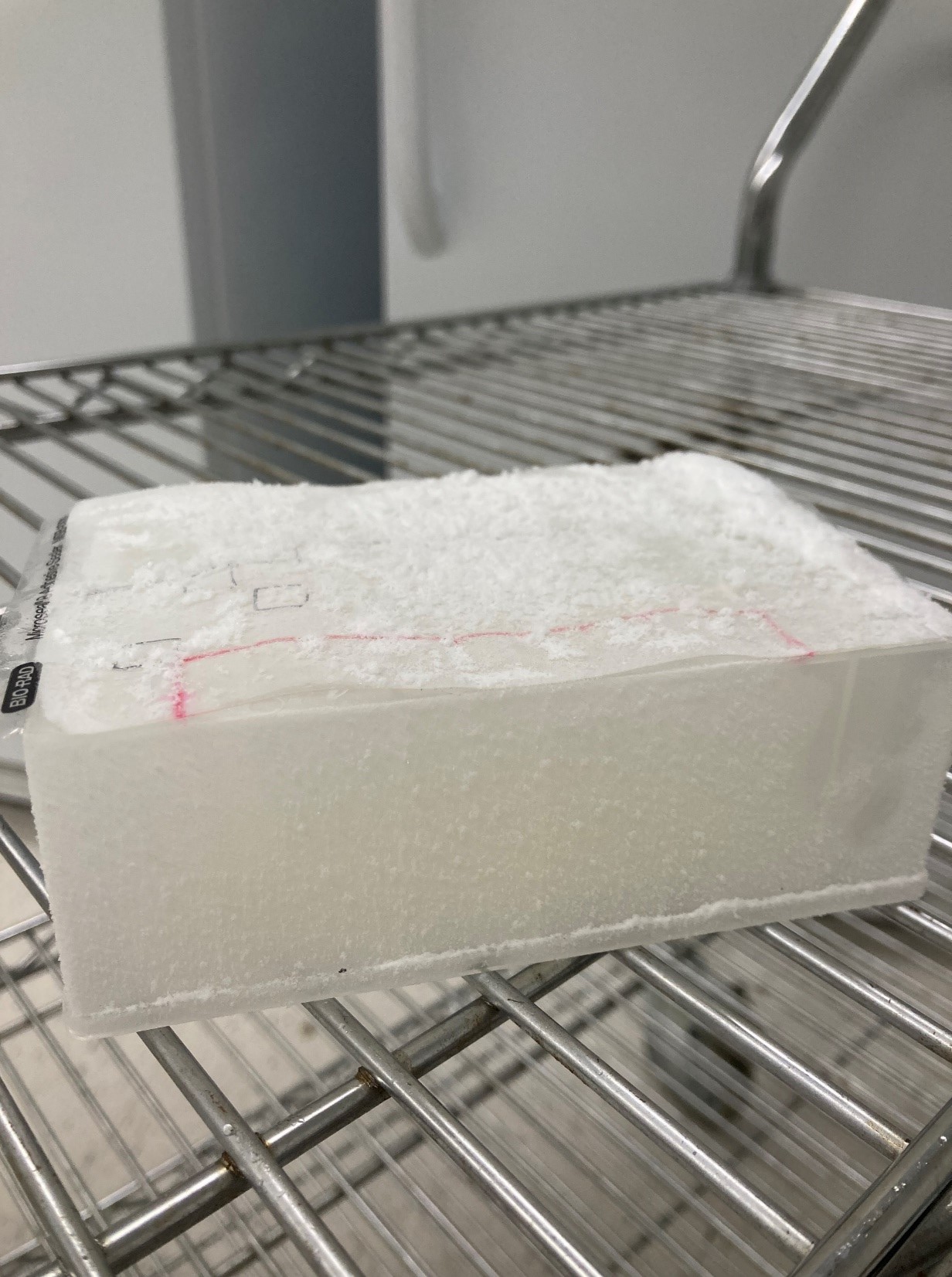
For an example of the plastic cover issue, you can see this picture below where the cold temperature of -80C causes the plastic film adhesive to come off quickly as it is removed from cold storage. It makes popping sounds and could aerosolize viral particles to other wells in the plate.
Image 2. 96 deep well plate of extracted RNA with a thin plastic cover that comes off as the plates is thawed.
We now use aluminum PCR plate covers that do not come off with freeze/ thaw transitions. Furthermore, we use a multi-channel pipette that pieces the cover to withdraw individual samples without exposing them to other wells.
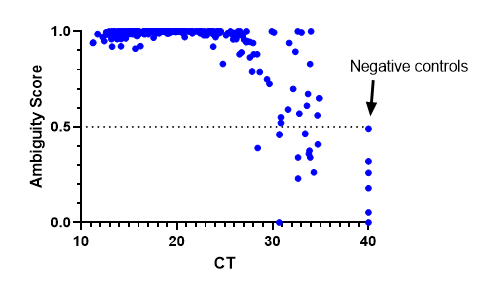
We have also implemented bioinformatic QC metric cut-offs to determine where a cut-off for negative specimens should be. We decided on an ambiguity score <0.5. The results were consistent with previous findings where lineages could be assigned at a CT >30, but sometimes they failed as CT values increased. Negative controls were assigned a CT of 40 and all fell below the 0.5 cut-off. This has been a useful metric to be sure we are providing high quality results.
Concluding remarks
Pre-analytic factors impact every part of testing and as COVID-19 sequencing has shown, even the NGS lab tests are not immune to these challenges.
The targeted PCR test helped flag/ resolve several of the issues as they arose.
COVID-19 sequencing is still for research/ epidemiologic purposes and demonstrates the importance of rigorous clinical validations to mitigate issues such as carry-over.
References Lippi G, Chance JJ, Church S, Dazzi P, Fontana R, Giavarina D, et al. Preanalytical quality improvement: from dream to reality. Clin Chem Lab Med. 2011;49:1113–26.
-Jeff SoRelle, MD is Assistant Professor of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX working in the Next Generation Sequencing lab. His research interests include the genetics of allergy, COVID-19 variant sequencing, and lab medicine of transgender healthcare.Follow him on Twitter @Jeff_SoRelle.