While SARS-CoV-2 testing may be dominating discussions, I wanted to highlight other important, but lesser known molecular microbiology tests, starting with BK virus.
About BKV
BK virus (BKV), a member of the Polyomaviridae family, has a tropism for uroepithelial cells and causes disease in immunosuppressed patients, particularly those who have undergone renal transplants.1,2,3 The vast majority of immunocompetent adults are infected with BKV, with estimates up to 90%, and the bulk of cases are entirely asymptomatic.1,3 The exact method of transmission is unknown,3,4 but respiratory transmission is hypothesized. BKV can remain latent after initial infection and can reactivate when immunosuppressed.4 Intermittent asymptomatic viral shedding in urine is particularly common in pregnant individuals or elderly individuals.2
In renal transplant patients, BKV can lead to significant damage to the transplanted kidney and graft failure.1 Polyomavirus-associated nephropathy (PVAN) can occur.2 In bone marrow transplant recipients, hemorrhagic cystitis can occur as a result of this virus.2 Other organ systems can be impacted although much more infrequently.4
The Lab’s Role in Diagnosis and Monitoring BKV
Given the profound impact on renal transplant patients in particular, these patients are routinely screened for BKV both in the blood and the urine. Importantly, BKV can be shed asymptomatically in the urine and thus correlation with BKV detection in the blood is essential. Molecular testing is the method of surveillance. There are currently no FDA approved assays for BKV so labs that perform testing use laboratory-developed tests with analyte specific reagents or research use-only kits.1
Quantification is necessary for monitoring. As with any quantitative assay, there must be at least one negative control, one high positive control, and one low positive control included per run. All controls should fall within the linear range of the assay. To monitor for amplification inhibition, an internal control should be included for each sample.1
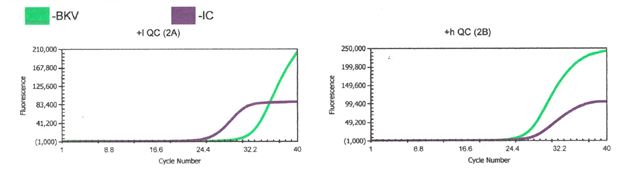
We perform a BKV LDT assay here using Diasorin reagents and instrumentation. The green line is BKV target while the purple line is the internal control (IC). We run a low positive, high positive, and negative control with every run. Director review for all control and patient results is required. We use commercial BKV positive controls, which have established acceptable range that the quantification of controls must fall within for the run to be considered valid.
The Results and How They Impact Patient Care
Currently, there are no targeted treatments for BKV. In renal transplant individuals, modulation of immunosuppression is the main approach for managing BKV.3,4 A delicate balance must be achieved as reducing immunosuppression can lead to organ rejection while high levels of BKV can cause organ failure.
References
- 2016. 12.3 Molecular Methods for Identification of Cultured Microorganisms, Leber AL Clinical Microbiology Procedures Handbook, 4th Edition. ASM Press, Washington, DC. doi: 10.1128/9781683670438.CMPH.ch12.3
- Gregory A. Storch and Richard S. Buller, 2019. Human Polyomaviruses, In: Carroll KC, Pfaller MA Manual of Clinical Microbiology, 12th Edition. ASM Press, Washington, DC. doi: 10.1128/9781683670438.MCM.ch108
- Furmaga J, Kowalczyk M, Zapolski T, et al. BK Polyomavirus-Biology, Genomic Variation and Diagnosis. Viruses. 2021;13(8):1502. Published 2021 Jul 30. doi:10.3390/v13081502
- Mark D. Reploeg, Gregory A. Storch, David B. Clifford, BK Virus: A Clinical Review, Clinical Infectious Diseases, Volume 33, Issue 2, 15 July 2001, Pages 191–202, https://doi.org/10.1086/321813

-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
