A 77 year old male with history of asthma, atrial fibrillation, and recurrent respiratory distress when visiting Vermont presented to the ED with progressive dyspnea and wheezing for the past 4 days. Two days prior, he required a “breathing treatment” at his PCP. One day ago, he saw his PCP and was prescribed prednisone and azithromycin. He denies cough, fevers, or chills. He used his albuterol and Advair inhalers which barely helped. He was found to be in Afib with RVR to the 160s, a respiratory rate in the 40s, and an oxygen saturation of 70%.
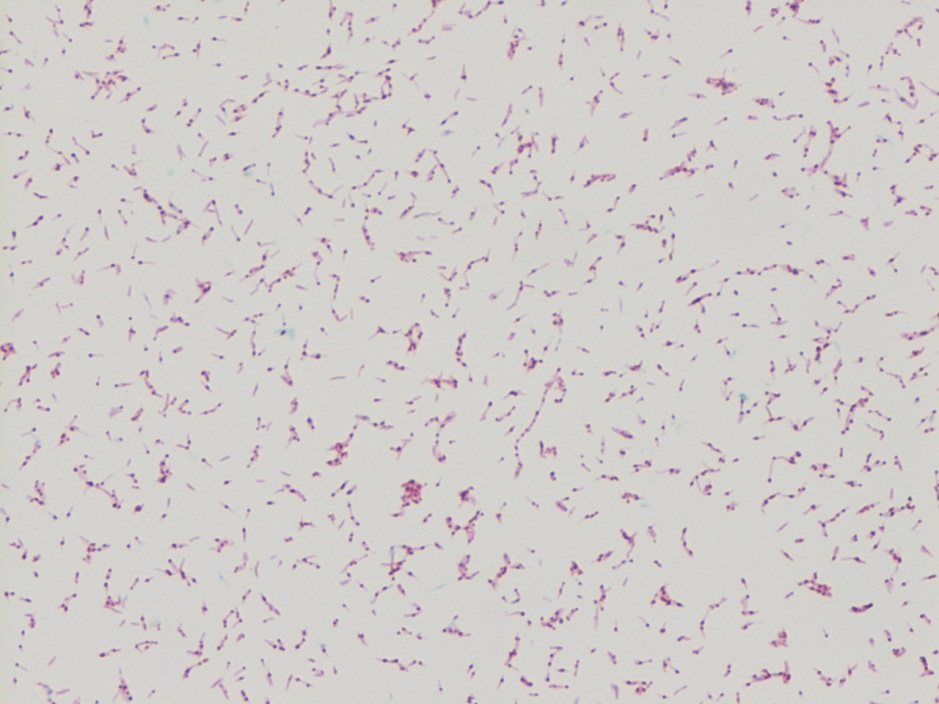
Kinyoun stain revealing broad rods with cross-barring.Colony growth on Lowenstein-Jensen medium.
Lab Identification
The organism was auramine fluorescent stain positive from the broth. The AFB culture bottle was sub-cultured to agar based medium and Lowenstein-Jensen medium, which yielded small yellow colonies. Kinyoun stain revealed broad rods with cross-barring. The organisms produced a yellow pigment when exposed to light, and a nucleic acid probe for Mycobacterium kansasii was positive.
Discussion
Mycobacterium kansasii was discovered in 1953 by Buhler and Pollack. It is an acid fast bacillus that produces yellow pigment when exposed to light (photochromogen). The bacilli are thick, long and cross-barred and have been described as ladder-like. It is prevalent in the Midwest and Southeast, and is the second most common cause of nontuberculous mycobacteria disease in patients with AIDS. Mycobacterium kansasii manifests as lung disease that clinically appears similar to tuberculosis. It can also cause local disease of the skin and subcutaneous tissue, as well as lymphadenitis and disseminated disease. Symptoms are more severe in immunocompromised hosts. Mycobacterium kansasii is generally acquired via either aspiration or local inoculation from the environment, with little evidence to support person to person transmission.
-Mustafa Mohammed, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 6 year-old girl with a history of posterior fossa ependymoma presented with a one month history of fever, headaches, vomiting and more recently, neck stiffness. Additional history includes remote tumor resection followed by radiation and chemotherapy resulting in remission, with a residual ventriculoperitoneal shunt (VPS). Her parents reported she was in good health until approximately 1 month prior to presentation and is up to date on her immunizations. She was previously seen by her primary care physician for her symptoms and treated her with amoxicillin for suspected strep throat. Upon admission, she received supportive therapy for her symptoms after she was found to have tumor recurrence on imaging. The patient was scheduled for resection approximately two weeks after discharge and on post-operative day two she developed fever, vomiting and neck stiffness again. At this time, blood cultures were drawn and a lumbar puncture (LP) was performed. Cerebrospinal fluid (CSF) from both the LP and VPS submitted for fluid analysis (Table 1) and culture.
Table 1: Cerebrospinal Fluid Analysis
Spinal Fluid
LP
VPS
Appearance
Clear
Clear
Nucleated cells
1075 cells/μL
628 cells/μL
RBC
150 cells/μL
35 cells/μL
Polys
94%
87%
Lymphs
2%
6%
Mono/Macrophage
4%
7%
Glucose
68 mg/dL
13 mg/dL
Protein
69 mg/dL
164 mg/dL
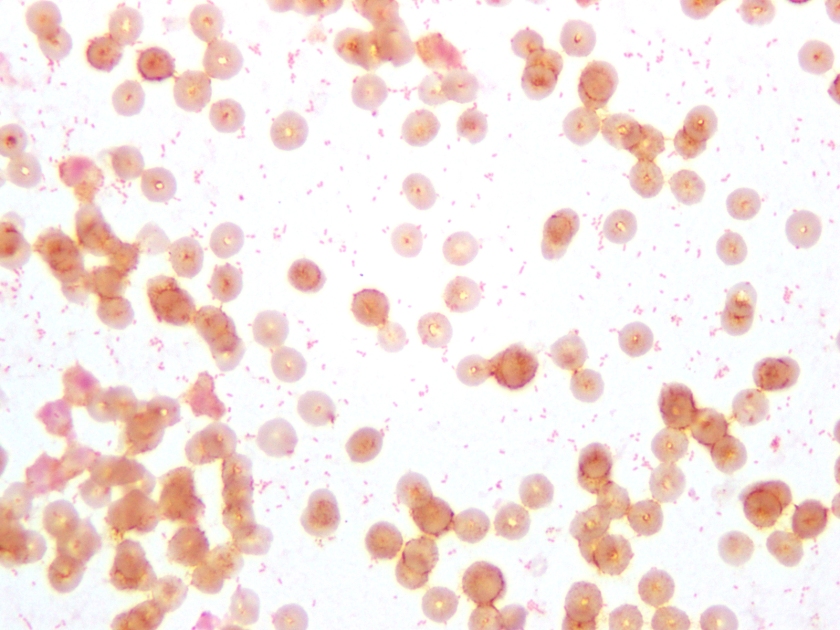
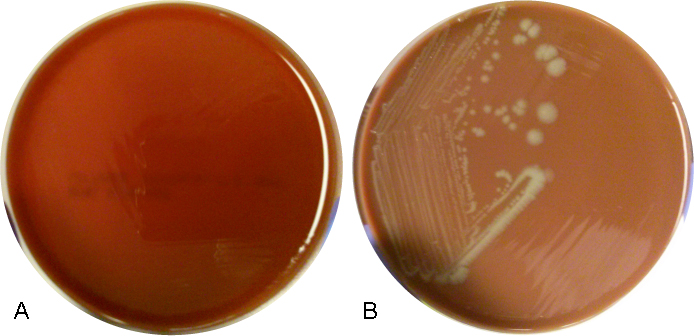
Figure 1. Gram stain of the pathogen isolated from aerobic blood culture, showing gram-negative coccobacilli, sometimes in pairs. The same organism was seen on the patient’s CSF Gram stain.Figure 2. Aerobic blood culture on (A) 5% sheep blood agar plate (BAP), showing no growth and on (B) chocolate agar plate (CAP), showing round, smooth, opaque grey-yellow colonies.
Culture results:
The CSF Gram stain showed rare, paired, Gram-negative diplococci, which could raise suspicion for Neisseria meningitidis, however the typical flattened sides of adjacent bacteria were not observed. Rather, the morphology was more consistent with Gram-negative coccobaccilli, which is better demonstrated on Gram stain of the blood culture (Figure 1). Culture of both the CSF and blood specimens grew fairly large, smooth, round, opaque grey-yellow colonies on CAP, however showed no growth on BAP (Figure 2), suggesting a fastidious organism requiring growth factors. The colonies were both catalase and oxidase positive. The organism was identified as Haemophilus influenzae by MALDI-TOF MS (matrix-assisted laser desorption/ionizations time-of-flight mass spectrometry). This H. influenzae isolate was non-typeable by slide agglutination serotyping performed at the state public health laboratory.
Discussion:
H. influenzae are small, pleomorphic, gram-negative rods or coccobacilli that are non-motile. They are facultative anaerobes that grow best between 35-37°C with 5% CO2. H. influenzae is a fastidious species, requiring hemin (X factor) and nicotinamide-adenine-dinucleotide (NAD/V factor) for growth, which are both available in chocolate agar, but not blood agar. On chocolate agar, the colonies are non-hemolytic, typically large, smooth, round and convex with an opaque, colorless or grey hue. Encapsulated strains, including H. influenzae serotype b (Hib), appear mucoid and are typically small, grey colonies on CAP. Isolates are catalase and oxidase positive. H. influenzae displays the “satellite phenomenon” when grown near Staphylococcus aureus. This occurs when colonies of S. aureus lyse nearby red blood cells releasing hemin and NAD in the media. The presence of extracellular hemin and NAD allow colonies of H. influenzae to grow in the immediate vicinity of S. aureus.
H. influenzae is widely distributed in humans, colonizing the nose and throat and is spread from person-to-person via direct contact or respiratory droplets. Severe infections, including pneumonia, bacteremia and meningitis, affect predominantly infants and children. The American Academy of Pediatrics recommends routine vaccination with the Hib conjugate vaccine for infants aged 2 through 6 months (2 or 3 doses, depending on vaccine product) followed by a booster dose at age 12 through 15 months. Hib is the only serotype preventable by vaccine. Prior to routine vaccination in the US, approximately 20,000 children under the age of 5 were infected with H. influenzae and 3-6% died each year.
-Petra Rahaman, MD is a 4th year Anatomic and Clinical Pathology resident at UT Southwestern Medical Center.
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
The manager of the microbiology laboratory walked into the monthly staff meeting to discuss safety. Her first announcement was that the one clean hand washing sink in the department was going to be removed. The techs were shocked, and some were angry. Didn’t the manager care about infection prevention and control? Didn’t she know that hand hygiene should always occur after PPE is removed and before leaving the lab? The manager waited for the reactions to subside, then she explained that since the staff treated the lab as a clean area in many instances, that there should be no need for hand washing. The staff went on to argue that they were working with microbiological pathogens, and that they did wear lab coats and gloves, especially when handling specimens and setting them up for cultures. Some of those specimen containers were pretty disgusting, in fact.
That was when the manager dropped the charade. She had no real intention of removing the sink, but she wanted to make a point. She was tired of watching her staff reading culture plates with no gloves. She had spoken about it before, but no one agreed- they had been handling incubated plates for years.
One of the most common issues lab managers and safety professionals face is maintaining Personal Protective Equipment (PPE) compliance in the work area. An effective weapon in this battle is telling stories of lab incidents with bad outcomes, or explaining the consequences of this unsafe behavior. That is a valuable piece of lab safety education. It is unfortunate that we sometimes have to learn from others’ mistakes, but when it comes to safety, that’s better than learning from your own. Some lab accidents and exposures can be career-altering or career-ending.
OSHA’s Bloodborne Pathogen Standard states that PPE (specifically gloves) must be worn when there is a risk of exposure. That is as specific as they get on the topic. Anytime patient specimens are handled or opened, it follows that gloves should be worn. That means that in the microbiology area, staff is handling specimens and agar plates with gloves while they streak plates and set up gram stain slides. These contaminated gloves are handling plate after plate, and then those plates are placed into the incubators. Like any other contaminated item in the lab, those plates should be treated and handled with gloves until properly discarded. That means that gloves are necessary when removing plates from the incubator, and when reading those cultures. Not only is staff handling contaminated plates, but they are working with bacterial and fungal colonies. There is a high risk of exposure in those processes.
OSHA also requires PPE under its Chemical Hygiene Standard (or Lab Standard). Gloves are required when handling chemicals, so they would be needed when performing simple chemical tests (oxidase, catalase, etc.) and when performing gram stains. Make sure you use chemical-resistant gloves when selecting the appropriate PPE for these tasks.
In 2010, OSHA responded to an inquiry specifically about the use of gloves while handling culture plates in the microbiology laboratory. The letter “strongly suggests” the use of gloves for the task, but OSHA’s own standards already address the issue and clearly require the need for PPE in that situation.
The story at the beginning of this entry is true- there was a lab manager who was fed up with her staff not wearing gloves, so she told them she was removing the sink. She was kidding, but she made her point. In that microbiology lab they all wear gloves to read cultures today.
Laboratory-acquired infections occur every year, and some of the easiest ones to investigate are the cases in which techs are infected with pathogenic bacteria. It is fairly easy to trace the sources of those exposures. What is the staff doing in your microbiology laboratory? Are they doing everything they can to prevent exposure to pathogens? As a manager or safety professional, are you enforcing the use of PPE when exposure is possible? Keep your staff from becoming a safety statistic- provide PPE, teach consequences of unsafe behaviors, and monitor the continual use of those safe work practices in your lab.
-Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
A 12 year old girl who recently emigrated from Nepal was seen in clinic to establish care. She was entirely asymptomatic. Stool ova and parasite exam was performed and on the permanent trichrome-stained section, the following parasites were identified.
Image (A)Image (B)Image (C)Image (D)Image (E)
Laboratory Identification:
The first image (A) is morphologically diagnostic for Dientamoeba fragilis trophozoites. They are approximately 10 microns in diameter and have 1-2 nuclei, which appear fractured. The next two images are diagnostic for Endolimax nana cysts (B) and trophozoites (C). The cysts are approximately 7 microns in diameter and most have 4 nuclei with blot-like karyosomes that are red on trichrome stain with clearing around the nuclei. The trophozoites are approximately 10 microns in diameter with a single large blot-like karyosome that is red on trichrome stain. The last two images are diagnostic for Entamoeba coli cysts (D) and trophozoites (E). The cysts are approximately 20 microns in diameter and have five to eight nuclei with karyosomes that are red on trichrome stain. The trophozoites are approximately 22 microns in diameter and have a single nucleus with a large kayosome that is darkly staining on trichrome stain. There is peripheral chromatin that is ring-like or clumped.
Discussion:
Dientamoeba fragilis, an ameboflagellate, is a potential pathogen that can be associated with diarrhea, vomiting, abdominal pain, and anorexia, particularly in children. Transmission is via ingestion of contaminated food and water. Some studies postulate co-transmission via helminth eggs, particularly with Enterobius vermicularis. Historically, this intestinal parasite is only known to have a trophozoite form. However, there are now case reports describing the presence of cysts and precysts in humans.1 Treatment is with metronidazole or paromomycin in patients who are symptomatic.
Endolimax nana and Entamoeba coli are protozoa that are considered non-pathogenic and therefore no treatment is necessary. However, when identified, they should be reported since their presence indicates exposure to contaminated food and water. Transmission is via ingestion of cysts. Once in the small bowel, they ex-cyst and migrate to the large bowel where they divide by binary fission and produce cysts. Both cysts and trophozoites are passed in stool.
Reference
Stark D, Garcia LS, Barratt JLN, Phillips O, Roberts T, Marriot D, Harkness J, Ellis JT. Description ofDientamoeba fragilis cyst and precystic forms from human samples. Journ Clin Micro. 2014; 52: 2680-2683.
-Joanna Conant, MD is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 33 year old African American female presents to the hospital complaining of mild abdominal pain for the past couple of days. She is 17 weeks pregnant and has a history of two prior spontaneous abortions at 15 and 16 weeks due to a shortened cervix. She is afebrile and denies any vaginal bleeding or leakage of amniotic fluid. A complete blood count reveals mild leukocytosis and anemia. On physical examination, her cervix is 2 cm dilated with bulging membranes. She is admitted for a possible cerclage placement, and an amniocentesis is performed to rule out infection prior to the procedure. The microbiology lab received 20 ml of clear, amber fluid for Gram stain and bacterial culture.
Figure 1. Direct Gram stain from the amniotic fluid showing many neutrophils and fusiform Gram negative bacilli (1000x oil immersion).Figure 2. Wright-Geimsa stain of the amniotic fluid specimen containing many acute inflammatory cells which have engulfed the fusiform bacteria (1000x oil immersion).Figure 3. Small, greyish-white colonies growing on Brucella blood agar after 48 hours of incubation under anaerobic conditions at 35°C.
Laboratory Identification:
The Gram stain showed moderate fusiform Gram negative bacilli in a background of many acute inflammatory white blood cells. Bacterial cultures grew small, greyish-white colonies as Brucella blood agar and routine blood agar after 48 hours of incubation under anaerobic conditions at 35°C. No growth was observed on kanamycin-vancomycin laked blood (KVLB) agar. The organism was identified by MALDI-TOF as Fusobacterium nucleatum and confirmed using the Vitek anaerobic identification card.
Discussion:
Fusobacterium nucleatum is an anaerobic, Gram-negative rod that is non-spore forming. It is considered normal flora of the oral cavity and gastrointestinal & genitourinary tracts of healthy adults. F. nucleatum has been implicated in the pathogenesis of oropharyngeal infections, especially in neutropenic patients with mucositis after receiving chemotherapy or bone marrow transplant. It is an important etiologic agent in a wide spectrum of extraoral infections including bacteremia, brain abscess, osteomyelitis and infections of the genitorurinary tract, including the fetal membranes. There have been many documented cases linking infections with F. nucleatum to chorioamnionitis, preterm birth, and neonatal sepsis. The mode of transmission of F. nucleatum to the amniotic fluid can be as a result of direct extension from the vaginal tract, hematogenous spread or as recently implicated, orogenital transmission.
Given that F. nucleatum is the most common of Fusobacterium species found in clinical specimens and it’s potential to cause significant disease, early identification of the pathogen is important. It grows well on a non-selective anaerobic agar and its growth is inhibited on Bacteroides bile esculin (BBE) and kanamycin-vancomycin laked blood (KVLB) agars. After 48 hours of incubation under anaerobic conditions, the colonies measure 1-2 mm in diameter and have been noted to have a characteristic internal flecking quality that is referred to as “speckled opalescence”. On Gram stain, the fusiform cells of F. nucleatum are long (usually 5-10 µm in length), slender filaments with tapered ends and may contain spherical swellings. In regards to biochemical testing, it is indole positive and lipase negative. Disk testing for Fusobacterium spp. shows the bacteria are resistant to vancomycin and susceptible to kanamycin and colistin.
While susceptibility testing is not routinely performed for all anaerobes, testing is indicated for organisms in pure culture isolated from normally sterile sites or for those more virulent organisms for which susceptibilities cannot be predicted. In the case of Fusobacterium spp., penicillin and ampicillin resistance among isolates of has been reported due to beta-lactamase production and it is recommended that all Gram negative anaerobes have a beta-lactamase screen performed. F. nucleatum is routinely susceptible to metronidazole, clindamycin and beta-lactam beta-lactamase inhibitor combination antibiotics.
In the case of our patient, her diagnosis of F. nucleatum in the amniotic fluid specimen precluded her from obtaining a rescue cerclage procedure. She was transferred to labor and delivery for a uterine evacuation secondary to the intra-amniotic infection and delivered a non-viable fetus. She received ampicillin and gentamicin as intravenous antibiotics.
-Brooke Sims, MD, is a third year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories.
Dr. Diamond from the Washington University School of Medicine talked with Lab Medicine about all things Zika Virus: a brief history of the virus, modes of transmission, and the implications for laboratory professionals and pathologists.
An 84 year old man with atrial fibrillation, coronary artery disease status post bypass surgery, and type II diabetes with chronic peripheral neuropathy presented to the ED with weakness, multiple falls, back pain, chills, and confusion. He was found to have a fever of 102o F. A workup for sepsis was performed but no source of infection was identified. Blood cultures were drawn and the patient was started on broad spectrum antibiotics. Fevers, chills, and confusion improved but patient continued to have back pain. A CT scan showed a pathologic fracture of L3 vertebrae, presumed to be secondary to infection with adjacent myositis.
Multiple blood culture bottles were positive for the organism with the following Gram smear morphology and colony morphology on blood agar.
Laboratory Identification:
Gram smear showed Gram negative cocobacilli. The colonies were gray-white on blood agar, colorless on MacConkey and oxidase negative. The organism was identified as Yersinia pseudotuberculosis by MALDI-ToF and confirmed by VITEK.
Discussion:
Yersinia pseudotuberculosis is a gram negative bacillus that belongs to the Enterobacteriaceae family and therefore ferments glucose, is oxidase negative, and can reduce nitrates to nitrites. This bacterium is endemic in a wide variety of animals and is presumed to be a possible foodborne pathogen due to similarities to Yersinia enterocolitica. There have been reported cases of outbreaks associated with milk and iceberg lettuce sprayed with untreated water. Growth is optimal at 25-32o C, but can grow at 4o C. Infection is rare but typically causes enterocolitis and ileitis. Children may present with mesenteric lymphadenitis, which may mimic acute appendicitis. Sepsis is rare but is associated with those with underlying disorders such as cirrhosis, hemochromatosis, and diabetes. Reported mortality rates may be as high as 75% despite proper antibiotic treatment.
In this patient, it was determined that the most likely source of infection was consumption of raw milk. Due to presumed vertebral and paravertebral soft tissue involvement, he was treated with six weeks of IV ceftriaxone.
-Joanna Conant, MD is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A young girl presented to the emergency department with 6 days of cough, congestion, and intermittent fever up to 102°F. Respiratory viral testing, blood cultures, and a chest x-ray were ordered. The patient was found to be RSV positive and sent home with oral steroids. Two days later she presented the emergency department once again with worsening respiratory symptoms and a positive blood culture with the following organism (Figure 1).
Figure 1. Gram stain demonstrating Gram-positive cocci in pairs and chains.
Our patient developed a Streptococcus pneumoniae superinfection and bacteremia in conjunction with RSV pneumonia.
Identification
S. pneumoniae is a Gram-positive cocci that forms “lancet” shaped pairs on Gram stain (Figure 1). Due to pretreatment with antibiotics, our Gram stain shows some pairs, but many Gram variable chains of cocci as well. S. pneumoniae grows as alpha hemolytic colonies on 5% sheep blood, chocolate, and CAN (colistin nalidixic acid) agar in 12-18 hours, where it forms umbelicated colonies with a characteristic navel-like depression in the middle due to autolysins produced by the bacterium. Some serotypes of S. pneumoniae, primarily serotype 3, have a mucoid phenotype seen in Figure 3. S. pneumoniae is a member of the Streptococcus mitis group, but due to its pathogenic potential it has always been singled out. This is accomplished using two biochemical tests: bile solubility testing with 10% deoxycholate, which dissolves colonies of S. pneumoniae but not those of other Viridans group streptococci, and optochin disc testing, to which S. pneumoniae is sensitive while other Virdians group streptococci are resistant (Figures 2 and 3). Many molecular assays have trouble differentiating S. pneumoniae from S. mitis group due to their similarities on a nucleotide and protein level, so biochemical testing is still a mainstay of organism identification.
Figure 2. Growth of α-hemolytic bacterial colonies on 5% sheep blood agar. Zone around the disc indicates the organism is optochin susceptible.
Figure 3. Growth of mucoid, α-hemolytic bacterial colonies on 5% sheep blood agar. The mucoid colony morphology suggests this isolate is likely serotype 3.
Clinical Significance
S. pneumoniae is known to cause a variety of clinical manifestations in children, from community acquired pneumonia and acute otitis media to bacteremia and meningitis. S. pneumoniae is also a colonizer of the upper respiratory tract; approximately 21% of children in developed countries and 90% of children in developing countries are asymptotically colonized. Due to the high rates of S. pneumoniae colonization in children, direct urine antigen testing is inappropriate, as it cannot distinguish asymptomatic carriage from invasive disease. S. pneumoniae direct antigen detection from CSF has been shown to have < 30% sensitivity and offers no benefit over a routine cytospin Gram stain.
Vaccination in children
Around 2000 the first S. pneumoniae vaccine became available. PCV7 was a heptavalent conjugate vaccine which provided protection from the 7 most common S. pneumoniae serotypes known to cause invasive disease (4, 6B, 9V, 14, 18C, 19F, and 23F). Routine vaccination of children was a huge success which reduced the incidence of invasive pneumococcal disease attributed to vaccine strains by 99%. An indirect benefit of the PCV7 vaccine was that adults >65 years of age saw a 92% decrease in invasive pneumococcal disease caused by PCV7 serotypes, despite not being vaccinated themselves, because of reduced transmission of S. pneumoniae from children to adults. Due to the selective pressure of the vaccine, non-vaccine serotypes of S. pneumoniae such as 19A subsequently became the predominant causes of invasive streptococcal disease. In 2010, a 13-valent pneumococcal conjugate vaccine (PCV13) was FDA approved. It includes all seven S. pneumoniae serotypes contained in PCV7, plus six additional serotypes (1, 3, 5, 6A, 7F, and 19A). PCV13 provides coverage against 2/3 of all serotypes responsible for invasive pneumococcal disease in children under 5 years of age.
Follow up
The patient had an uneventful hospital stay. All subsequent blood cultures were negative and susceptibility testing found the patient’s S. pneumoniae isolate to be susceptible to penicillin, cefotaxime, and clindamycin. The patient and was discharged home after 24 hours of observation with a 7 day course of amoxicillin.
References:
Manual of Clinical Microbiology, 11th edition
Pediatric Red Book, 2015 Report of the Committee on Infectious Diseases, 30th edition
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
A group of physicians from the University of Iowa have started a dialogue about Mycobacterium chimaera infections in patients who have undergone cardiac surgery. It seems as though the bacteria finds its way to the patients via a heater-cooler device used during their procedure. If you’re a micro tech or a pathologist and you come across a cardiac patient who has a fever of unknown origin, night sweats, loss of energy, and failure to gain weight, M. chimaera is something to keep in mind.
A 45 year-old woman was hospitalized for a bilateral subarachnoid hemorrhage with right-sided intraventricular hemorrhage secondary to a basilar artery aneurysm. On hospital day 2, after endovascular coiling of her aneurysm, she developed seizure-like activity. She was found to have new bilateral thalamic and brainstem infarcts with increased hydrocephalus and had an external ventricular drain placed.
She showed some minimal neurological improvements over the next 2 weeks until hospital day 17 when her mental status acutely declined and she developed a fever, leukocytosis, and meningeal signs. 8cc of cloudy, yellow fluid was collected via lumbar puncture. Analysis of the fluid showed pleocytosis (cell count of 54K) with a neutrophil predominance and markedly elevated protein.
CSF Gram stainCSF Gram stainCSF aerobic culture on blood agarCSF aerobic culture on MacConkey
Laboratory Identification:
Initial review of the spinal fluid gram stain showed many polymorphonuclear leukocytes and what appeared to be paired gram negative cocci suspicious for Neisseria meningitidis. However, many organisms lacked the more characteristic “kidney-bean” shape. Further inspection of the gram stain revealed many gram negative organisms which more closely resembled bacilli. Given the patient’s history and clinical course, it was determined the pathological agent was most likely a gram negative coccobacillus. On culture, the bacteria formed smooth, round, opaque colonies on Blood and Chocolate agar and was lactose non-fermenting on MacConkey agar. The bacterial colonies were also oxidase negative.
Mass spectrometry identified the organism as Acinetobacter radioresistens.
Rare gram positive appearing organisms of similar shape were also located on the gram stain. This demonstrates that Acinetobacter is known to occasionally retain the crystal violet stain leading to cases of initial misidentification.
Discussion:
Acinetobacter radioresistens is one of about 30 species of bacteria included in the Acinetobacter genus. Acinetobacter is characterized as a gram negative, aerobic coccobacillus which is non-motile, non-fermentative, and oxidase-negative. It grows well on standard aerobic media and typically forms smooth, round, mucoid colonies at 37°C. Acinetobacter is a water organism which preferentially colonizes aquatic, humid, and tropical environments; perhaps accounting for the increased incidence of Acinetobacter infections between the months of July and October.
While there have been reported cases of community-acquired Acinetobacter pneumonia in Southeast Asia and Australia, in most areas of the world Acinetobacter is known primarily as an agent of nosocomial infections. Studies show that an estimated 33% of healthcare workers are colonized with Acinetobacter and that it is one of the most prevalent bacteria isolated from the white coats of medical students. Despite its ubiquity in hospitals, Acinetobacter infections are relatively rare. Many patients may be colonized with it, but Acinetobacter only usually causes disease in immunocompromised and/or critically-ill patients with long hospitalizations. At particular risk are ventilated patients supported with multiple lines, drains, and catheters. Acinetobacter is reported as the pathological agent in a small percent of ventilator-associated pneumonias, central line-associated bloodstream infections, catheter-associated urinary tract infections, and surgical site infections. It is also recognized as a cause of nosocomial meningitis in neurosurgical patients with external ventricular drains, especially those with a history of intracranial hemorrhage and recent prior antibiotic therapy.
Acinetobacter infections are of particular concern because several species demonstrate resistance to many antimicrobials. Acinetobacterbaumanni, the species responsible for the majority of Acinetobacter infections, has demonstrated resistance to 1st-3rd generation cephalosporins, macrolides, penicillins, and aminoglycosides. Because these infections are robust and difficult to treat, patients with Acinetobacter infections have a 25-75% mortality risk depending on the site of their infection and their baseline cardiopulmonary and immune status. Currently, carbapenems are considered the gold standard treatment.
-Elaine Amoresano, MD, is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.