I don’t think anyone enjoys filling out
the paperwork at a doctor’s office. For transgender individuals, this can be an
experience that ranges from irksome to offensive. Most intake forms don’t allow
for expression of their gender identity. Furthermore, confusion on gender and
sex can create real confusion and healthcare failures in several places that
laboratory medicine encounters a transgender individual.
Arguably the first place the lab
encounters a transgender patient is via the phlebotomist. These professional
collectors of blood must confirm two patient identifiers, which are often name
and date of birth. The “name” used is the legal name. Using a transgender
person’s “dead name” (name given at birth) represents a gender they do not want
to be associated with and can be a very offensive experience. “Isn’t it obvious
that name is not what I look like?”
While names can be legally changed, this
happens with varying difficulty and legal cost in different states. A solution
is to improve training of phlebotomists to explain the necessity of confirming
a legal name so lab results are properly matched to the patient. Additionally,
front-desk intake workers should be similarly trained to interact with
transgender patients when recording demographic information. This can be aided
by electronic health records (EHR) becoming more flexible and inclusive of the
gender diversity.
Traditionally, EHR would only include one
field for SEX: M or F.
Several in the laboratory community have
asked how many different gender options should be included? Facebook included
up to 71 options in 2017. That’s a big step up from the 2 traditional EHRs are
built around.
The World Professional Association for
Transgender Health (WPATH) executive committee in 2011 outlined the recommended
fields to include in EHR: preferred name, sex assigned at birth, gender, and
pronoun preference. EHRs are evolving and can be flexible depending on the user
requirements. At my program, we use EPIC at 3 different different sites (children’s,
county and university hospitals) and each has a different version.
From what I’ve seen preferred name is an easy addition and would not interfere with
functions of the EHR or Laboratory Information Systems (LIS), which is the
Lab’s version of EHR.
If the field for sex assigned at birth is different from gender, then it would clear up any confusion about whether the
person is transgender and then they should be addressed by the pronouns
matching the gender. While there is a spectrum of genders, only transgender males
and transgender females are of a high enough prevalence to have medically
relevant recommendations. Plus, if a system at least starts here, they could
expand further as necessitated by their population.
EHR could include preferred pronouns, but I haven’t seen this implemented in an EHR
yet. Ideally, you would just use the pronouns that match the intended
appearance of the individual (ma’am to someone wearing a dress, etc.).
Lastly, I think Legal sex should be added to the EHR as well. One of our hospitals
has this and it makes several processes easier such as processing hormone
medication.
Legal (or administrative) sex, sex assigned at birth, and gender data fields provide the clearest and simplest picture of a patient
and should be a minimum for labs making recommendations for changes to HER.
Next month I will describe in greater
detail the issues that can arise in the lab when gender or sex are entered
incorrectly in the system for transgender patients and how this can negatively
affect care delivery.
References
Deutsch MB, Green J, Keatley J, Mayer G, Hastings J, Hall AM, World Professional Association for Transgender Health EMR Working Group. Electronic medical records and the transgender patient: recommendations from the World Professional Association for Transgender Health EMR Working Group. J Am Med Inform Assoc. 2013 Jul-Aug; 20(4):700-3.
Gupta S, Imborek KL, Krasowski MD. Challenges in Transgender Healthcare: The Pathology Perspective. Lab Med. 2016 Aug; 47(3):180-188.
-Jeff SoRelle, MD is a Chief Resident of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and improving genetic variant interpretation.
In previous blog posts we discussed some hints and tips for how to survive when your lab is being inspected. Today we get to flip things around and let you be the inspector. Whether it’s an internal audit of your own laboratory, or an external inspection of a peer laboratory, we’ll discuss some ways to help keep you on track to cover the most important aspects of the overall testing process in a limited amount of time.
For external audit preparation, the CAP has a wonderful training program that all volunteer inspectors are required to take prior to participating in an inspection. For labs that are not CAP accredited, they still have helpful information on their website that is free and open to all: https://www.cap.org/laboratory-improvement/accreditation/inspector-training. CLSI document QMS15-A (Assessments: Laboratory Internal Audit Program; Approved Guideline) is another great resource to use when planning your audit.
The primary role of an auditor is to review policies, processes, and procedures to identify any inconsistencies (does your SOP match the manufacturer recommendations, and is staff following the SOP as written). Audits should focus on collecting objective evidence and facts, rather than subjective opinions. For example, staff failing to document required weekly maintenance tasks, as opposed to an auditor simply not liking the particular form the tasks are being documented on.
Define the Objective of the Audit
Laboratory leadership should be involved in the planning process to help define the scope and expected goal of performing the audit. This can range from an overall assessment of general laboratory quality and safety, to a more directed and focused audit on either a single department, instrument/test, or test process (specimen collection, physician notification of critical values, etc). The format for the audit findings should also be discussed – will the site require a formal, written report outlining all observations detected, or will a simple informal summation discussion be sufficient?
Draft a Schedule for the Audit
Once the scope of the audit is defined, a tentative schedule should be created so all staff involved in the audit process are aware and available to participate. If the audit will encompass multiple departments and all phases of testing (pre-analytic, analytic, post-analytic), it may be necessary to split the audit up over multiple days, or to recruit multiple auditors. The frequency of audits will depend on the perceived risk to quality based on previous findings or complaints received, but at a minimum should be completed annually.
Prepare for the Audit
Reach out to the local management team of the site being audited for help in gathering the information you’ll need to prepare. This can include things such as a testing activity menu, list of new instrumentation or new test validation studies, employee roster if personnel and competency records will be reviewed, and copies of previous audit/inspection results to check for corrective action implementation and sustainability. Review the information provided, and use it as a guide for where you feel your efforts should be focused on based on highest risk.
Utilize a Patient Tracer
Ask the site to pull all related records and reports for a particular patient sample by choosing a date, and specifying any particular characteristics for the specimen that you want to follow (such as age of the patient, sex, or focusing on abnormal/critical results). By asking the sites to prepare a patient tracer ahead of time, this will reduce the amount of time spent waiting and digging for specific files or log sheets as they are already organized and ready when you walk in for the audit. Tracers should adhere to the defined scope/objective of the audit, and will help you follow the path of a specimen through the entire process from pre-analytical, analytical, and finally post-analytical phases.
Pre-analytical: Include any specimen collection instructions or a printout/photocopy from the test directory for each test requested. This information should be compared to the information within the applicable SOPs to ensure they match and are both current and accurate. Physician orders can be included to confirm that the correct test was ordered and performed based on what was requested by the clinician.
Analytical: Copies of the related SOPs for the test being reviewed should be included. Ensure the SOPs have all required elements, including a current, valid signature of approval from the medical director. Instrument QC and maintenance logs for the day of testing, calibration records, and patient correlation studies should also be reviewed, along with the reagent lot-lot validation performed. When available, copies of the actual instrument printouts should be included to check for accuracy in result transcription. Training and competency records for the staff who performed any handling or testing of the specimens in question may also be reviewed.
Post-analytical: Check for supervisory review of patient log sheets and QC records, along with appropriate corrective actions documented as applicable. Review the patient results in the same format that is seen by the physician: confirm reference ranges and units of measure are accurate, interpretive notes are valid and appropriate, test methodology is stated when applicable, abnormal values are flagged, and confirm result transcription accuracy from the original instrument printout. Proficiency testing results should be reviewed for any unsuccessful events to confirm sustainability of corrective actions.
Conduct the Audit
Perform an objective review of the documents provided, along with any affiliated records and logs based on the scope of the audit (temperature logs, reagent inventory records, decontamination records, etc). As with an official inspection, be transparent with the staff as issues are identified so they can have an opportunity to clarify any confusion, or locate additional records that may be missing or incomplete. Document any discrepancies or possible issues noted, as well as any good lab practices observed that should be celebrated. When logging your findings, be specific and provide as much details as possible so the staff can quickly identify what was found and make the needed corrections (SOP numbers, dates, instrument serial numbers, etc).
In addition to reviewing documentation, perform a direct observation of the staff doing specific tasks. Are they following the steps outlined in their procedures, or are deviations noted? Rather than a formal interview, ask the staff to explain what they are doing, or why they are performing certain steps in a particular order. Again, the audit is not meant to be punitive or to ‘catch someone in the act’, but rather to help identify areas for improvement or clarification so that testing processes can be improved and standardized among all staff members. Asking open ended questions will provide more information than directed ones. For example, “Show me how you would access testing instructions if your computer network was down” as opposed to “Where are the paper versions of your SOPs?”
Prepare an Audit Report
The audit findings should be summarized for the site based on the format agreed upon during the initial planning stage (written report, verbal discussion). Whenever possible, similar findings should be grouped together so the location can identify systemic problems that need to be addressed on a more global level (expired reagents found in multiple departments, staff failing to utilize appropriate PPE in multiple departments, etc). Depending on the number and severity of the issues identified, sites may prefer to have the observations grouped by department as well for easy assignment of follow-up action items to the department leaders. Issues should also be ranked by risk severity so that the site knows where to focus their improvement efforts first: 1) Patient care and employee safety issues; 2) Regulatory compliance gaps; 3) Recommendations for improved overall good laboratory practice.
Implement Corrective Actions
Any issues identified during the audit should be assigned to a specific person for follow-up, along with an anticipated date of completion. Perform a proper root cause analysis to identify why the issue happened, and then decide how to correct it and prevent it from happening again. Depending on the scope of the audit, the audit team members may be involved with these tasks, or this may fall to the sole responsibility of the management team being inspected.
Evaluate the Effectiveness of the Audit
The utility of the audits will depend greatly on the commitment of laboratory leadership to both implement, and sustain, effective corrective actions based on the quality gaps identified. This can be assessed by the overall level of compliance with the regulations being checked, and comparing the results of this audit to previous and subsequent ones to hopefully show a downward trend in potential citations detected. The audit team should obtain feedback on the audit process to assess the inspected lab’s overall satisfaction with the program, the amount of support offered to the inspected laboratory, effectiveness of communication between the teams, and any potential areas for improvement in the process.
Performing internal audits is a great way to meet regulatory, accreditation, and customer requirements. It allows you an opportunity to identify non-conformances and risks that can affect both quality, and patient/employee safety. By performing regularly scheduled internal audits, not only will staff members become more experienced and better prepared for the official external inspections from regulatory and accrediting agencies, but the laboratory will move from a culture of reactive, corrective actions to that of a proactive model of continual improvements.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018 Top 5 in the 40 Under Forty recognition program. She has worked in the medical laboratory profession for over 18 years. In her current position, she transitions between performing laboratory audits across the entire Northwell Health System on Long Island, NY, consulting for at-risk laboratories outside of Northwell Health, bringing laboratories up to regulatory standards, and acting as supervisor and mentor in labs with management gaps.
In general, there are two reasons employees in the laboratory
should care about proper waste disposal. Improper disposal is expensive. Laboratorians
like raises, bonuses, and updated equipment, but there is less money for those
things when paper items are tossed into sharps containers or when used gloves go
into red bag trash containers. Labs in many states also risk large fines if items
with biohazard symbols are disposed of into regular trash containers. The other
reason to care about trash disposal involves the environment. Regulated Medical
Waste (red bag trash and sharps) has to be treated, and some of it is
incinerated while some ends up in special biohazard landfills. Both of those
are things we want less of in our environment.
As a lab safety professional, you may know of several other
reasons to implement and maintain proper lab waste segregation, but in my years
of safety training, money and the environment are the two that tend to hit home
with staff. There are multiple waste streams generated in the lab setting, and
while management in some departments may choose to offer only biohazard waste
receptacles for everything, the safety savvy professional knows this is
wasteful and perhaps a bit lazy. With proper education and training, laboratorians
are capable of goo trash segregation that meets the regulations and meets best
practice standards.
Appropriate trash segregation in the lab requires knowledge
about what waste goes into what type of container, and it requires availability
and proper placement of those containers. If a processing department only uses
red bag trash cans, for example, then much of the non-hazardous waste will end
up there. Assess the laboratory areas for proper placement of all necessary
types of waste receptacles.
In one lab, it was discovered that staff was throwing out
urine containers with embedded needles into red bag trash containers. Why?
There simply were no sharps containers in the area. It was a simple fix to move
containers nearby, but no one was paying attention, and there could have been an
unnecessary needle stick exposure. In another lab staff emptied urine sample
cups into the sink and tossed them into regular trash bins. From a waste
standpoint, that was fine, but because there was patient information on the
container labels, HIPAA violations occurred.
Many venipuncture sample tubes used today are plastic, and
they cannot be broken to create sharp edges. Given that, those items could be
disposed of into biohazard trash bags. That can save a lab some money by
reducing the volume of sharps containers used (they are more expensive to
handle). However, glass specimen tubes are still available for purchase. Be
sure to check for these in your racks before throwing out all lab tubes into a
plastic bag. A broken tube can cause a very unfortunate exposure event.
Place patient information and extra labels into bins for
shredding if available. Teach staff that in most cases it is acceptable to
place used disposable lab coats and gloves into regular trash receptacles
provided they are not visibly bloody. Other items can go into the regular waste
stream such as plastic transfer pipettes, gauze pads, and paper towels (again,
provided there is no blood visible on them).
If items can be broken to create a sharp edge, they should
be disposed of into a sharps container. That includes specimen cups made of
hard plastic, sharp pipette tips, and any glass item. Agar plates and wooden
applicator sticks should also go into a sharps container. Remember, if the item
breaks while a trash bag is handled, an employee may become exposed, and the
incident would need to be treated as an unknown source exposure, something that
should always be avoided.
Make sure staff know the proper disposal of chemical waste
as well. Never pour chemical waste down the drain unless your facility has a
permit to do so. Place chemical waste containers in appropriate locations and
label them according to EPA regulations. Provide proper training for employees
who sign waste manifests when hazardous waste is hauled away from the lab.
If
you take the easy route and combine all of your laboratory waste, you would be
responsible for both increased departmental expenses and for unnecessarily
adding bio-waste to the environment. Talk regularly to your group of trained lab
scientists about proper waste segregation, use signage as reminders, and assess
their lab waste knowledge regularly. Proper waste management takes work. Mistakes
can be made easily, and some of them can cause injury and invoke heavy fines. Invest
in a robust laboratory waste management program to avoid those issues and to
create a safety savvy example for others.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Last
month we discussed the rules associated with evaluating your PT results, and
how to investigate any unsuccessful surveys. In the last of this 3-part series
we’ll review ways to utilize your PT reports to check for trending in your patient
values – shifts, trends and bias. Your PT results can help show you developing
problems and allow you to correct them, before they become failures or begin to
affect patient care. Before declaring a failure as a ‘random error’, be sure
that it truly is.
Accuracy & Systematic Errors
Accuracy
describes how close your measured value is to the reference value – did you
obtain the correct result? This will be affected by systematic errors, such as
using expired or degraded reagents, changes in lot numbers or calibration
values, or instruments with analytical lamps or lasers near the end of their
use life. Systematic errors are reproducible inaccuracies that occur in the
same direction; all results will be falsely low or all results will be falsely
high. If systematic errors are present, all results will show similar
deviations from the true value. Bias is a measure of how far off your results
are from their true intended value.
Precision and Random Errors
Precision
on the other hand refers to the overall agreement of results upon replicate
testing – will you get the same value if you repeat the test? Precision is
affected by random errors, such as incomplete aspiration of a sample or reagent
due to fibrin clots or air bubbles, operator variability in pipetting technique,
or temperature fluctuations. Random errors are statistical fluctuations in the
measured data due to the limitations of the assay in use. These errors will
occur in either direction from the mean, unlike systematic errors that will be
on the same side. Imprecision can be measured and monitored by evaluating the
standard deviation (SD) and coefficient of variance (CV) for an assay.
Let’s
look at some example PT results from CAP, and see what hints these reports
reveal to us.
Albumin: Although all results passed and were graded as ‘acceptable’, there are still issues that should be looked into. For the last 3 surveys in a row, the plot shows that nearly all samples have been on the same right side of the mean. When comparing the value of the % relative distance from the first survey to the most recent one, you can see that the values are trending worse and getting closer to being unacceptable if the pattern continues. Additionally, be mindful of the standard deviation index (SDI) value reported. This is a measure of your bias, and how far off your values are from the mean. It should be defined within your Quality System Manual (QSM) the values which should trigger an investigation, but as a general rule, anything >±2.0 indicates a potential issue. (https://unityweb.qcnet.com/Documentation/Help/UnityWeb/399.htm)
Alkaline Phosphatase: Again all results passed, but 3/5 samples have SDI values >±2.0. The first survey had all values to the right of the mean, the second survey was a nice tight even mix of +/- bias, and now with the most recent survey all values are appearing to the left of the mean. If this shift coincides with a change in lot number, a calibration may be necessary to get results back on target to help lower the SDI values.
GGT: Although only 1 sample was graded as unacceptable, all of the results for this recent survey were at risk of being failures due to how close they were to the upper limit of acceptability. Results like this should be very carefully evaluated to ensure that there is no impact on patient care. Provided the sample stability has not been exceeded, all 5 samples should be repeated. If the repeat values are closer to the target mean, you will need to identify what went wrong on the day the samples were originally tested. If the repeat values are still grossly far from their intended target, a full patient lookback would need to be performed from the time the samples were originally tested until the day they were repeated, as there is a systemic problem that has now continued for weeks or longer.
Vancomycin: Similar to the albumin example above, these results show a trend occurring between the first survey and the most recent; however unlike albumin these are moving in the correct direction. Values are getting closer to the target mean, and SDI values are decreasing, suggesting that any corrective actions implemented after the last survey were successful.
Lithium: This shows a good example of what
you hope all of your quantitative proficiency results will look like. There is
a nice distribution of results on both sides of the mean, and SDI values are
all relatively low. Values such as these allow you to have complete confidence
in the accuracy of your patient results.
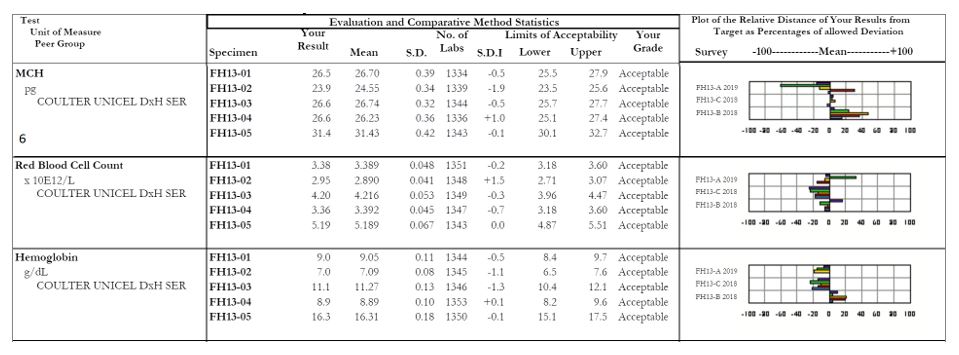
MCH: Focus on sample #2, with an SDI of -1.9. The other samples within this survey all appear fine, but it looks as though there was truly a random error with sample #2. When we look at the affiliated analytes we see a similar issue with the RBC count of sample #2, which coincides with our decreased MCH (a reminder for our non-hematology readers, MCH = (Hgb x 10)/RBC). For any calculated values, be sure to evaluate the all parameters together as well as individually to serve as a common sense check that your results are appropriate and truly make sense.
It is
important to have a robust quality assurance program that outlines what to
monitor, key decision points for when to take action, and guidance on what
those actions should include. Your proficiency testing results can provide you
with a ton of useful information to evaluate the overall quality of laboratory,
and help provide confidence in the patient values being reported out as well.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018 Top 5 in the 40 Under Forty recognition program. She has worked in the medical laboratory profession for over 18 years. In her current position, she transitions between performing laboratory audits across the entire Northwell Health System on Long Island, NY, consulting for at-risk laboratories outside of Northwell Health, bringing laboratories up to regulatory standards, and acting as supervisor and mentor in labs with management gaps.
Laboratory professionals work with vendor representatives on a regular basis, and it is important to develop a good working relationship with them to ensure continued smooth operations in the department. They provide analyzers, products, equipment, and services. However, lab managers and employees may sometimes need to pay special attention to the actions a representative will take in the department or to some of the information they may provide. They should be experts about their products and processes, but they may not always be well-versed in your lab-specific process and the regulations.
One common safety mistake representatives make has to do
with proper use of personal protective equipment (PPE). Not all vendors provide
adequate PPE training, and many of the representatives may not have a
laboratory background. Check to make sure vendors wear lab coats and gloves
when working in the lab, and offer face protection if they open up instruments
for repairs or diagnostics. Some reps bring their own lab coats and use them in
different settings where they work. This is common, but it is also a violation
of OSHA’s Bloodborne Pathogens standard. PPE used in a lab should never be
taken out of the department (except as waste). Don’t let your vendor roll up his
used lab coat and place it into his work bag for his next stop. Let him know
about the regulations and offer him a new disposable coat upon each visit.
Another common issue with lab vendor reps is the use of
laptop computers and cellphones in the laboratory. In some cases, they must use
their computers to connect to instruments or to the company control center, but
they should be decontaminated before removal from the department, especially if
they were set on top of a lab counter or analyzer. Can reps use lab phones
instead of their cell phones? It’s a worthwhile question, especially if cell
phone use is against your lab policy (it should be), and if allowing vendor use
of the cell phone will be a detriment to your lab’s safety culture. Again, as
with PPE use, this safety knowledge may not be known by the vendor company, and
certainly they need education about local policies as well.
Laboratory vendors that manufacture analyzers or that design
testing processes know their products inside and out, but their set-up work and
lab staff training should be monitored, particularly if the information
pertains to local or state regulations. For example, some lab analyzers are put
in place using an extension cord for power because the analyzer cord doesn’t
reach the outlet. In many locales, the permanent of an extension cord is not
permitted. Often a vendor will train staff to incorrectly dispose of
bio-hazardous or chemical waste. That can lead to large citations and fines if
the mistakes are not caught and corrected. If a new process or analyzer
generates a new waste stream, be sure all waste regulations are being followed.
For example, if an instrument waste line is tied to a drain, contact your local
wastewater treatment center to obtain approval for drain disposal.
Labs need vendors and their representatives, they play a vital role making sure the department can provide quality patient testing and care. Be sure these valuable team members understand your operations, and provide lab safety training in order to prevent injuries or even lab-acquired infections. Ask questions, and communicate with the vendor to ensure that all lab safety procedures are being followed and that safety regulations are not violated. Keeping that eye on safety when dealing with vendors will help to ensure that the important relationships created with them will last.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
This generation is very new to the workforce. In fact, the majority has not had a job yet as they are all eighteen and younger at the time of this writing. However, it is important to know how to adapt to this generation as they are starting to enter the workforce and many people communicate with this generation daily on a personal level.
This generation experiences a tremendous amount of uncertainty in their early lives. From the economic downturn in the late 2000s and school and concert shootings, this generation cares about security. This security is important on both a physical but also on a professional level; they want to make sure that they have professional stability. They care about making a difference, but not to the extent of Generation Y, the Millennial Generation.
There is some concern about this generation’s ability to connect with people on a long-term social level, mainly due to technological and social media advances. However, they do have a preference for face-to-face communication, so even if they do not come with that skill to the workplace, they can learn and adapt to it. Additionally, they are competitive and good multitaskers. They also have an entrepreneurial and independent spirit; they want to be in charge of their own projects and start their own companies. They are also looking into different ways to get their education that do not involve higher education and student debt. They are an imaginative generation with an intellectual curiosity.
Generation Z is the most diverse and open-minded generation, which means that they bring a plethora of ideas, background, concepts, and experiences. Leaders can utilize their diverse base to foster diversity of thought, practice, and skills at organizations. Including this generation as interns and entry-level workers is a good start to begin the process of mentoring this generation while learning from everything they bring to the organizational table.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
Last
month we discussed the rules and requirements for how to properly perform
proficiency testing (PT) within your laboratory. In part 2 of this 3-part
series we’ll review the rules associated with evaluating your results, and how
to investigate any unsuccessful surveys. Still to come in part 3 we will look
into how to utilize your PT results to monitor for trends and shifts in your
values.
The
rules:
Performance Review: Laboratories must initiate and document a review of their PT performance evaluations within 2 weeks of notification that results are available. This includes a review of both graded and non-graded/educational analytes and events as well.
Key
things to note: Even though educational samples are not formally graded, you
should still verify the accuracy of your results, with appropriate follow-up
for any failures. CAP specifically requires you to evaluate these educational
challenges as well. Whether the sample is graded or not does not change the
fact that you had an incorrect result.
Unsatisfactory Performance: For any unsatisfactory results,
you are required to perform a root cause analysis to determine why (see below
for guidance). This also includes any clerical errors – you need to evaluate
your process and find ways to prevent these simple errors from happening again.
If they are happening with PT samples, it is possible they are happening with
patient samples as well.
Cessation of Patient Testing: Unsatisfactory events indicate
that there was a problem with that particular survey; whereas unsuccessful events indicate
there has been a pattern of unsatisfactory events/samples and a larger problem
exists. If a pattern of poor performance is detected, you may be asked by your
local state department of health to cease all testing for a particular analyte.
Key
things to note: This also applies to clerical errors. Even if there was no
technical problem with the accuracy of your results, failure to submit results
on time or clerical errors made while submitting can also have severe impacts
on your ability to continue offering that test.
Remedial Action: If you’ve been notified by your
PT provider or state DOH to cease testing, there are extensive steps that must be
completed to prove that the problem was correctly identified and corrected. You
must also identify where samples will be referred to for tests you are unable
to perform in-house.
Key
things to note: If testing has been removed from your laboratory, you will be
required to demonstrate successful performance in 2 consecutive PT survey
events for the analyte(s) in question before being granted permission to resume
patient testing. This can cause significant delays and financial impact for
your organization.
Root Cause Analysis: Investigate to determine who,
what, why, when, and how the event occurred. Be sure to evaluate all phases of
testing to ensure you identify all potential causes.
Pre-Examination:
Human Resources – evaluate the training and competency records for staff involved in the handling and testing of samples.
Facilities – reagent inventory control & storage temperatures, equipment maintenance and function checks
Standard Operating Procedures (SOPs) – staff compliance with written policies, bench excerpts are current and valid, document version control up to date
Specimen –test requisition/order entry (was the correct test code ordered/performed?), labeling (were aliquot/pour off tubes properly labeled?), transport (was appropriate temperature requirements maintained until testing performed), quality (was there visible deterioration with the sample prior to testing or cracked/damaged tubes received?), quantity (was the original sample spilled or leaking causing an incomplete aspiration of sample by your instrument?)
Examination:
Method
Validations – were instruments current with calibration requirements, any bias
noted during instrument correlation studies, values being reported within the
verified AMR
Environmental
Controls – temperatures/humidity within tolerance limits, for light sensitive
studies (bilirubin) was there excessive exposure of the samples to light prior
to testing, excessive vibrations occurring that may have affected results
(nearby construction or a running centrifuge on a shared work bench)
Quality
Control – did QC pass on the day of testing, was QC trending or shifts noted
that month
Analytical
Records (worksheets) – were sample results transcribed correctly between the
analyzer and worksheet, between the worksheet and LIS
Instrument
Errors – were any corrective actions or problems noted for the days before,
during, or immediately after testing of PT occurred
Testing
Delay, Testing Errors – were samples prepared and not tested immediately
leaving them exposed to light or air which may affect results (blood gas
samples), any errors or problems noted during testing that may have caused a
delay or affected accuracy of results
Post-Examination:
Data
& Results Review – check for clerical errors, was data trasmitted correctly
from the instrument into LIS, was data entered correctly on your PT provider
entry submission forms
Verification
of Transmission – did your results correctly upload to the PT provider website,
was there an error or failure with submission
Review
of LIS – are your autoverification rules set up correctly, is the
autoverification validation current with no known issues
Patient
Impact – perhaps
the most important step to take when reviewing PT failures, you need to
determine what impact your failure had on your patient results. Depending upon
the identified root cause and how different your values were from the intended
response, this can potentially pose a severe impact on your patient values
tested at the same time as the PT samples.
Involve
your medical director to determine if the discrepancy in results is clinically
significant. Perform a patient look-back to review patient values for the same
analyte with the failure during the time period in question. Evaluate the bias
that was present, and if deemed to be clinically significant then corrected
patient reports will need to be issued with a letter from the medical director
explaining why. If it was decided that the discrepancy is not clinically
significant, document this in writing and keep on record with your complete
investigation response.
Corrective Actions/Preventative
Actions– use the following set of questions to help guide you
in ensuring that the problem identified during your root cause analysis will
not occur again:
What
changes to policies, procedures, and/or processes will you implement to ensure
there will not be a repeat of this problem?
Do
any processes need to be simplified or standardized?
Is
additional training or competency assessment needed? If so, identify specific
team members to be trained, and who will be accountable for performing and
documenting this training.
Is
additional supervisory oversight needed for a particular area or step?
Are
current staffing levels adequate to handle testing volumes?
Would
revision or additional verification of the LIS rules address or prevent this
problem?
How
can the communication between laboratory, nursing, and medical staff be
improved to reduce errors in the future?
Continuous Process
Improvement –
after identifying the true root cause(s) for the failure and implementing corrective/preventative
actions, you need to evaluate the effectiveness of those improvements. Have
they been sustained? Are they working to correct the original problem? Have you
created new problems by changing the previous process?
Quality
Management Meetings – if necessary, increase the frequency of these meetings
during the evaluation period for timely feedback to management and staff
Implement
internal audits and quality indicators to check for potential issues
Access
the specimen transport conditions to ensure they meet test requirements
Evaluate
and monitor your turnaround time metrics to track problem specimens and impact
of testing delays
If
necessary, increase the frequency when QC is performed or calibration frequency
if stability issues are identified
Performing
a thorough root cause analysis for any failures will allow you to implement
appropriate corrective actions that will address the true issues. Having a
robust quality management program will help ensure these issues are identified
and corrected in a timely manner, and reduce the potential for the dreaded
Cessation of Patient Testing letter from your local DOH.
Coming
up in the final installment of this series on PT testing, we’ll review all of
the quality indicators and data that can be found in your PT evaluation reports
to help ensure you’re on track for accurate patient values.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018
Top 5 in the 40 Under Forty recognition program. She has worked in the
medical laboratory profession for over 18 years. In her current
position, she transitions between performing laboratory audits across
the entire Northwell Health System on Long Island, NY, consulting for
at-risk laboratories outside of Northwell Health, bringing laboratories
up to regulatory standards, and acting as supervisor and mentor in labs
with management gaps.
Outside the city of New Bern, in Craven County, North
Carolina, there is a particular system for residents to dispose of their
garbage. Locals must go to the nearest participating gas station and purchase
stickers which cost about $2.00 each. These stickers must be placed on each bag
of garbage generated in the household, otherwise they will not be picked up
during the weekly trash collection. In order to save money, a group of widows
has formed a club in which members scout out the open dumpsters in town
(usually behind stores or gas stations). Then they call and let group members
know where they can covertly dump their trash for free that week.
This story may seem funny, but for the most part, it is
true. I have no doubt this also occurs in other parts of the country where the
system for trash collection is similar. Why do people behave this way? Are they
purposely trying to circumvent the trash collection system in place or is the
system just not easy for locals to utilize? If you’re having difficulty getting
people to change safety behaviors (like PPE compliance) in your laboratory, you
might need to determine that for the systems you have in place and ask similar
questions.
In one laboratory the manager struggles with staff who work
part of the day in a clean office and another part in the lab itself. When the
employees go into the lab for brief periods, they often fail to don their PPE.
Upon further investigation, you would learn that staff are not allowed to keep
their lab coats on their chairs and that all PPE is kept in one lab store room
located on the opposite side away from the offices. The system is set up to reinforce
PPE non-compliance.
In another lab the manager placed a permanently-mounted
counter face shield in the chemistry department so that staff would be forced
to use it when popping specimen caps. Staff loaded instrument racks behind the
shield, but when they carried the racks over to the analyzers, their faces were
not protected from splashing. Exposures continued to occur. Here the system is
at play again. A face shield was put in place to change behaviors, but it was
only a partial solution. In order to protect staff fully here, they would need
goggles or a face shield that can be worn. Offer light-weight reusable or
disposable face protection that staff can use easily. Be sure to give them a
say in whatever option is chosen.
Sometimes the system issues are not apparent until there is
a safety event, and unfortunately, that can result in bigger problems. If your
training program does not include regular fire safety training, a small fire
situation may get out of hand quickly. Does your staff have experience handling
a fire extinguisher? Would they easily be able to put out a fire? Do they know
their evacuation routes and meeting places, and could they get there with ease?
What about the lab emergency management plan? Have staff participated in a
table-top drill so they have a basic understanding of how to respond during a
chaotic disaster? These are examples of some safety systems that need to be in
place to keep staff ready and safe at all times.
When people take shortcuts or find ways to circumvent the system, there is usually a pretty good reason, Often, it is the design of the system. In New Bern, elderly women can’t lift large heavy trash bags, so they use smaller bags. They don’t want to pay the same price for a garbage bag sticker that others are paying for big bags. There’s a problem with the system- and those ladies found a way around it. What problems do you see in your lab safety system? If you don’t know what they are, ask around. Staff will talk. It’s better to find out what the workarounds are now and to fix them before an injury or exposure occurs.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years
experience as a certified medical technologist. Today he is the
Laboratory Safety Officer for Sentara Healthcare, a system of seven
hospitals and over 20 laboratories and draw sites in the Tidewater area
of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Generation Y is coming and they are coming in strong! It is
fast becoming the world’s largest working generation and their impact on the
workforce will become even clearer in the next few years. These digital natives
find communication natural, in any shape or forms it comes. They prefer texting
and instant messaging, but also appreciate face-to-face meetings and
hand-written notes. They use social media for both personal and professional
use and consider it essential to know how and where to access information.
Instant gratification has become one of this generation’s key values, because
they grew up with the world of information at their fingertips. They value
professional development and feedback and they are at work to learn and grow.
When working with a Millennial the first step is to show
them that you respect them and what they bring to the table. This generation
has received more negative attention than other generations, but they have a
tremendous amount to offer to the workplace (as do all the other generations).
They value collaboration and learning opportunities, so they are typically
quick to adjust when giving constructive feedback. Because of their
collaborative approach, they value inclusion and Social Media to bring people
together. They are well versed in finding information and can typically solve
smaller technological issues without any help.
This generation is focused on having their work mean
something, to have a purpose that is larger than simply getting a paycheck.
They dislike long email and voicemails and anything that is a waste of paper.
They appreciate flexibility and sending documents electronically. They
experiences high academic pressures, so they are comfortable working in a
fast-paced environment. They are comfortable multitasking and handling multiple
projects simultaneously.
Millennials who work in larger organizations are on the
brink of entering leadership positions. However, there are many self-starters
who have had to learn leadership skills along the way. Because this generation
values collaboration, leaders tend to encourage group work and giving people an
acknowledgement for trying. They dislike people who are afraid or do not want
to learn new technology and cynicism as they are a generally very positive
generation.
When working with Millennials, note that they respond well to a participation work environment so ask for their input and suggestions. Be open about any processes, systems, and share information freely. Provide them with lots of feedback to help them learn and grow. Millennials respond well to a faster pace work environment, so do not try to slow them down. They dislike formality and stiffness, so allow flexibility whenever possible. For example, invite them to provide input for their own goals and do not hover over them. Give them multiple things to work on simultaneously so that they can go from project to project when their energy shifts. This generation is crucial to bring your organization to the next level, so mentor them, help them grow and develop and you get their dedication, passion, collaboration, and positivity in return.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
What’s the purpose? That’s the question that most Gen Ys, or
commonly known as Millennials, ask of their job. Why am I here? Can I make a
difference in the world if I remain doing what I am doing?
The Baby Boomers worked because they felt an obligation to
put in a hard day’s work whether they liked doing what they were doing or not. It
was a job. The Generation Xers introduced a focus on work-life balance, which
was not the case for the Baby Boomer. The Boomers never heard of the concept of
“work-life balance” until their children, the Gen Xers, made it a job
requirement and reality.
As for the Millennials, they need to really believe in their
job and what they are doing. Millennials ask questions that the Boomers and Gen
Xers wouldn’t think of asking. This is often misinterpreted as being lazy or
looking for the easy way out. This is not the case. The Millennials took the
best of their predecessors. Most Millennials have a good work ethic and they definitely
look for balance. However, they’re also searching for a purpose.
My favorite story of a Millennial is centered on the importance of taking lunch at work. This topic surfaced from a Roundtable Discussion with laboratory professionals last October 2018, at the ASCP Annual Meeting in Baltimore. The actual topic for this Roundtable Discussion was “diversity.” However, that quickly changed when the nine people at the Roundtable focused on generational differences. This roundtable was rich in generational diversity. The table was comprised of Boomers, Gen Xers and Millennials. Boomers stated that they found it both necessary and easy to work through lunch. Why? It’s because they pride themselves in their incredible work ethic. The Boomers praised themselves for being better than “most Millennials” who often don’t and won’t work through lunch. Instead of that mindset, perhaps the better approach would be “What can we learn from Millennials in the work place?” That answer is “purpose and balance.”
-Catherine Stakenas, MA, is the Senior Director of Organizational
Leadership and Development and Performance Management at ASCP. She is
certified in the use and interpretation of 28 self-assessment
instruments and has designed and taught masters and doctoral level
students.
Every
laboratory knows that they must participate in proficiency testing (PT) for all
of the regulated analytes they report. But did you know that there is more to
it than simply checking your overall score in each survey you participate in?
Whether you utilize samples from the CAP, API, or have developed your own
in-house blind sample testing algorithm, there is a lot of data available to
help you assess the quality of your laboratory program. In the first of this 3-part
series, we’ll review why PT testing is important and the rules that must be
followed. In part 2 we’ll discuss how to properly perform an investigation when
scores are <100%. Lastly, in part 3 we’ll look at how to review your results
so that you get the most out of them for a successful quality laboratory.
Why
participate? Well frankly, because you have to. It is a CLIA/CMS requirement,
and if your lab has additional accreditations, those agencies will have their
own rules and requirements as well (we’ll get to the rules in a little bit).
But outside of the regulations stating you must
participate; all labs should want to
participate. It’s an opportunity to check your accuracy against peers who are
using the same instrumentation as you. Similar to utilizing an affiliated QC
report, this is a way to see what the “real” value is supposed to be (despite
what a manufacturer may claim it to be), and how close/far off your lab is to
that true value. It can help you identify potential problems before they become
huge problems with patient values being affected, and it’s also a great way to
satisfy competency requirements for your staff.
The
rules:
Participation: For every regulated analyte being tested under your laboratory permit1, you must participate in a CMS-approved PT program2.
Key things to note: This only applies to testing performed using non-waived methodologies. Waived testing is exempt from PT requirements; although it is still recommended that participation occur if an evaluation program is available. Additionally, this only applies to your primary instrumentation. For example, if you have an automated urinalysis reader and your backup methodology is to read dipsticks manually, you are only required to participate in PT for the primary methodology. (Your backup method would then be evaluated for accuracy through semi-annual correlation studies.)
Routine
Analysis:
Unless otherwise instructed by the provider of your PT samples, PT samples are
to be treated the same as patient samples. Meaning they are handled, prepared,
processed, examined, tested and reported the same way you would perform patient
testing; AND by the same staff who would handle patient testing.
Key
things to note: If nursing staff perform a particular test within their unit
(for example, ACT testing in the cardiac cath lab), it is those nursing staff
members who must run the PT samples. You cannot have the laboratory perform PT
testing unless the laboratory also performs the patient testing. Additionally,
PT samples should be rotated among all staff members who perform patient
testing. Meaning all shifts, and all days of the week that the test is
performed – don’t let the day shift get all the fun.
Repeated
Analysis:
Similar to rule #2, unless you routinely perform duplicate testing on your
patient samples, you cannot perform duplicate or repeat testing on your
PT samples. You cannot run a PT sample in duplicate “just to make sure.” Patient
samples are just as important to be accurate as a PT sample, which is why we
participate in a PT program in the first place.
Key
things to note: After the date that laboratories are required to report results
back to the PT provider, you are then allowed to use the samples for repeat
testing. This can be used to check for uniformity in grading of reactions among
staff members, and to assess annual competency. But only after the submission date has passed.
Interlaboratory
Communication:
You cannot discuss the results or samples from a PT survey with any other
laboratory (or Facebook user group) until after
the results submission deadline has passed. Doing so before that time would be
considered cheating. The point of PT testing is not to see how good your
networking skills are, but to ensure accuracy of your own results. Plus, the
other lab may not be as good as you think they are.
Key
things to note: If your laboratory is part of a larger integrated health
system, be careful that you have separate designated staff assigned to enter
results from each location. Entering results for more than one permit number by
the same person would be considered a violation of the interlaboratory
communication rule as they could compare results from Lab A to Lab B prior to
submitting. Also, be mindful of what you put on social media. User groups are a
great networking resource and learning tool, but you still need to follow the
rules. Violating them in a public arena such as Facebook for all the world to
see would put yourself and your organization in great jeopardy if you were
caught.
Referral
of Samples:
You are not permitted to forward or share your PT samples with any other
laboratory until after the
result submission deadline has passed. Similarly, if your laboratory has
received PT samples from another lab, state regulations may require you to
notify your local Department of Health to inform them of the violation.
Key
things to note: The intended purpose of performing PT testing is to verify the
accuracy of your own laboratory testing. If you would routinely send a positive
sample to a reference lab for additional confirmation testing, you would not do
so in this case. Simply report out the values for the tests that your
laboratory performs only. The reference laboratory will have their own PT
samples to check accuracy for the confirmation testing they perform for you.
Ensure your testing menu is up to date and accurate so that your PT provider is
not expecting values for a confirmatory test if you do not physically perform
it in-house.
Records
Retention:
Ensure that all records and documents related to the testing of PT samples are
saved for the amount of time required by your regulatory agencies (typically
2-5 years). This includes instrument print outs, LIS chart copies of the filed
results, QC records for the day of testing, and any associated worksheets used
to document your results.
Key
things to note: Retaining a copy of the instrument maintenance logs and QC
records along with the actual PT results will help you investigate any scores
that are less than 100%.
Attestation: Both the laboratory director and
all personnel performing testing must sign the included attestation statement.
This is not just a way to track who performed the test, but is a legal binding
document assuring that testing was carried out appropriately as per the rules
defined above.
The penalties
for labs that are caught violating the rules (whether intentionally or not) can
be quite severe. These penalties can include the revocation of your CLIA
permit; a ban for the laboratory owner and laboratory director; as well as
possible financial penalties and fines.
Coming
up in the next blog we’ll review the rest of the rules related to evaluation of
your scored PT results, and how to perform a thorough investigation into any
unsuccessful survey events.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018
Top 5 in the 40 Under Forty recognition program. She has worked in the
medical laboratory profession for over 18 years. In her current
position, she transitions between performing laboratory audits across
the entire Northwell Health System on Long Island, NY, consulting for
at-risk laboratories outside of Northwell Health, bringing laboratories
up to regulatory standards, and acting as supervisor and mentor in labs
with management gaps.