Emergency services were called to a fire in a small apartment building, in which the structure was completely engulfed. Most of the occupants had been evacuated – however, once the fire was extinguished, the charred remains of an adult woman were found in the debris.
At the autopsy of severely fire-damaged human remains, two key questions must be answered: 1) who is the decedent?, and 2) were they alive when the fire started?
Question #1 is particularly relevant in this case, as many people lived in the building. Presumptive identification based on the tenant list may seem reasonable at first, but this victim could represent a visitor, contractor, or subletter. When facial identification isn’t possible, radiographic identification can be done with dental x-rays or x-rays of other bones which may have unique features from healed trauma or degeneration. Additional methods of positive identification could include fingerprints (if still intact), or DNA comparison to first degree relatives.
Question #2 is of importance because fire can be used in an attempt to disguise the identity of a victim of violent crime and destroy evidence. Cutaneous evidence of trauma may be disguised by burns, so full body x-rays are taken of every fire-damaged body. X-rays can also reveal retained bullets, knife tips, or fractures unlikely to have been caused by the fire.
When deciding if a fire victim was alive when the fire started, we first examine the upper and lower airways for soot. Most fire victims do not die from cutaneous burns, but from smoke inhalation – including carbon monoxide (CO) toxicity, which is often apparent by cherry red discoloration of the blood and viscera. Postmortem carboxyhemoglobin measurements in house fire victims are typically greater than 50%. There are exceptions to this rule, of course. Rarely, someone who was clearly alive when the fire began will have minimal or no soot in their airways and a negligible carbon monoxide concentration. This can happen in a “flash fire”, such as one ignited by gasoline or oxygen tanks, in which thermal injury to the upper airway may cause rapid occlusion by laryngospasm or edema. People with underlying heart or lung conditions will be more susceptible to the effects of carboxyhemoglobin, and may not survive long enough to obtain a level above 50%. Fires also produce other toxic products of combustion such as cyanide, and can lower ambient oxygen saturations to result in asphyxiation by lack of ambient oxygen (even without CO).
Forensic pathologists need to be aware of the artifacts that fires can create. Pugilistic posturing of fire victims (limb flexion) is due to heat-related contraction of muscle fibers. Epidural hematomas can result from boiling blood and bone marrow within the calvarium extravasating into the epidural space. The heat can induce fractures in exposed bone once the surrounding soft tissue is consumed or fully charred. Finally, the heat can split apart skin and soft tissue, resulting in sharp-force-like defects which occur parallel to the orientation of muscle fibers (rather than across them, which is more suspicious for penetrating trauma).
Of utmost importance in fire-related deaths, however, is scene investigation. The manner of death in fire fatalities is related to the origin of the fire. Most fire deaths are accidental, as the fire is unintentionally sparked by some electrical malfunction or unattended flame. However if the fire started intentionally, the manner of death can be homicide (if started by another) or suicide (started by the victim). It is therefore crucial to review the final fire investigation report before finalizing the autopsy report and death certificate.
This image shows dark black soot lining the main and lobar bronchi; this indicates the victim was breathing during the fire.Heat-related epidural hematomas have a brown, amorphous appearance rather than the bright red color of traumatic epidural hematomas.The scalp has been consumed by fire, and the exposed bone is calcined and brittle with fractures of the outer table.
-Alison Krywanczyk, MD, FASCP, is currently a Deputy Medical Examiner at the Cuyahoga County Medical Examiner’s Office.
Microbiology Case: Lung nodules in a patient undergoing lung transplant evaluation
Case History
A 71-year-old male with a past medical history of severe interstitial lung disease (ILD) presented for lung transplant evaluation. His chest CT demonstrated findings consistent with his known diagnosis of ILD, along with a 3.6 cm focal nodular calcific density near the right costophrenic angle, and additional scattered calcified lung nodules measuring up to 3 mm. Sputum cultures were obtained to evaluate the CT findings.
Laboratory Identification
Routine bacterial, fungal, and AFB sputum testing was performed. No AFB were recovered, and a mixture of bacteria consistent with oral flora were found on blood, chocolate and MacConkey agars. The fungal culture grew a moderate amount of round, non-hyphenated yeast which were encapsulated, urease-positive and reacted with caffeic acid (Image 1A and 1B) consistent with Cryptococcus species. The organism was definitively identified as Cryptococcus gattii by MALDI-TOF mass spectrometry, which was subsequently confirmed by growth and the appearance of a deep blue color on Canavanine Glycine Bromothymol Blue (CGB) agar (Image 1C). The patient was prescribed daily fluconazole to take daily for 6 months, and underwent a successful bilateral transplant two months after treatment initiation.
Image 1. A) Urease testing of the patient’s yeast (left, positive) versus Candida albicans (right, negative) consistent with Cryptococcus sp. B) Caffeic acid testing of the patient’s yeast (left, positive) versus C. albicans (right, negative) consistent with Cryptococcus sp. C) Growth of the patient’s isolate (left) versus Cryptococcus neoformans (right) on Canavanine Glycine Bromothymol Blue (CBG) agar. The deep blue color produced by the patient’s isolate is indicative of Cryptococcus gattii.
Discussion
Cryptococci are important pathogens of both immunocompetent and immunocompromised hosts. While Cryptococcus neoformans causes most human cryptococcal disease, Cryptococcus gattii is also a clinically important cause of infections. Though genetically similar, these two species exhibit important differences with respect to ecological niche, pathogenesis, and epidemiology. Historically, trees (specifically eucalyptis) have been identified as environmental reservoirs of C. gattii, while C. neoformans is associated with pigeon guano.1Cryptococcus neoformans has a worldwide distrubtion, while C. gattii is thought to be geographically restricted to Australia, Western Canada and the Pacific Northwest of the United States, although this has become less clear in recent years. Indeed, the patient in this case had not traveled to any of these locales; instead, he is from the southeastern United States, where the organism may be endemic.3
There is an established association between C. gattii and infections in immunocompetent hosts, and recent evidence points to genetic and immunological factors which predispose some individuals to C. gattii infection. Possible differences in clinical course and patient outcomes have been suggested to justify differentiation between C. gattii and C. neoformans in laboratory settings. Importantly, routine laboratory methods such as commercial biochemical identification systems, morphological observations, and cryptococcal antigen testing lack the discriminatory power to distinguish these species.2 By contrast, MALDI-TOF MS and molecular methods, including some molecular panels performed on positive blood culture bottles, are able to discriminate between C. gattii and C. neoformans. The use of glycine as a sole carbon and nitrogen source in the presence of canavanine allows biochemical differentiaton through the use of CGB agar. The degredtation of L-canavanine to ammonia in the presence of glycine by C. gattii raises the pH and results in associated color change, while C. neoformans remains a yellow or green color (Image 1C). While robust, this incubation can take up to five days resulting in prolonged turn around times.2
Cryptococal infection begins through inhalation of the organism into the lungs, where the yeast then can dissemisate to other anatomical sites. When compared to C. neoformans, C. gattii is less likely to present with central nervous system (CNS) involvement but exhibts a higher incidence of imaging abnormalities and mass lesions. In pulmonary settings, C. neoformans infections commonly present with infiltrates while C. gattii infections are nodular2 as seen in this case.Irrespective of the species involved, cryptococcal infections can be asymptomatic or classically present as a meningoencephalitis, chronic or acute pneumonia, or in a number of cutaneous manifestations. Fluconazole is the drug of choice for management of asymptomatic or mild to moderate pulmonary infections. Despite the removal of the infected lungs, it was determined that the patient should complete the entire six month course of fluconazole due to his immunosuppression post-transplant.
References
Beardsley, J., Dao, A., Keighley, C., Garnham, K., Halliday, C., Chen, S. C.-A., and Sorrell, T.C. What’s New in Cryptococcus gattii: From Bench to Bedside and Beyond. J. Fungi. 2023; 9, 41:1-16.
Lockhart, S., Roe, C. C., and Engelthaler, D.M. Whole-Genome Analysis of Cryptococcus gattii, Southeastern United States. Emerg. Infect. Dis. 2016 Jun; 22(6): 1098-1101.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
-Francesca Lee, MD, is an associate professor in the Departments of Pathology and Internal Medicine (Infectious Diseases) at UT Southwestern Medical Center
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
Working in a cancer center, our cytologists are well-versed in cancer morphology being able to diagnosis primary malignancies, distant metastases, and even combined metastatic disease in the same lymph node. What we don’t see as often as community hospitals are infectious diseases. However, we do have many immunocompromised patients at our institution, so the rare opportunistic infection does occur. And boy, do we get excited to pass the case around! Please find a series of infectious events embedded within this post. And unfortunately, we do not live in an area where coccidiomycosis is endemic, so beyond school, we haven’t had the pleasure of identifying those in our daily work.
Case 1. Lung, Bilateral, BAL (Bronchoalveolar Lavage)
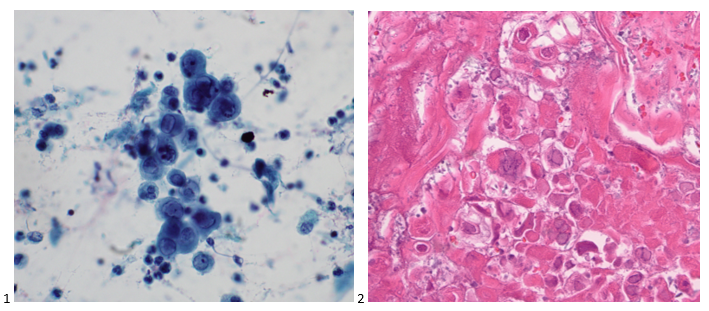
A 73-year-old male patient was admitted to the ICU with pneumonia. The pulmonologist performed a bilateral bronchoalveolar lavage (BAL) to rule out pneumocystis pneumonia. We prepared a pap-stained smear, two cytospins, a SurePath liquid based prep, and a cell block. Two additional cytospins were sent to histology for GMS staining. While no malignant cells were identified, fragments of squamous epithelium with acute inflammation and necrosis were present. Multiple viral inclusions were identified, appearing as ground glass within the nuclei. (Image 1). These cells present with classic 3 M features: molding, multinucleation, & margination of chromatin. The cell block also highlights viral inclusions, but demonstrates pseudohyphae and spores associated with surrounding squamous cells as well (Image 2).
Diagnosis: Herpes Simplex Virus (HSV) and Candida.
Case 2. Lung, Left Lower Lobe, CT-guided FNA
A 72-year old male with stage IIA squamous cell carcinoma underwent a VATS right upper lobectomy and mediastinal lymph node dissection. He completed adjuvant carboplatin/gemcitabine therapy. On a surveillance CT scan, the treated area demonstrated progression as well as multiple bilateral lung nodules. To determine whether the new left lower lobe superior segment lung nodule was a metastasis or new primary, a CT-guided biopsy was performed. The smears and cell block sections were negative for malignancy but demonstrated inflammatory cells and necrotic debris, consistent with a necrotizing inflammatory process (Images 3-5). A separate pass was sent for microbiological cultures to correlate our findings. The following day, Kinyoun and GMS stains were performed on paraffin-embedded sections of the cell block. No fungal organisms were identified on GMS, but acid-fast bacilli were noted by the cytologist on the Kinyoun-stained section (Image 6).
Diagnosis: Acid-fast bacilli (AFB), consistent with Mycobacterium Avium Complex. Isolated and confirmed by microbiology.
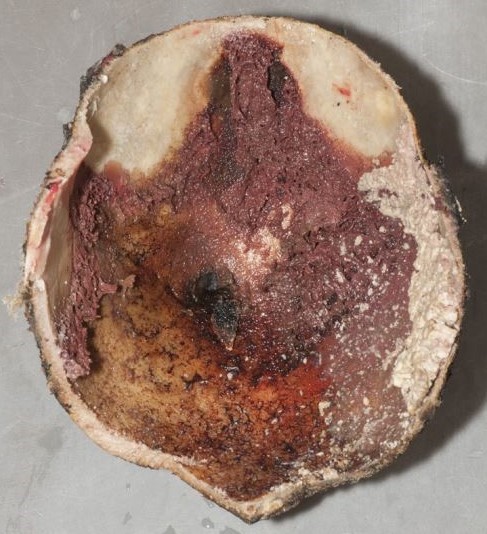
Case 3. Lung, Right Upper Lobe, CT-guided FNA
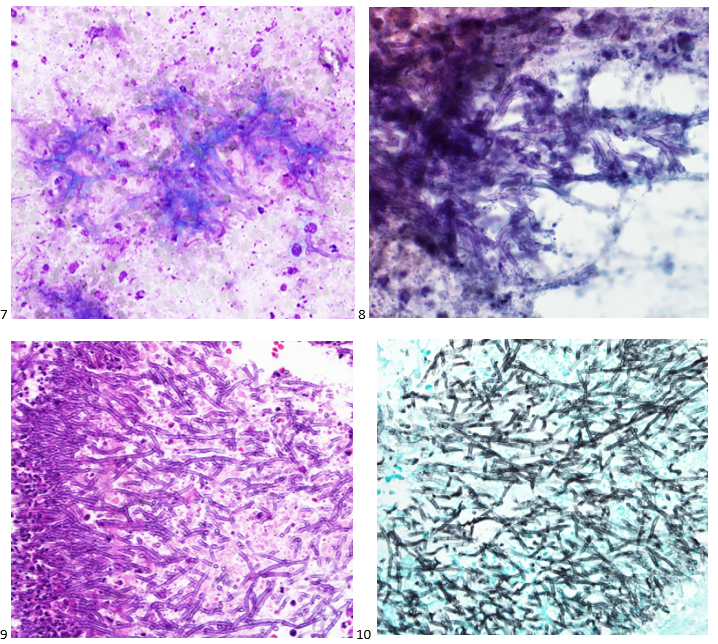
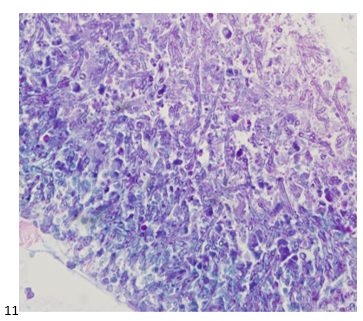
A 58-year-old male presented with multiple lung nodules and a brain mass. We reviewed the brain mass excision from an outside institution and agreed with the original diagnosis of anaplastic oligodendroglioma, WHO grade III with a Ki-67 proliferation index that approached 20%. EGFR was not amplified (ratio 1.2), but 1p/q19 co-deletions were noted in greater than 75% of tumor cells. To rule out primary versus metastatic disease, the patient had a CT scan-guided biopsy of right upper lobe lung mass. No malignant cells were identified in the sample; however, necrotic debris and abundant fungal hyphae were noted (Images 7-9). A portion of the sample was sent to Microbiology for culture. The following day, a GMS and PAS stains were performed on paraffin-embedded sections of the cell block which demonstrated the same fungal hyphae seen in the smears and cell block preparations (Images 10 & 11).
Diagnosis: Abundant fungal hyphae, consistent with Aspergillus
Case 4. Left Hilum, EBUS-FNA
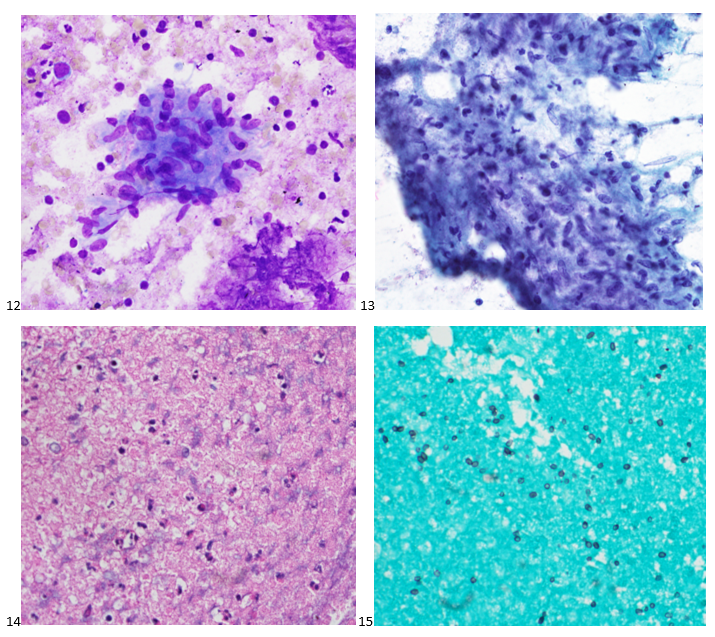
A 20-year-old female patient presented with patches, pain, and inflammation on her legs, and she was diagnosed with erythema nodosum. When her swelling and pain worsened, a chest X-ray demonstrated a left hilar mass, and a subsequent CT demonstrated the mass to be encircling the left superior pulmonary artery and obstructing the pulmonary vein along with multiple peribronchial ground-glass opacities and hilar lymphadenopathy. The concern from the referring physician was thymoma versus lymphoma given her age and clinical presentation. The patient underwent an endobronchial ultrasound to assess the hilar mass and lymphadenopathy. The lymph node aspirates appeared benign, with flow cytometry supporting the cytologic diagnosis. On the left hilum FNA, there were aggregates of lymphocytes, plasma cells, and epithelioid histiocytes with caseating necrosis and fibrosis (Image 12-14). Kinyoun, PAS, and GMS stains were performed on paraffin-embedded sections of the cell block. No acid-fast bacilli were identified. Fungal organisms in the form of budding yeast were noted on GMS (Image 15) and PAS stain. The patient was prescribed a 12-week course of antifungal medication.
Diagnosis: Necrotizing inflammation with fungal organisms, suggestive of Histoplasmosis.
Case 5. Lung, Right Middle Lobe, BAL (Bronchoalveolar Lavage)
A 44-year-old male patient with uncontrolled Type II diabetes and hypertension presented to pulmonary after imaging demonstrated diffuse mediastinal and hilar lymphadenopathy. The differential diagnosis was sarcoidosis versus a lymphoproliferative process. An endobronchial ultrasound was performed to evaluate the lymph nodes, all of which came back as reactive. A BAL was performed and sent for cell count, cytology, flow cytometry, and microbiology. Flow cytometry analysis demonstrated a reversed CD4:CD8 ratio, and upon further testing, the patient was determined to have HIV. Eosinophilic froth or casts were identified on the cytopreparations of the BAL (Images 16). GMS and PAS stains were performed with adequate controls, and the PAS was negative for other fungal organisms while the GMS demonstrate positive staining for what we in cytology refer to as cups or crushed ping pong balls (Image 17). He was treated with Bactrim.
Diagnosis: No malignant cells identified. Positive for Pneumocystis jirovecii.
Case 6. Lung, Right Lower Lobe, CT-guided FNA
A 68-year-old male patient with a history of a renal transplant presented with an endobronchial mass in the left lower lobe that was biopsied and diagnosed as adenocarcinoma at an outside institution. We reviewed the slides in-house and determined the original tumor to be a mucoepidermoid carcinoma. After an unsuccessful staging procedure, a mediastinoscopy was performed, and the mediastinal lymph nodes showed hyalinizing non-necrotizing granulomata, suggesting underlying sarcoidosis. No microorganisms were identified with AFB, GMS, or PAS stains. The patient did not receive adjuvant therapy following the resection of his endobronchial tumor. Seven years later, he presented to the ER for syncope and 30 lbs. weight loss in 5 months. A CT scan was performed demonstrating a thick-walled cavitary lung mass in the right lower lobe. The patient was referred to radiology for a CT-guided FNA of the RLL mass. Fibrous tissue and abundant microorganisms with a polysaccharide capsule were identified on both FNA and core biopsy (Images 18-20). The PAS, GMS, Mucicarmine (Image 21), and Fontana Masson special stains were performed on cell block sections, with proper controls, highlighting abundant microorganisms. The patient was prescribed an antifungal for his cryptococcoma (cryptococcal lung abscess).
Diagnosis: No malignant cells identified. Abundant microorganisms, morphologically consistent with Cryptococcus species.
If you enjoyed this special series, look out for more in the future! And feel free to recommend or request interesting cases!
-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
An elderly patient with urothelial carcinoma of the bladder was treated with intravesical Bacillus Calmette-Guerin (BCG). The patient presented nearly a year later with back pain and their laboratory tests revealed leukocytosis with neutrophilia. Magnetic Resonance Imaging (MRI) of the back showed findings suspicious for discitis/osteomyelitis of the vertebrae with epidural phegmon/abscess. The abscess fluid was sent for aerobic and anaerobic bacterial, acid-fast bacilli and fungal cultures and empiric intravenous antibiotics was commenced. Gram stain and all cultures were negative.
Their symptoms persisted and a repeat MRI 3 months later demonstrated similar findings. Decompression of the vertebrae was repeated and fluid from the disc space was sent for cultures. Again, Gram stain was negative while no growth was seen on aerobic, anaerobic and fungal cultures. However, about eight weeks after incubation, the Lowenstein-Jensen media showed rough and buff colonies (Figure 1). Matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF) performed on an isolate from the media confirmed the presence of Mycobacterium Tuberculosis Complex (MTBC). MALDI-TOF alone cannot distinguish between species within in the complex and thus, the result was reported as MTBC, with a comment indicating that MTBC includes M. tuberculosis and M. bovis.
Figure 1. Lowenstein-Jensen Medium with buff and rough MTBC colonies.
Upon request, phenotypic antimicrobial susceptibility testing (AST) was performed and it showed susceptibility to all primary anti-mycobacterial drugs including Pyrazinamide (PZA). Also, due to a clinical concern for M. bovis BCG infection, further species-level was required. Therefore, the isolate was sent to the Centers for Disease Prevention and Control (CDC) for species-identification/confirmation and to the State Department of Health for confirmatory AST. Results from the CDC showed M. bovis but the State Department of Health showed PZA susceptibility, inconsistent with M. bovis which is intrinsically resistant to PZA.
Discussion
M. bovis is a part of the MTBC, which includes M. tuberculosis, M. bovis and BCG strain, M. africanum, M. microti, M. orygis, M. canetti, M. caprae, M. pinnipedii, M. suricattae. M. bovis is the main cause of tuberculosis in cattle, deer, and other mammals and compared to M. tuberculosis, is a rare cause of tuberculosis in humans. There were about 59, 273 cases of tuberculosis in the U.S between 2006 and 2013 and 770-948 (1.3-1.6%) of those were due to M. bovis[1]. However, the worldwide burden is thought to be underestimated, especially in regions with considerable consumption of unpasteurized milk.
Risk factors for M. bovis infection include practices. which expose humans to mammals with M. bovis or their products. These practices include livestock farming, veterinary medicine and consumption of unpasteurized milk. Bacillus Calmette-Guérin (BCG) is a live attenuated strain of M. bovis used as tuberculosis vaccine in many areas with relatively high prevalence of tuberculosis. However, it’s also used as adjunctive therapy for non-muscle invasive bladder cancer and unfortunately, this has rarely been complicated by M. bovis BCG infection. There were about 118 cases reported between 2004 and 2015, accounting for approximately 1-5% of patients with intravesical BCG [2]. Some of the risk factors of BCG infection are traumatic catheterization, active cystitis, persistent gross hematuria following transurethral surgery, immunosuppression and age ≥70 years.
M. bovis (and M. bovis BCG) infection is indistinguishable from M. tuberculosis clinically and radiologically. However, there is a higher incidence of extrapulmonary tuberculosis and an increased risk of scrofula -infection of the lymph node(s) in proximity to the mouth and esophagus- and gastrointestinal disease.1 The laboratory workup and findings are also similar. Microscopically, primary specimen smears are screened using auramine-rhodamine stain which is the most sensitive, while carbol-fuchsin (Ziehl-Neelsen or Kinyoun) stain is used to confirm presence of growing acid-fast bacteria. MTBC is slow-growing on culture, requiring at least 7 days to form colonies on solid media. M. bovis colonies appear small and rounded, with irregular edges and a granular surface on egg-based media, and small and flat on agar media.3
MALDI-TOF which is used reliably in the workup of many bacterial infections also can’t differentiate between MTBC species. Where available, biochemical testing can be used to differentiate M. tuberculosis from M. bovis (see table 1). However, this is being replaced by newer modalities especially DNA hybridization or polymerase chain reaction (PCR)-based molecular methods such as the Region of Deletion analysis.
Species level differentiation between M. bovis and M. tuberculosis is extremely important when M. bovis is suspected because the first line drugs for treating M. tuberculosis are Rifampicin, Isoniazide, PZA and Ethambutol, and M. bovis is intrinsically resistant to PZA.1,3 The observation of this mono-resistance pattern on AST of MTBC isolate raises the suspicion for M. bovis and may warrant further workup. Importantly however, M. bovis infection cannot be excluded on the basis of an MTBC AST showing susceptibility to PZA, as this AST is difficult to perform and identifies only about 80% of M. bovis cases and approximately 7% of M. bovis cases are incorrectly reported as PZA susceptible.2 When required, isolates should be sent to a public health laboratory for M. bovis confirmation.
Table 1. Biochemical differences between M. bovis and M. tuberculosis.1
Pfyffer, G. “Mycobacterium: General Characteristics, Laboratory Detection, and Staining Procedures.” In Manual of Clinical Microbiology, Eleventh Edition, pp. 536-569. American Society of Microbiology, 2015.
-Adesola Akinyemi, M.D., MPH, is a fourth year anatomic and clinical pathology resident and Chief resident at University of Chicago (NorthShore Program). He will be undergoing fellowship trainings in cytopathology (Northwell Health, NY) and oncologic surgical pathology (Memorial Sloan Kettering Cancer Center, NY). He is also passionate about health outcomes improvement through systems thinking and design, and other aspects of healthcare management.
Twitter: @AkinyemiDesola
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
An adult patient with no significant past medical history presented to the emergency room one day after arriving from a one-month stay outside of the United States. They had a fever for approximately 10 days. At the ER, their temperature measured over 102 degrees Fahrenheit. They also complained of nausea, cough, and headache. However, they denied abdominal pain, vomiting, neck pain, diarrhea, constipation, or urinary symptoms. The attending physician ordered a urinalysis, viral panel, dengue serology, malarial blood smear, urine culture, and blood culture. The urinalysis was consistent with a UTI and the patient was discharged with ceftriaxone.
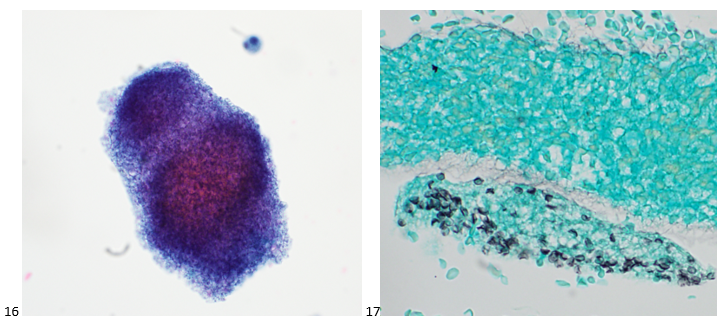
The respiratory viral panel (RSV, Influenza A/B, SARS-CoV-2), malarial blood smear, urine culture, and dengue fever serology came back negative the next day. However, the Gram stain from the blood showed gram negative rods (Image 1) with concurrent bacterial growth on the blood, chocolate, and MacConkey agars. No growth was present on the CNA agar (Image 2).
Image 1. Gram stain from the positive blood culture. Image 2. Plates demonstrating growth of this organism. Note the growth on blood agar, chocolate agar, and MacConkey agar but not CNA agar. The organism is a non-lactose fermenter.
Multiplex PCR from positive blood culture and later MALDI of the pure isolate confirmed the Salmonella organism, which was later serotyped via a Salmonella Rapid Latex Agglutination Test Kit as Salmonella typhi. Susceptibility testing revealed that the organism was susceptible to Ceftriaxone and the patient was treated accordingly.
Discussion
The Salmonella genus is divided into two species: Salmonella bongori and Salmonella enterica. The Salmonella species can be further divided into the following subspecies: enterica (group I), salamae (group II), arizonae (group IIIa), diarizonae (group IIIb), houtenae (group IV), indica (group VI). To complicate matters more, these subspecies may be further classified based on their serotype.1 Salmonella can be serotyped based on their O, H, and Vi antigens.2 As a whole, the Salmonella enterica sub enterica (group I) are gram negative rods that belong to the Enterobacteriales family. They are highly motile, facultative anaerobes that produce H2S and do not ferment lactose. We will be primarily focusing on the non-typhoidal Salmonella and typhoidal Salmonella subspecies.
The non-typhoidal Salmonella organism resides within the enteric tracts of humans and animals. They primarily cause infection via the feco-oral route via contaminated poultry, eggs, and meat products. These organisms are very sensitive to stomach acid; therefore, an abundant inoculation must take place within the gastrointestinal tract. The mucosa is invaded and becomes inflamed. The subsequent increase in prostaglandins and cAMP cause the patient to experience loose diarrhea.2 Shallow ulcerations may be present on histology. Non-typhoidal Salmonella most commonly causes gastroenteritis consisting of bloody diarrhea, fever, vomiting, and abdominal pain. Bacteremia may occur in approximately 5% of patients. In addition, sickle cell patients are at risk of developing osteomyelitis. The diagnosis is made through a stool culture and most patients can be treated symptomatically, as this is a self-limiting infection.3
On the other hand, typhoidal Salmonella may have a more serious presentation. The typhoidal Salmonella infections are caused by the Typhi and Paratyphi (A, B, or C) serotypes, with the former causing more severe illness. These serotypes reside in humans and are also transmitted via the feco-oral route. The organism reaches the basolateral side of the M cells and spread to the mesenteric lymph nodes and the blood. They also replicate within macrophages and are able to inhibit the fusion of lysosomes with phagosomes.2 Clinically, the patients present with fevers due to the bacteremia, followed by abdominal pain and the characteristic “rose spots” on the second week of infection. If not treated, patients may develop complications such as septic shock, hepatosplenomegaly, or abdominal perforations secondary to necrosis of Peyer’s patches within the GI tract. The infection is diagnosed with blood (40-80%) and stool (30-40%) cultures and must be reported to the state. Patients are parenterally treated with ceftriaxone and may be changed to other susceptible antibiotics if clinically indicated.3
There are two typhoid vaccines available: a live oral vaccine and an inactivated injection. The typhoid vaccine is recommended for certain high risk populations including travelers, those with known contact with typhoid carrier, and some laboratory workers who work routinely with this organism. The vaccine, while beneficial, does not replace proper hand and food hygiene in prevention of typhoid fever.4
References
Achtman, M., Wain, J., Weill, F.-X., Nair, S., Zhou, Z., Sangal, V., Krauland, M. G., Hale, J. L., Harbottle, H., Uesbeck, A., Dougan, G., Harrison, L. H., & Brisse, S. (2012). Multilocus Sequence Typing as a Replacement for Serotyping in Salmonella enterica. PLoSPathogens, 8(6), e1002776. https://doi.org/10.1371/journal.ppat.1002776
Kaplan Medical. (2017). USMLE step 1 lecture notes 2017: Immunology and microbiology. Simon and Schuster.
Spec, A., Escota, G. V., & Chrisler, C. (2019). Comprehensive review of infectious diseases. Elsevier.
-Ximena Wise, MD is an AP/CP pathology resident at the University of Chicago (NorthShore). She is interested in pursuing fellowships in Surgical Pathology and Gynecologic Pathology after completing her residency training.
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
Len began his shift in the hematology department. He liked to use the counter-mounted safety shield when opening specimens because he did not like to wear goggles over his eyeglasses. When it was time to read differential slides, he knew he could not look into the microscope with his glasses on, so he reached up with his gloved hands, grabbed his frames and set them on the dirty hematology workbench next to the scope.
OSHA’s Bloodborne Pathogens Standard was promulgated (put into effect as law) in 1991. Its purpose was to prevent employee exposures to infectious organisms that may be present in blood or body fluids. For those employers covered, that meant creating an Exposure Control Plan, providing certain vaccinations, educating staff about exposure follow-up, and providing personal protective equipment (PPE).
Much has changed in healthcare since 1991, but the standard remains unchanged. Changing an OSHA standard does not happen often, and it does not happen quickly. In many ways, for the Bloodborne Pathogens Standard, that’s a good thing. The same protective measures must be in place in workplaces like laboratories, and despite the appearance of novel pathogens over the last 30 or so years, the basic required risk assessments and mitigation steps still apply.
Some people, however, complain that the standard doesn’t speak clearly enough about issues that have changed over time and that now need to be addressed. Do the regulations speak to personal electronic devices in the lab like smart phones, smart watches, and ear buds? There is mention of not having food or drink in the department, but what about chewing gum or candy? Sometimes you need to dig a bit deeper to discover that those issues are also addressed, even though some of those issues did not exist when the standard was written.
If you read the line, “Eating, drinking, smoking, applying cosmetics or lip balm, and handling contact lenses are prohibited in work areas where there is a reasonable likelihood of occupational exposure,” it seems very clear that OSHA is trying to prevent hand to face contact. While they did not cover every possible action, this likely includes gum chewing and touching cell phones which are then brought to the face (or worse, used at home by a toddler wanting to play). It can be argued that lab employees use telephones often on the job, and that gloved hands are near the face because of that.
So what other actions occur in your lab that could potentially create bloodborne pathogen exposure – actions that may occur every day or so quickly you don’t notice? Have you thought about wireless headsets or speaker phones in the lab? Do you look in cabinets and drawers for food or drink (especially during off-shifts)? Is gum chewing allowed in your lab (hint: if you’re in a CAP-accredited lab this is strictly forbidden)?
And what about poor Len with his glasses? Has anyone trained him to remove his gloves, wash his hands, and place his spectacles on a clean surface before using the microscope? There might be other things you did not notice. If you have an employee with hearing aids, do they remove them to answer the phone? Do some staff wear gloves when opening the lab exit door and others use bare hands? Are computer keyboards used with and without gloves? Is PPE worn into lab rest rooms? These are all instances where a lab-acquired infection could begin, and they happen in a flash. Perform risk assessments to not only locate the risks, but to implement ways to mitigate them. Magicians claim that their hands can move faster than the eye can see in order to work their tricks. Employees will perform “tricks” as well, but the outcomes may not be as entertaining. Providing safety education and observing people at work to see where other risks exist are important steps toward complying with the Bloodborne Pathogens Standard. The regulations are not new, but with updated lab policies and safety measures, they can be powerful tools to protect you and your staff from the new pathogenic threats headed our way.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
An 85 year old female with past medical history of hypertension, hyperlipidemia and past surgical history of cholecystectomy presented to the emergency department (ED) with an abdominal pain in the left upper quadrant, which had been persistent for several days. Her vitals were BP:145/86 mm/Hg; pulse: 86 beats/minute; respiratory: 20/min; Temp: 98.3 °F (36.8 °C); SpO2-98%. Her medical history revealed that she had a diagnostic laparoscopy, common bile duct exploration, and stone extraction nine months ago. Since then, the patient had a chronically draining abdominal sinus for which she underwent diagnostic laparoscopy and multiple benign peritoneal implant biopsies 5 months prior to the current event.
Examination of the LUQ revealed a fluctuant lump in the LUQ, which was close walled with no purulence or drainage. The CT abdomen demonstrated an increased infiltration of the left rectus abdominis, left anterior abdominal wall muscles, and subcutaneous tissues in the upper abdomen, with a suspicion for infectious etiology.
The patient was evaluated by general surgery for abscess at the LUQ. The abscess was drained, the fluid was sent for a bacterial culture, and the patient was started on IV vancomycin and Zosyn. Blood cultures were collected but had no growth. The pathology report of peritoneum implants and soft tissue biopsies showed focal necrotizing granulomatous inflammation but negative special stain for fungi (GMS-F) and acid-fast bacilli (AFB). The Gram stain of her abscess fluid culture was negative with a few neutrophils. However, her culture grew spready colonies on blood and chocolate agar after 4 days of incubation (Figure 1). Since the initial Gram stain was negative, Kinyon stain was performed and was positive (not shown). It was identified by Matrix-assisted laser desorption ionization Time of Flight (MALDI-ToF) as Mycobacterium fortuitum species.
Figure 1. Dry spready colonies on Chocolate agar plate.
Discussion
There has been recent evidence of an increased prevalence of Nontuberculous Mycobacterium (NTM), and it is becoming a major public health concern.1,2 NTM is a diverse group of ubiquitous, environmental, acid-fast organisms that can produce a wide range of diseases, most of which are found in skin and soft tissue infections (SSTI).3 Historically, NTM has been classified into Runyon groups based on the colony morphology, growth rate, and pigmentation.4 Identification is made with rapid molecular diagnostic technology. However, grouping the species of NTM is based on the growth rates and divided into rapidly growing mycobacteria (RGM) and slowly growing mycobacteria (SGM).
RGM includes species that grow on the media plates within 7 days and subdivided into 5 groups based on pigmentation and genetic similarity: Mycobacterium fortuitum, Mycobacterium chelonae/abscessus, Mycobacterium mucogenicum, and Mycobacterium smegmatis. Most SSTIs commonly associated with surgery and cosmetic procedures are caused by 3 RGM species: M fortuitum, M abscessus, and M chelonae. These infections are nonspecific in their clinical presentations and may present with abscesses, cellulitis, nodules, ulcers, panniculitis, draining sinus tracts, folliculitis, papules, and plaques. There is a delay in diagnosis of these infections, as mycobacterial cultures are not routinely performed on surgical wound infections or skin biopsy specimens which are essential for an accurate diagnosis, especially because the treatment varies depending on the species and its sensitivities.5
M. Fortuitum is a Gram positive, acid-fast, aerobic rod-shaped, saprophytic, rapidly growing NTM that is typically considered an opportunistic pathogen. They are widely distributed in the nature and can be isolated from soil, dust, natural surface and municipal water, wild and domestic animals, fish, hospital environment, contaminated medical instruments, and implants. Common culture media include Middlebrook 7H10 or 7H11 agar, BACTEC 12B broth and 5% sheep blood agar or chocolate agar. These organisms may not stain well with the Ziehl-Neelsen or Kinyoun method and may not be recognized readily with the fluorochrome method due to lipid rich long-chain mycolic acids in their cell walls. Because of the high mycolic acid content in the cell wall, it does not stain well by the Gram stain, which is likely the reason for the negative Gram stain results in our patient abscess culture.
It is well known that older biochemical tests are replaced by newer diagnostic methods including matrix associated laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) and molecular methods, including line probe hybridization assays, as well as 16S ribosomal RNA sequencing. DNA line probe assays provide a rapid means of identification and currently there are two commercially available assays: INNO-LiPA MYCOBACTERIA v2 assay (Fujirebio Europe, Ghent, Belgium) and GenoType assay (Hain Lifescience GmbH, Nehren, Germany). However, neither of them is currently FDA-approved, and therefore, the use is largely restricted to the public health or reference laboratories in United States. Studies utilizing these lines probe assays have reported satisfactory sensitivity and specificity.6,7,8,9 Notably, a study by Fida et al., reported a case of Mycobacterium smegmatis that was misidentified as Mycobacterium fortuitum by a DNA line probe assay.
In our case, histopathology reported necrotizing granulomas with a negative AFB stain. There has been literature evidence reporting that these SSTIs cases present with a mixed suppurative-granulomatous inflammation, with only a few cases showing well-formed granulomas.10 In most of these pathological cases, mycobacterial stains, such as AFB or FITE, are negative. However, negative stains do not entirely exclude the diagnosis and hence medical management by clinicians should be based on the culture, which remains the gold standard method for identification of AFB.11
There is limited literature evidence of M fortuitum as an opportunistic pathogen causing disseminated infection especially in immunosuppressed patients or receiving steroids.12 A case report of chyluria caused by Mycobacterium fortuitum infection in a 64-year-old male, who was successfully treated with two weeks of amikacin, trimethoprim-sulfamethoxazole and levofloxacin followed by 24 weeks of levofloxacin and doxycycline.13 Another case of Mycobacterium fortuitum osteomyelitis of the cuboid bone following a penetrating plantar trauma. The patient underwent a single-stage surgery and resolved the infection after 5 months of treatment with gentamicin-/vancomycin.14M. Fortuitum is resistant to all antituberculosis drugs but susceptible to macrolides, amikacin, doxycycline, fluoroquinolones, and trimethoprim-sulfamethoxazole. Therefore, an aggressive and prolonged NTM treatment is required to completely clear the infection and reduce the recurrence.
References
-Preeti Malik, M.D, MPH, PGY2 Pathology resident at Montefiore Medical Center.
-Phyu M. Thwe, PhD, D(ABMM), MLS(ASCP)CM is Associate Director of Infectious disease testing laboratory at Montefiore Medical Center, Bronx, NY.She completed her CPEP microbiology fellowship at the University of Texas Medical Branch in Galveston, TX. Her interest includes appropriate test utilization and extra-pulmonary tuberculosis.
One of the most common questions I’m asked by family members is “do you know when they died?” If death occurs in the hospital, or is witnessed, the time of death isn’t controversial. It’s common though in forensics that people may not be found for hours, days, weeks, or more. Forensics television shows usually depict an investigator measuring body temperature at the scene, and then confidently declaring they’ve been dead for 44 hours. Unfortunately, there aren’t any existing methods that actually give that level of precision – but there is a way we can systematically approach the question.
When determining time of death (TOD), it’s most important to keep in mind that it will be an estimate. The estimate starts with the “window of death” – the time between when the decedent was last known alive and when their body was found. The smaller this window, the greater accuracy is possible.
Once the window is known, one can assess postmortem changes of the body. Livor mortis is the gravity-dependent settling of blood within vessels, which can appear as soon as twenty minutes after death. Sparing of lividity will be present in areas of pressure, such as parts of the body pressed against the floor or with tight clothing. Livor is initially blanchable, but after 8 to 12 hours blood extravasates from vessels and it becomes “fixed”. Clearly though, this only allows one to differentiate between ‘less than’ or ‘greater than’ 8 to 12 hours.
Rigor mortis (stiffening of the body after death) occurs because of postmortem ATP depletion. Muscle fibers require a supply of ATP to both contract and relax – once ATP levels are sufficiently low, muscle will remain contracted until the fibers are broken down by decompositional changes. Generally speaking, rigor starts to develop within an hour of death, peaks from 12 to 24 hours, and dissipates by 36 hours. However, these are average intervals. The onset of rigor is hastened by vigorous physical activity, seizures, electrocution, or increased body temperature, which preemptively deplete ATP. Rigor is also harder to detect in people with low muscle mass (e.g. infants), and can’t be assessed in frozen bodies with those with extensive thermal damage.
Cooling of the body after death, known as algor mortis, is similarly prone to interfering elements. One can find many formulas for estimating the time of death based on the temperature of the body – unfortunately, none of them are particularly useful because of the assumptions that must be made. Change in temperature after death is affected by numerous variables, including body habitus, clothing, wind, actual body temperature at the time of death (not many people are constantly at 98.6℉), sepsis, terminal seizures, and many others. If the environment is warmer than the body, the temperature can even increase after death.
I’ll briefly mention vitreous potassium measurement, which is probably the most recently discovered (and debunked) “holy grail” of time of death. Similar to algor and rigor mortis, vitreous potassium does a reasonably decent job predicting time of death in a controlled experiment – but in this line of work, people don’t tend to die in controlled environments.
At the end of the day, time of death is best estimated by thorough scene investigation, correlated with the evidence the body provides. Newspapers or mail not retrieved from the mailbox, expiration dates on perishable groceries, last refills of prescriptions, and unreturned text messages or phone calls can all narrow down the window of death.
As stated earlier, the longer the interval between death and discovery of the body, the more difficult time of death determination becomes. In advanced decomposition, there is no rigor, livor, or algor remaining to assess (there may even be scant residual soft tissue). In one such situation, despite months of a potential “window of death”, dates on unopened bills and crossed-off calendar dates helped us place the time of death within one or two days. It’s not as flashy as multivariate equations for temperature or potassium levels, but it’s far more accurate and scientifically defensible.
Image 1. The quilting pattern of this decedent’s mattress is visible in the livor mortis on his back.Image 2. This decedent’s right arm is defying gravity due to rigor – he was initially face down, and his arm musculature became temporarily fixed in this position. Rigor can be forcibly broken if needed, but will also break down as decomposition proceeds.
-Alison Krywanczyk, MD, FASCP, is currently a Deputy Medical Examiner at the Cuyahoga County Medical Examiner’s Office.
Methicillin-resistant Staphylococcus aureus (MRSA) is a well-known cause of bacteremia, pneumonia, skin and soft tissue infections, and osteomyelitis, resulting in significant morbidity and mortality worldwide.1 Many testing methods (e.g. MALDI-TOF with susceptibility testing, molecular, chromogenic agar) have been developed for identification of MRSA and clinical microbiology laboratories will often use more than one. On occasion this leads to discrepant results which can be challenging to resolve and report.
How does methicillin resistance work?
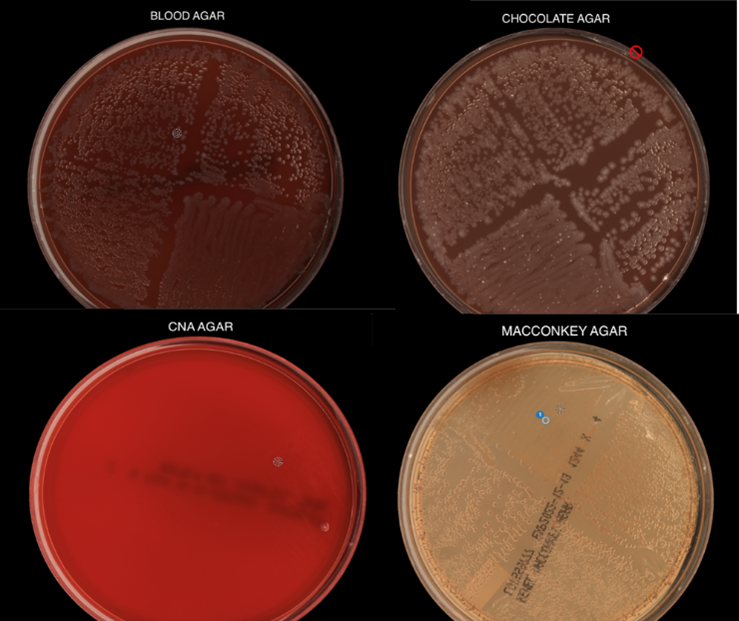
Staphylococcus aureus (SA)has a peptidoglycan cell wall containing alternating N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM) molecules with peptide chains reinforced by crosslinks. Crosslinking is mediated by penicillin-binding proteins (PBPs), which are the targets of beta-lactam antibiotics such as penicillins and cephalosporins.2 In methicillin-sensitive S. aureus (MSSA), these antibiotics bind PBPs and prevent formation of crosslinks, thus disrupting cell wall synthesis. However, methicillin resistance can occur if the PBPs are altered. MRSA produces PBP homologues such as PBP2a (encoded by the mecA gene) or more rarely, PBP2c (encoded by mecC), which don’t allow beta-lactam antibiotics to bind strongly so crosslinking occurs.3,4
Image generated by author.
What tests are used to identify MRSA?
MRSA testing can be genotypic or phenotypic, but most cannot be performed directly on patient samples. With molecular testing, we can detect mecA and/or mecC, the genes most commonly responsible for methicillin resistance. However, positive molecular results on a direct specimen source (e.g., positive blood culture) cannot be definitively attributed to SAif other mecA-harboring organisms such as methicillin-resistant Staphylococcus epidermidis are also present.5
When there is a pure isolate of SA growing in culture, lateral flow assays and latex agglutination tests can be used to interrogate the presence of mecA. Both lateral flow assays and latex agglutination tests detect PBP2a using antibodies specific to this alternative penicillin-binding protein. Chromogenic agars are a modern-day biochemical test, taking advantage of specific enzymes produced by MRSA (e.g. phosphatase) which cleave chromogens in the media.6
Disk diffusion and broth/agar dilution are the standard phenotypic methods for quantitating antimicrobial resistance in SA growing in bacterial culture. Despite the name, methicillin is no longer used for testing or treatment of MRSA. Per Clinical and Laboratory Standards Institute, oxacillin-resistant and cefoxitin-resistant SA should both be reported as MRSA and considered resistant to all beta-lactam antibiotics.7
Why don’t my test results match?
Although detection of the mecA gene or its protein product PBP2a are the standard7, mixed MSSA and MRSA cultures can lead to discrepant results. Another source of genotypic-phenotypic discrepancy are mecA mutations where the gene is still present and detected, but functional PBP2a is no longer produced. PBP2c only shares ~70% homology to PBP2aand is not detected by latex agglutination assays4-5, and mecC-mediated MRSA might be resistant only to cefoxitin and not oxacillin7. Other mechanisms of MRSA resistance are still being studied and not all are included on molecular test panels.
References
Turner, N.A., Sharma-Kuinkel, B.K., Maskarinec, S.A. et al. Methicillin-resistant Staphylococcus aureus: an overview of basic and clinical research. Nat Rev Microbiol 17, 203–218 (2019). https://doi.org/10.1038/s41579-018-0147-4
Sawa, T., Kooguchi, K. & Moriyama, K. Molecular diversity of extended-spectrum β-lactamases and carbapenemases, and antimicrobial resistance. j intensive care 8, 13 (2020). https://doi.org/10.1186/s40560-020-0429-6
Srisuknimit V, Qiao Y, Schaefer K, Kahne D, Walker S. Peptidoglycan Cross-Linking Preferences of Staphylococcus aureus Penicillin-Binding Proteins Have Implications for Treating MRSA Infections. J Am Chem Soc. 2017 Jul 26;139(29):9791-9794. doi: 10.1021/jacs.7b04881.
Ballhausen B, Kriegeskorte A, Schleimer N, Peters G, Becker K. The mecA homolog mecC confers resistance against β-lactams in Staphylococcus aureus irrespective of the genetic strain background. Antimicrob Agents Chemother. 2014 Jul;58(7):3791-8. doi: 10.1128/AAC.02731-13.
Lakhundi S, Zhang K. Methicillin-Resistant Staphylococcus aureus: Molecular Characterization, Evolution, and Epidemiology. Clin Microbiol Rev. 2018 Sep 12;31(4):e00020-18. doi: 10.1128/CMR.00020-18.
Flayhart D, Hindler JF, Bruckner DA, et al. Multicenter evaluation of BBL CHROMagar MRSA medium for direct detection of methicillin-resistant Staphylococcus aureus from surveillance cultures of the anterior nares. J Clin Microbiol. 2005;43(11):5536-5540. doi:10.1128/JCM.43.11.5536-5540.2005
CLSI Performance Standards for Antimicrobial Susceptibility Testing M100, 32nd edition. (2022) Clinical and Laboratory Standards Institute
– Angelica Moran, MD, PhD is a clinical microbiology fellow at University of Chicago Medicine and NorthShore University Healthsystem and research fellow at the Duchossois Family Institute. She is interested in translational research developing clinical laboratory diagnostics for precision medicine and the microbiome.
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
A 40 year old man was found deceased in a parking garage in a Midwest city. It was late October and had rained the previous evening. He was identified by his sister who was a tenant in the adjacent apartment building. Unknown to her, he had recently been discharged from the hospital after a one-week psychiatric admission. His sister stated he was homeless and would occasionally sleep in the parking garage for shelter.
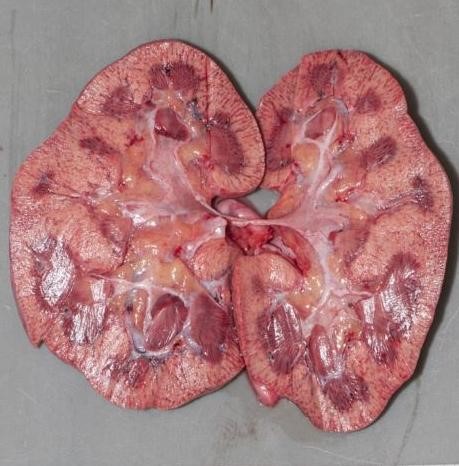
At the scene the decedent was prone on the ground, clad only in a pair of boxers. His water-soaked shoes, socks, sweatpants, and shirt were strewn about him. Autopsy revealed an atraumatic, thin adult man. Prominent pink discoloration was noted over the hips and knees. Internal examination showed only patchy black-brown discoloration of the gastric mucosa and pale kidneys. Histology was remarkable for subnuclear vacuolization of the renal tubular epithelium. The cause of death was certified as environmental hypothermia, and the manner of death accidental.
Hypothermia is defined as a core body temperature below 95℉ (35℃) and can result from endogenous illnesses like hypothyroidism or sepsis. The most common cause, though, is exposure to cold environments. On exposure, the hypothalamus initiates shivering and increases cellular metabolism to produce heat. Another crucial survival response is vasoconstriction, particularly of vessels in skin and skeletal muscle. If the overall loss of heat overtakes the body’s ability to produce or retain heat, hypothermia will result.
Developing hypothermia doesn’t require frigid weather – in dry air, temperatures of 50℉ can still result in hypothermia. Wind removes warmed air surrounding the body, and water conducts heat three times faster than air; therefore, with either of these factors present, people can develop hypothermia at even warmer temperatures,
The autopsy findings of hypothermia are not specific. External examination may show bright pink discoloration of the skin over joints (“frost erythema”). There may be black-brown spots on the gastric mucosa, (“Wischnewsky spots”), thought to result from terminal vasodilation of submucosal vessels. The kidneys may be pale with microscopic subnuclear vacuolization of the tubular epithelium (the “Armanni-Ebstein” lesion). Acute hemorrhagic pancreatitis has also been described. However, these findings require a period of survival to develop—many cases, particularly if the decedent succumbs quickly, show no findings at all. The diagnosis of hypothermia therefore relies heavily on scene investigation. “Paradoxical undressing” (demonstrated in this case), refers to the phenomenon of a terminally hypothermic person taking off their clothes. This is caused by a feeling of warmth resulting from failure of vasoconstriction in the skin, and contributed by altered mentation.
Those at greatest risk are people spending extended time outdoors, including the homeless and outdoor recreationalists. The elderly and very young have a lower ability to centrally regulate body temperature. Children’s increased body surface area also leads to more rapid heat loss. People who are intoxicated with alcohol or drugs may not sense the cold or lack judgment to seek shelter. Alcohol also acts as a vasodilator, impairing vasoconstrictive adaptation to cold.
As the weather cools down, be mindful of how easily hypothermia can develop. Temperatures can be above freezing, yet those who are vulnerable are still at risk of hypothermia. Prepare yourself well for any snowy excursions, and keep an eye on those in your community who may not be able to seek shelter.
Stomach mucosa showing spots of black or dark brown discoloration known as Wischnewsky spots. These are not specific to hypothermia and may just be an indicator of physiologic stress.Bright pink discoloration over the knees, or “frost erythema”.Pallor of the renal cortices corresponds to the microscopic “Armanni-Ebstein” lesion. This isn’t specific to hypothermia and can be seen in ketoacidosis from any cause.
-Alison Krywanczyk, MD, FASCP, is currently a Deputy Medical Examiner at the Cuyahoga County Medical Examiner’s Office.