Emergency services were called to a fire in a small apartment building, in which the structure was completely engulfed. Most of the occupants had been evacuated – however, once the fire was extinguished, the charred remains of an adult woman were found in the debris.
At the autopsy of severely fire-damaged human remains, two key questions must be answered: 1) who is the decedent?, and 2) were they alive when the fire started?
Question #1 is particularly relevant in this case, as many people lived in the building. Presumptive identification based on the tenant list may seem reasonable at first, but this victim could represent a visitor, contractor, or subletter. When facial identification isn’t possible, radiographic identification can be done with dental x-rays or x-rays of other bones which may have unique features from healed trauma or degeneration. Additional methods of positive identification could include fingerprints (if still intact), or DNA comparison to first degree relatives.
Question #2 is of importance because fire can be used in an attempt to disguise the identity of a victim of violent crime and destroy evidence. Cutaneous evidence of trauma may be disguised by burns, so full body x-rays are taken of every fire-damaged body. X-rays can also reveal retained bullets, knife tips, or fractures unlikely to have been caused by the fire.
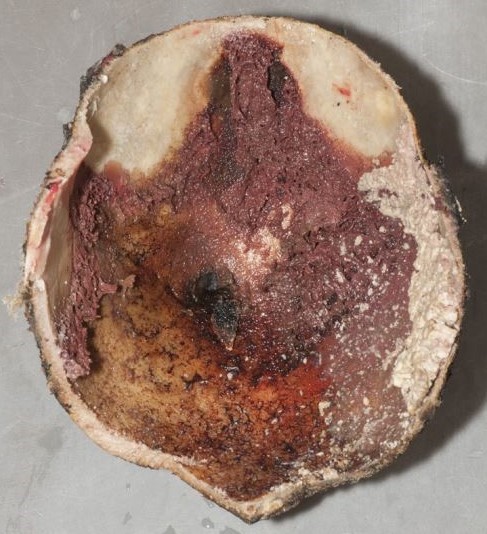
When deciding if a fire victim was alive when the fire started, we first examine the upper and lower airways for soot. Most fire victims do not die from cutaneous burns, but from smoke inhalation – including carbon monoxide (CO) toxicity, which is often apparent by cherry red discoloration of the blood and viscera. Postmortem carboxyhemoglobin measurements in house fire victims are typically greater than 50%. There are exceptions to this rule, of course. Rarely, someone who was clearly alive when the fire began will have minimal or no soot in their airways and a negligible carbon monoxide concentration. This can happen in a “flash fire”, such as one ignited by gasoline or oxygen tanks, in which thermal injury to the upper airway may cause rapid occlusion by laryngospasm or edema. People with underlying heart or lung conditions will be more susceptible to the effects of carboxyhemoglobin, and may not survive long enough to obtain a level above 50%. Fires also produce other toxic products of combustion such as cyanide, and can lower ambient oxygen saturations to result in asphyxiation by lack of ambient oxygen (even without CO).
Forensic pathologists need to be aware of the artifacts that fires can create. Pugilistic posturing of fire victims (limb flexion) is due to heat-related contraction of muscle fibers. Epidural hematomas can result from boiling blood and bone marrow within the calvarium extravasating into the epidural space. The heat can induce fractures in exposed bone once the surrounding soft tissue is consumed or fully charred. Finally, the heat can split apart skin and soft tissue, resulting in sharp-force-like defects which occur parallel to the orientation of muscle fibers (rather than across them, which is more suspicious for penetrating trauma).
Of utmost importance in fire-related deaths, however, is scene investigation. The manner of death in fire fatalities is related to the origin of the fire. Most fire deaths are accidental, as the fire is unintentionally sparked by some electrical malfunction or unattended flame. However if the fire started intentionally, the manner of death can be homicide (if started by another) or suicide (started by the victim). It is therefore crucial to review the final fire investigation report before finalizing the autopsy report and death certificate.



-Alison Krywanczyk, MD, FASCP, is currently a Deputy Medical Examiner at the Cuyahoga County Medical Examiner’s Office.
