You know that old adage “you can’t teach an old dog new tricks”? Well, laboratory professionals know that’s wrong—not only do we need to learn new tricks, sometimes we need to learn them in order to help diagnose a patient. In that regard, continuing education sessions—like those at ASCP’s Annual Meeting—can be so helpful to bench technologists. Today, I attended “Team Approach to Diagnosis of Fungal Infections” presented by Dr. Jeannette Guarner, MD, FASCP from Emory University in Atlanta, Georgia. Here are some of the tidbits I learned.
An easy reminder for dimorphic fungus: “mold in the cold, yeast in the beast.”
In direct stains of tissue samples, not all broad-based budding yeast 8 to 15 microns are Blastomyces. It could be Candida or even Aspergillus.
If you’re able, tell the clinician to send to biopsy samples for micro AND pathology—shared specimens tend to introduce error.
Paracoccidioidomycosis is much more common in males (20:1); current thinking is that estrogen is protective.
Chrysosporium (previously Emmonsia): dimorphic yeast currently only seen in South Africa.
Fusarium can grow in blood cultures. (In the tissue, it almost looked like Aspergillus with hyaline septated hyphae.)
Fusarium is generally resistant to antifungals
When seen in tissue samples, hyaline septated hyphae DOES NOT ALWAYS equal Aspergillus.
Black molds are black because of melanin, which protects them from UV rays, heavy metals, free radicals, and high temperatures.
Cryptococcus is the only fungus that has mucin in its cell wall; mucin stain will be positive.
Crypto can sometimes do a broad-based budding.
-Kelly Swails, MT(ASCP), is a laboratory professional, recovering microbiologist, and web editor for Lab Medicine.
Hello again readers. It’s been a while as I took some time off from blogging. But I hope to update you every once in a while when I can. So, I’m currently in my final year of residency and have been serving as chief since April 1st. My chief term ends before the end of the year to provide time to focus on studying for the boards (we take our boards in mid-May).
When I reminisce about residency, I can’t believe that almost four years have flown by so quickly. I remember arriving in Chicago for a 2 week boot camp we had prior to our start date on July 1st just like it was yesterday. It was nice to be back in a familiar city (The University of Chicago is my alma mater), although many things had changed in the two decades since I had last been a college student in the Windy City.
Thinking about it now, I really appreciate all the thought and hard work that my director of surgical pathology, Dr. Elizabeth Wiley, had put into organizing this boot camp to ease us into the transition to residency (and surgical pathology). We learned Rokitansky method of autopsy dissection on 3 pig blocks that she personally picked up from the butcher’s for us and later had to complete a competency exam by ourselves on a 4th pig block. We learned to cut frozen sections on various tissues from our pig blocks (and of course, had a competency exam on that as well). We learned to gross uteri and prostates on ground turkey versions (complete with chickpea leiomyomas) that she and her fellows had made for us. We had weekly online exams on histology (we had a slide scanner which I now appreciate that not everyone has one) and special didactics on surgical pathology topics we don’t see much during general sign-out (dermatopathology, neuropathology, hepatopathology, and nephropathology) in addition to the usual goings-on during a surgical pathology rotation. We eventually had online modules on surgical pathology as well. And of course, we had three months straight (I hear its five months now) of learning to gross with our awesome fellows. I now appreciate more deeply just how innovative and dedicated Dr. Wiley was to our surgical pathology education. And even though I ultimately chose to pursue fellowships in hematopathology and molecular genetic pathology, the foundation in surgical pathology that was established during that boot camp still helps and influences me now.
During my first year, I was also fortunate to have hematopathology at Jesse Brown VA Medical Center with Dr. John Kennedy. He is a hematopathologist who was trained as a morphologist before the heavy reliance on flow cytometry and IHC. And he taught me to love the morphology of blood cells especially with respect to lymphomas. I had enjoyed my hematology sub-I at the NIH when I was a medical student but had originally entered residency thinking that I’d pursue molecular genetic pathology and clinical microbiology. But a great mentor can really open your mind to a different path and that is what Dr. Kennedy did for me. The second time I rotated with him, he was away for much of the rotation. But I loved the opportunity that I was given to take care of the hematopathology service in his absence. I looked at all the daily cases and performed path reviews and counts on peripheral blood smears and body fluids and the surgical pathology attending at the end of the day would review and sign-out my work. This experience of graduated responsibility helped me to decide to pursue hematopathology and it was nice to have someone believe in me and my abilities. I was also fortunate that I was in a city where the Lymphoma Foundation also held quarterly inter-program Lymphoma Rounds which I was able to attend.
So my advice is to identify mentors early on in your residency. You may not be able to see the ripple effect they have on your life until later on but I promise that they will touch your lives in an indelible manner that will help shape the pathologist you will become later on in life.
This week I’m at the ASCP Annual Meeting and will write about those experiences in a future blog, but for now, I’d like to take this opportunity to personally thank my mentors. I hope that I take your lessons and make you proud as a future physician-scientist with a public health (molecular epidemiology aka biomarker discovery which was one of my areas of specialization during my MPH) focus. You have touched my life in ways that I may not always be able to articulate but do acknowledge and appreciate.
-Betty Chung, DO, MPH, MAis a fourth year resident physician at Rutgers – Robert Wood Johnson University Hospital in New Brunswick, NJ.
One of the interesting things about working in the field of laboratory medicine is that there are always opportunities for learning new things. Almost every call I get from my colleagues outside the lab allows me and the lab team these opportunities. And sometimes we are reminded of the reason we do the things we do, basically re-learning them.
Case in point: An ICU physician contacted the lab, understandably concerned. He had been monitoring the pO2 in a patient using an I-Stat point of care analyzer. Values had been in the range of 50-70 mmHg, and he had been adjusting ventilation on the basis of those results. A blood gas sample was sent to the main lab, analyzed on an ABL analyzer and gave a result of 165 mmHg, repeated shortly thereafter on a new sample with a 169 mmHg. Understandably, the physician wanted to know which analyzer was wrong and how he should be adjusting his patient’s ventilation.
We quickly did an investigation and determined an interesting fact that we hadn’t paid much attention to previously. A blood gas sample that is sent through the tube system that has any amount of air in the sample, will give falsely elevated pO2 result. We investigated this by collecting blood gas samples, running them on both the I-Stat and the ABL, and then sending them through the tube system and rerunning them on both instruments after tubing. The pO2 values matched on both instruments, both before and after tubing. But interestingly, if there was any air in the collection device when the device was sent through the tube system, the pO2 after tubing still matched on the two instruments, but the values were more than double the original values. If no air was present, there was very little change before and after tubing. We tested this by expressing all air from one set of samples before tubing and leaving air in the syringe on the other set.
The collection process for blood gas samples in our institution has always specified that the collector should express any air in the sample before sending the sample to the lab through the tube system, and after this incident the reason for that step became clear. However, the staff collecting blood gases on the floors needs to be periodically retrained in the collection, and the lab staff needs to be reminded that air in a blood gas syringe arriving through the tube station is a reason to reject the sample. We were reminded that education needs to be a continuous process. We also learned that when we discover the reason for a process, it’s a good idea to document that reason in order to both understand the need and to help motivate people to follow it.
-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.
The American Society of Cytopathology is conducting a reproducibility study, and they need your help. They’d like for participants to evaluate images from the new Paris System for Reporting Urinary Cytology Atlas. If you’re able to participate, follow this link.
Just in time for Halloween: a recently-published study in mBio discusses the 2014 outbreak of Listeria monocytogenes tied to caramel apples. There’s not enough water in caramel and an apple is too acidic to support this bacterium, so how did this outbreak occur? From the study: “Our findings suggest that the 2014 listeriosis outbreak associated with caramel-coated apples can be explained by growth of L. monocytogenes occurring at the interface between two foods which, by themselves, are inhibitory to pathogen growth.”
Case history:
An 18 year old pregnant woman at 16 weeks gestation presented at the emergency department with nausea and vomiting for 3 days. Three days ago she and some of her friends ate chicken at a party. None of her friends experience her symptoms. Laboratory tests revealed urinary tract infection and a stool sample was sent to the microbiology laboratory for culture.
She was prescribed an antibiotic and was released from the ED.
Laboratory identification:
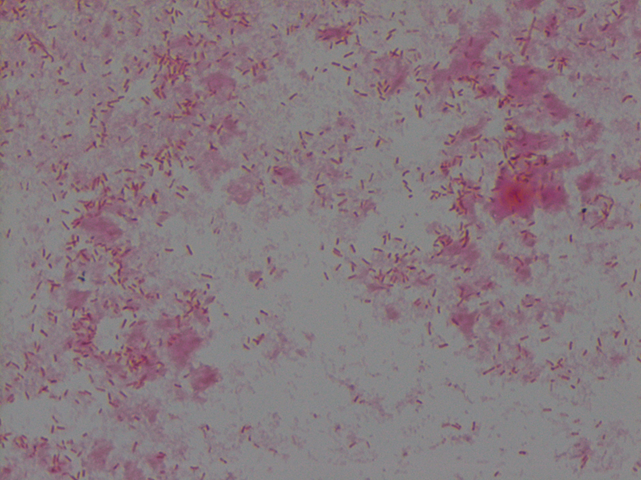
The organism grew well on MacConkey agar, and formed small colorless lactose-negative colonies. Gram stain revealed short gram-negative bacilli and MALDI-ToF confirmed the bacteria as Yersinia enterocolitica.
Non-lactose fermenting, flat colonies on MacConkey agarGram stain of Yersinia enterocolitica reveals Gram-negative bacilli
Discussion: Yersinia enterocolitica is a gram negative, short, non-spore-forming bacillus in the family Enterobacteriaceae. They can exhibit bipolar staining, especially from the primary sample. It is a facultative anaerobe can grow at temperatures ranging from 4-43oC that is motile at room temperature but non-motile at 37oC. The organism grows well on MacConkey agar, and forms small colorless lactose-negative colonies but if the clinical team is suspicious for Yersinia, a selective growth medium is recommended. The most widely used is cefsulodin-irgasin-novobiocin (CIN) agar, which inhibits the growth of competing flora and produces characteristic colony morphology (red color with “bull’s eye” appearance).
The major route of Y. enterocolitica infection is through contaminated foods or water. The primary pathogenic event is colonization of the intestinal tract where most of the pathologic effects and clinical manifestations occur. Temperature and calcium concentration regulate expression of virulence factors that guide the invading Yersinia and allow them to survive and disseminate.
The most common form of disease caused by Y. enterocolitica is gastroenteritis associated with consumption of contaminated food or water, especially raw or undercooked pork such as chitterlings. Disease can range from self-limited gastroenteritis to terminal ileitis and mesenteric lymphadenitis that can be misdiagnosed as appendicitis. Gastrointestinal infections are usually self-limiting and do not merit antimicrobial therapy. However, in immunocompromised hosts and in patients with septicemia or invasive infection, the mortality can be high (approximately 50%).
Kossivi Dantey, M.D. is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
–Christi Wojewoda, MD, is certified by the American Board of Pathology in AP/CP and Medical Microbiology. She is currently the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Antibiotic resistance is a huge concern for microbiologists. In addition to stewardship programs and regulating agricultural use of antibiotics, is it time to re-examine clinical testing paradigms?
A recent study suggests that the typical way microbiologists test for antibiotic susceptibility–meuller-hinton plates and antibiotic disks–might be fallible. When his team tested Salmonella against polymyxin using typical methods, the organism tested sensitive; when the tested the same organism against the same antibiotic using medium that more closely resembled human cells, the organism tested resistant.
Bloomberg Business discusses the paper here. The article is worth your time, even if the info-graphic gives erroneous information (it mentions meuller-hinton broth instead of meuller-hinton agar plates).
Ammonia is a small molecule that is produced as a part of normal tissue metabolism. Its formation results from the breakdown of compounds containing nitrogen, such as the amino groups in proteins and the nitrogenous bases in nucleic acids. In the tissues, ammonia is stored mainly in the form of amino acids, specifically the amino acid glutamine which has three amino groups. Normally, the body can remove excess ammonia easily via the liver pathway known as the urea cycle. This short, 4-step cyclical pathway converts two ammonia molecules into a small, water soluble urea molecule, making it able to be easily excreted in the urine. Without a functional urea cycle however, the body has no other adequate mechanism for getting rid of the ammonia that is constantly being produced by metabolism.
Liver damage or disease can disrupt the urea cycle, causing blood ammonia levels to rise. This is the most common cause of elevated ammonia in the adult population. In a pediatric patient, elevated ammonia is frequently seen as a consequence of an inborn error of metabolism (IEM). Many IEM, especially those in the urea cycle pathway, will result in elevated blood ammonia levels. In addition, in IEM causes, the ammonia concentrations may be well over 1000 µmol/L, when the normal range of ammonia is generally in the 30 – 50 µmol/L range. Elevated blood ammonia concentrations are serious because ammonia is toxic to the brain. The higher the ammonia concentration is, and the longer it stays high, the more brain damage that will occur.
Interestingly, the concentration of ammonia in the blood may not correlate with the neurological symptoms that are seen. Usually if the ammonia concentration is <100 µmol/L, the person will show no symptoms at all. Concentrations of ammonia in the 100 – 500 µmol/L range are associated with a wide variety of symptoms including: loss of appetite, vomiting, ataxia, irritability, lethargy, combativeness, sleep disorders, delusions and hallucinations. These patients may present with an initial diagnosis of altered mental status, and if there is no reason to suspect an elevated ammonia, the symptoms may lead to drug or alcohol testing. When ammonia concentrations are >500 µmol/L, cerebral edema and coma may be seen, with cytotoxic changes in the brain. Ammonia concentrations in the 1000+ µmol/L range are extremely critical and are treated aggressively with dialysis to pull the ammonia out of the system. In particular, urea cycle defects require close monitoring of ammonia and glutamine concentrations, with immediate response when they rise.
Laboratory testing for ammonia is often problematic as contamination can occur from a number of sources including atmospheric ammonia, smoking and poor venipuncture technique. In addition if the sample is not centrifuged and analyzed promptly, ammonia is formed by the continuous deamination of amino acids and the concentration increases by 20% in the first hour and up to 100% by 2 hours. Consequently samples to be tested for ammonia should be placed on ice immediately after being collected and transported to the lab for analysis as soon as possible. Many minimally elevated ammonia results are a consequence of poor sample handling. However, a truly elevated ammonia is a critical lab finding that should be addressed immediately.
-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.
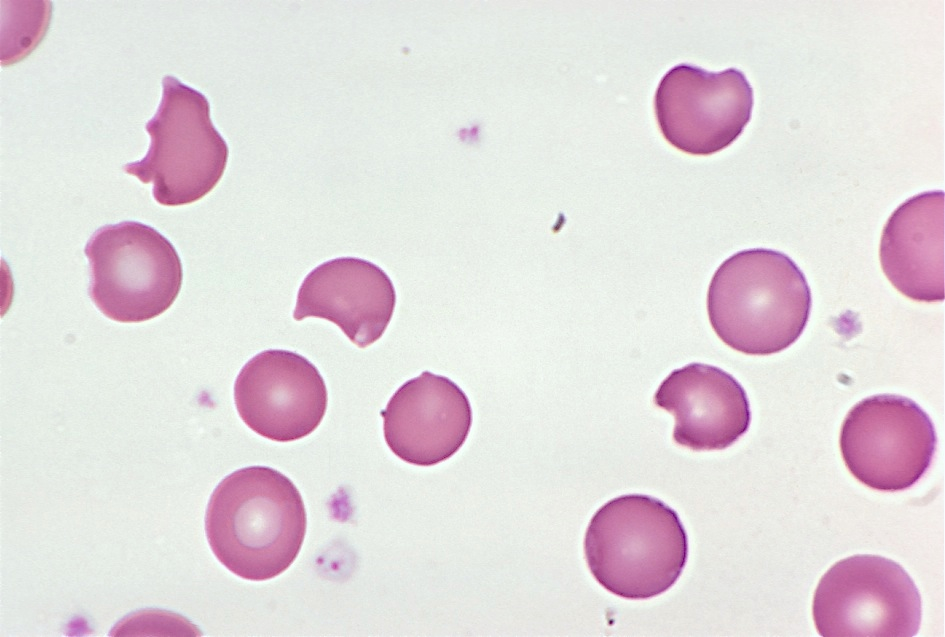
A 32-year-old male presents with mild jaundice and flank pain. He recently developed sinusitis, which was treated with trimethoprim-sulfamethoxazole, but is otherwise healthy. His hemoglobin is 10.2 g/dL (13.5-17.5), MCV is 90 μm3 (80-100), and total bilirubin is 3.4 mg/dL (0.2-1.5). A representative field from his blood smear is shown here. What is the most likely diagnosis?
Aplastic anemia
Iron-deficiency anemia
Glucose-6-phosphate dehydrogenase deficiency
Autoimmune hemolytic anemia
Megaloblastic anemia
The answer is glucose-6-phosphate dehydrogenase (G6PD) deficiency. G6PD deficiency is an X-linked recessive disorder in which patients produce decreased amounts of G6PD, a red blood cell enzyme involved in detoxifying free radicals.
When a patient with G6PD deficiency is exposed to an oxidant stress (which can be anything from an illness to ingestion of certain foods or drugs), the resulting reactive oxygen species attack structures within the red cell.
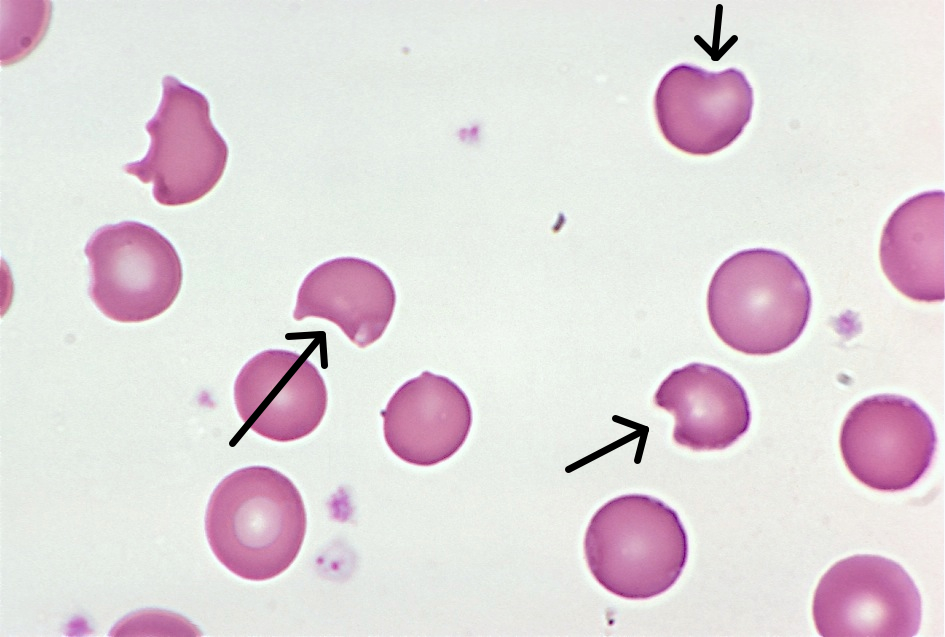
Globin chains are particularly vulnerable to oxidant damage. They become denatured and stick to the inside of the red cell membrane, forming inclusions called Heinz bodies, which are visible on crystal violet staining. Heinz bodies are removed by macrophages in the spleen, leaving visible “bites” in the red cells. Several bite cells are visible in this patient’s blood smear (arrows).
Most episodes of hemolysis in patients with G6PD deficiency resolve on their own after the offending substance is removed.
-Kristine Krafts, MD, is an Assistant Professor of Pathology at the University of Minnesota School of Medicine and School of Dentistry and the founder of the educational website Pathology Student.
An 8 week old female was brought to an outside hospital due to pallor, decreased eating over several days, vomiting, fever, and blue color in the feet. The patient had received her two month vaccinations the day prior to presentation. Her past medical history was significant for being born at 32 weeks gestation, followed by an uneventful 4 week NICU stay. At the outside hospital the patient was in respiratory distress, tachycardic, with pallor. She was intubated and transferred to our institution due to concern for an ALTE (apparent life-threatening event). Blood and CSF specimens were drawn. Upon presentation, the patient had a white blood cell count of 19,600/mm3. Her CSF had 63 nucleated cells/mm3 (30% neutrophils, 49% lymphocytes, 11% monocytes), glucose of 23 mg/dL and protein of 212 mg/dL. Blood and CSF cultures were performed with the following results:
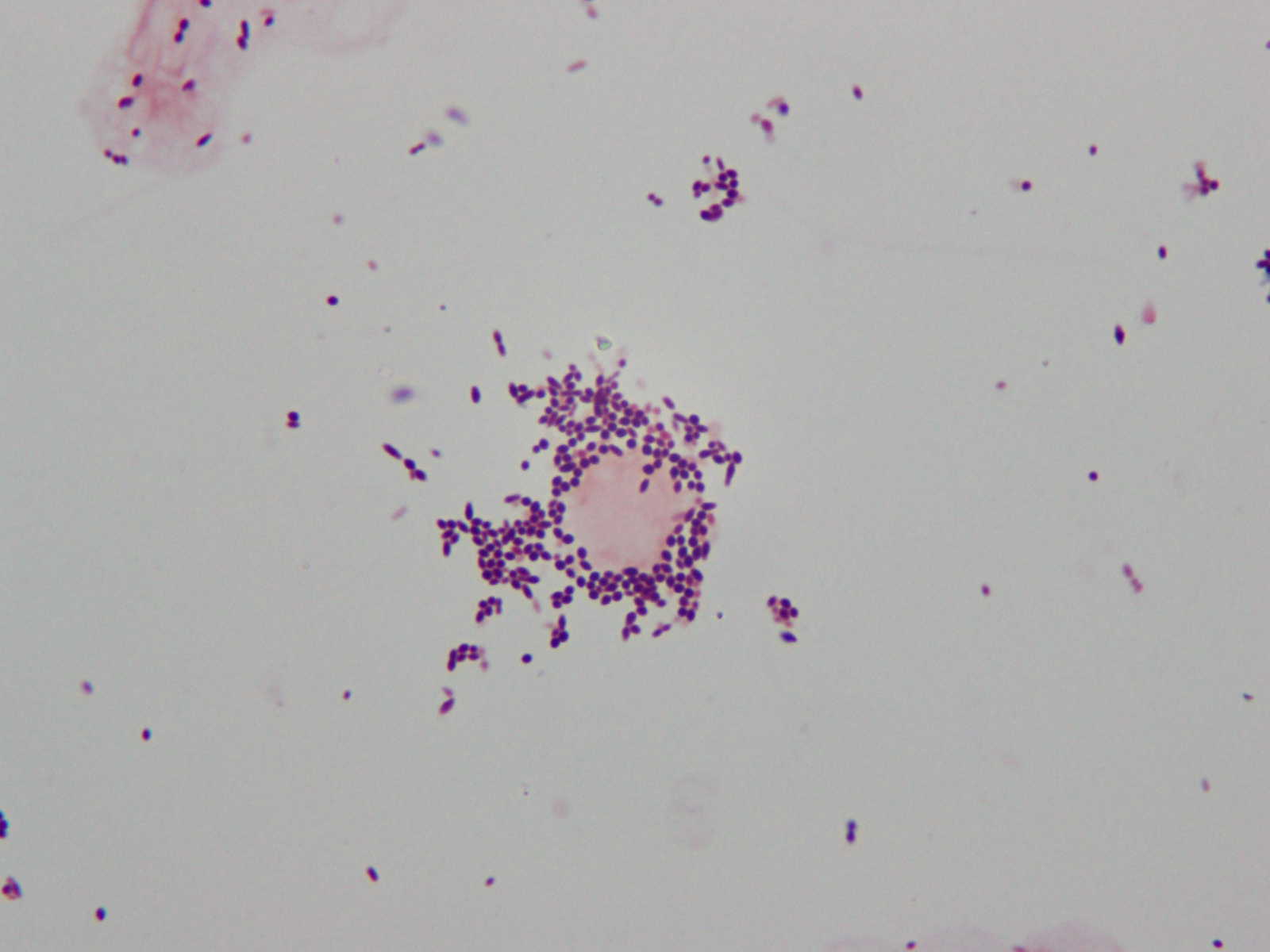
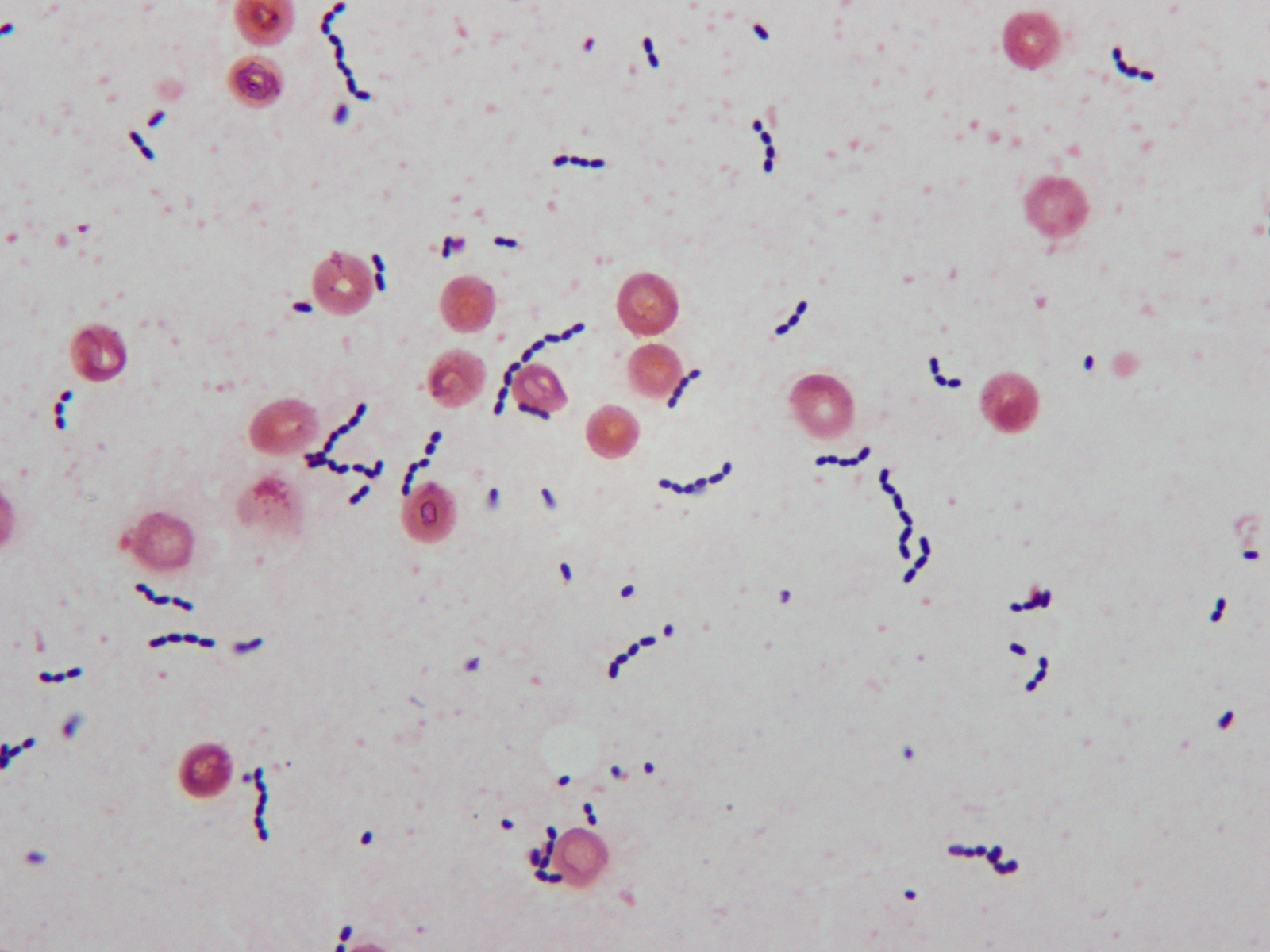
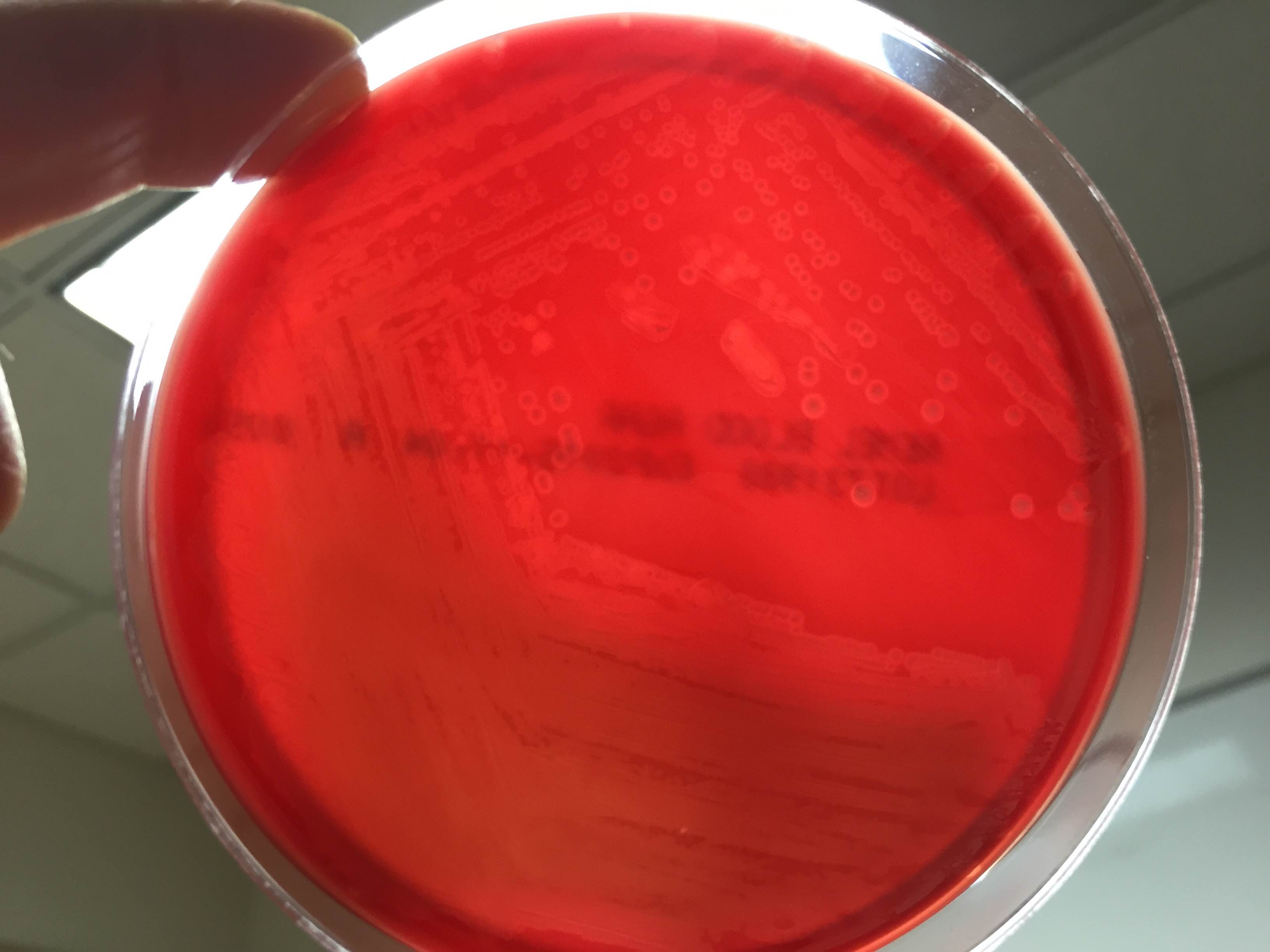
Gram stain of cerebral spinal fluid (CSF) specimen showing Gram positive cocci in singles and pairsGram stain of positive blood culture broth showing Gram positive cocci in chainsSmall zones of beta hemolysis around colonies growing on 5% sheep blood agar
Laboratory Identification
CSF Gram stain was read as many Gram-variable coccobacilli (Image 1) and blood culture Gram stain was resulted as Gram-positive cocci in pairs and chains (Image 2). The Nanosphere Verigene Gram-positive blood culture molecular assay was performed on the positive blood culture broth immediately following Gram staining. CSF and positive blood culture specimens were plated to 5% sheep blood, chocolate, MacConkey, and CNA agars. In >24 hours colonies from both specimens grew a single organism on sheep blood, chocolate, and CNA agars. On blood agar, colonies exhibited a soft zone of b-heomlysis (Image 3). Colony Gram stains showed Gram-positive cocci in chains, catalase testing was negative, and the organism typed in Lancefield antigen group B. Verigene identified the organism directly from the positive blood culture broth as Streptococcus agalactiae (aka Group B Streptococcus or GBS) and MALDI-TOF mass spectrometry confirmed the identification of S. agalactiae.
Discussion
Laboratory Considerations
As our CSF specimen demonstrated, streptococci can be difficult to interpret from specimen Gram stains. Organisms are often are pleomorphic in size and shape and they have a tendency to stain Gram-variable. This lead to the report of Gram-variable coccobacilli on our patient’s CSF culture.
S. agalactiae produces a soft zone of b-heomlysis on sheep blood agar. Unlike Streptococcus pyogenes (aka Group A Streptococcus) which produces a wide zone of b-hemolysis, soft b-hemolysis can often be very subtle, especially with young growth. Soft zones b-hemolysis can best be seen by holding plates up to a light source or my moving a colony out of the way to observe if hemolysis is present underneath. The pattern of S. agalactiae b-hemolysis is very similar to that produced by Listeria monocytogenes. Streptococcal isolates that type as Lancefield Group B, but produce large zones of b-hemolysis can create confusion and are most likely not S. agalactiae, but S. porcinus or S. pseudoporcinus.
Clinical Significance
S. agalactiae is the cause of significant neonatal disease. Early-onset infection presents as systemic infection, respiratory distress, apnea, shock, and pneumonia within the first 24 hours of life (range, 0–6 days). Meningitis is less common in early-onsetS. agalactiae infections, found in just 5-10% of cases. Late-onset disease presents at 3 to 4 weeks of age (range, 7–89 days) as meningitis and/or sepsis with other focal infection. Approximately 50% of survivors of early- or late-onset meningitis have long-term neurologic sequelae.
S. agalactiae colonizes the urogenital or gastrointestinal track of 10-30% of pregnant women. Being born to a S. agalactiae colonized mother is the most significant risk factor for development of disease in neonates. For this reason, women are screened for “Group B Strep” colonization between 35 and 37 weeks of pregnancy. Women found to be colonized receive prophylactic antibiotics immediately prior to delivery to prevent transmission to the child. Since implementation of these practices in 1996, there has been a substantial decline in early-onset S. agalactiae infections. Interestingly, these measures have not affected the incidence of late-onset disease.
Treatment
Until recently S. agalactiae was considered universally susceptible to penicillin. There have now been a few reports of S. agalactiae isolates with increased penicillin MICs due to mutations in the penicillin binding protein Pbp2x. The detection of these isolates is still extremely rare, so much so that S. agalactiae susceptibility testing for penicillin and other b-lactams is not considered necessary at this time. Penicillin and its derivatives are the preferred treatment option.
Patient follow-up
Our patient had a complicated course of late-onset Group B Streptococcal meningitis including multifocal cerebral infarctions and seizures. She was treated with a 28 day course of ampicillin. Blood cultures taken 24 hours after the start of antibiotics were negative and her CSF culture was negative when rechecked 5 days after her presentation. Due to her complicated course, the patient was hospitalized for 4 weeks. Follow-up appointments have shown the patient’s MRI is nearly normal 8 weeks post infection and the patient is doing well, although she is still followed by neurology to assess for long term sequelae.
Our patient’s mother had an unknown Group B Strep carrier status at the time of her birth, as she was born at 32 weeks, which is before routine screening occurs for pregnant women. Either way, the mother’s status would not have affected the patient’s risk for late-onset Group B Streptococcal infection.
References:
Red Book 2015
Journal of Clinical Microbiology, 10th edition
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.