A 64 year old male presented with one week of swelling in his right 4th finger. He was initially treated for a suspected bacterial infection, but did not respond to treatment and the finger was aspirated. The specimen was positive for fungal organisms.
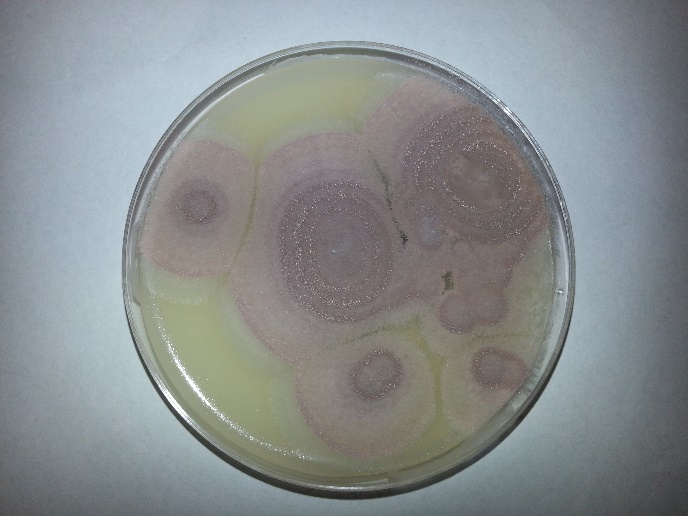
Fungal plates grew the following:
Note the flat powdery/velvety colony growth. It is common for the colonies to have a purple or lavender color with a white border.
Scotch tape prep revealed the following morphology:
Note that the elongated phialides, and taper to a long slender tube, resembling bowling pins. Sometimes this morphology has also been referred to as “skeleton hands.”
Discussion: Purpureocillium lilacinum (formerly Paecilomyces lilacinus) is a fungus that is found ubiquitously within our environment, but has rarely been associated with disease in humans. A review paper in 2004 found 119 reported cases that implicated P. lilacinum from 1964 to 2004. It has been most commonly associated with ocular infections, often linked to intraocular lens implantations. There is scarce data concerning its susceptibility. In the event of a cutaneous infection such as the one presented in this case, it is recommended that posaconazole be used as first line therapy. In the event of treatment failure, or intolerance, there is little data about which antifungals to treat with, though voriconazole has been shown to have successful in-vitro.
The patient in this scenario had a history of undifferentiated spondylarthropathy, and was on methotrexate for a monoarthropathy in same finger in which the fungal growth occurred. He also received a cortisone injection into the joint adjacent to, but not directly into the site of the infection approximately a month prior to presentation. It could be possible that the cortisone injection had allowed the fungus to be inoculated into the finger, but we may never be certain. The patient also was gardening prior to his infection, and that could have also possibly contributed to his fungal infection.
P. lilacinum is found readily in the environment, and should be considered on the differential of cutaneous infections. Though immunocompromised patients have historically been more susceptible, it has been reported in immunocompetent individuals and should be considered, especially in the event of failure of response to antibiotic treatment. More research needs to be done to better understand treatment regimens for this organism, though this is difficult as it has been difficult to test in animal models.
Reference:
Clinical manifestations, treatment and outcome of Paecilomyces lilacinus infections. F.J. Pastor and J. Guarro. Volume 12, Issue 10, pages 948–960, October 2006 DOI: 10.1111/j.1469-0691.2006.01481.x
-Rich Smith is a Pathology Student Fellow at University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
“The Clinical and Laboratory Standards Institute (CLSI) has published a revised document titled Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria (M45-Ed3).This guideline informs clinical, public health, and research laboratories on susceptibility testing of infrequently isolated or fastidious bacteria that are not included in CLSI documents M02, M07, or M100. Antimicrobial agent selection, test interpretation, and quality control are discussed. “Susceptibility testing is particularly necessary in situations in which the etiological agent belongs to a bacterial species for which resistance to commonly used antimicrobial agents has been documented, or could arise. The intent of this document revision is to assist labs in determining an approach for testing that is relevant to their individual practice settings.”
A 22 year old male, treated for gonorrhea one month ago, presents with two days of dysuria and white penile discharge. He reported complete resolution of his symptoms with treatment. He has had sexual contact with 2 partners in the past month.
Cultures are taken and the following is seen on gram stain.
N. gonorrhoeae is a gram negative diplococci responsible for the disease of gonorrhea. Though most specimens for gonorrhea are received from sources suspected of having the disease, it should be noted that whenever dealing with a gram negative diplococci of unknown source, care should be taken, and the specimen should be handled under a hood for possible exposure to N. meningitidis.
Seems like a clear cut case of gonorrhea, but given the patient’s history is this treatment failure, or likely reinfection?
The CDC has warned that rates of antibiotic resistant gonorrhea are on the rise. A once easily curable disease, is now becoming resistant to our mainstay treatment of ceftriaxone and azithromycin. Although cases have been reported, the majority of ‘failure of treatment’ scenarios are likely re-infection. Patients likely do not abstain until they are symptom free, or the partner may not be treated, leading to a reinfection of the patient. In the event of treatment failure, the CDC even recommends re-treating with the same ceftriaxone/azithromycin regiment. It is still recommended that a sample be taken for culture in the event that there is any concern over failure of treatment and possible antibiotic resistance.
Historically, testing for N. gonorrhoeae consisted of culture and gram stain, but the CDC now recommends testing for gonorrhea with nucleic acid amplification testing (NAAT). This test has improved sensitivity, less subjectivity and a much faster turnaround time than gram staining and culturing. It cannot, however, be used for test of cure, as the NAAT tests for DNA, which still may be present, even if the organisms have been killed within the host, leading to a false positive result.
When a clinician suspects gonorrhea, he or she should take care with what site the specimen is being collected from, and what sample is specifically needed. This lab is validated for only certain types of specimens, and it is important to communicate with the clinicians to ensure the proper specimens are being submitted.
The CDC states that the optimal samples should be vaginal swabs for women, and first catch urine for men. Great care should be used when collecting the ‘first catch urine’ as this is a dirty catch, and that some tests have specific requirements about quantity. For instance, at this lab, we require no more than 30 ml of urine. Any more volume could dilute the specimen which could cause a false negative result.
If a culture is required in the event of treatment failure, it is best if the clinician innoculates the sample directly onto Thayer Martin agar (or chocolate agar if that is all that is available). Given that N. gonorrhoeae is such a labile organism, it need special media to grow, and great care must be taken with transport. This lab recomends inoculating onto the Jembec plates (Thayer Martin media with a CO2 pellet) allowing survival during transport.
N. gonorrhoeae inoculated directly onto the Jembec plateCultures can also be innoculated onto chocolate agar. Notice the smaller grey colonies, which is the N. gonorrhoeae. Notice the other colonies on the plate, as chocolate agar is not a selective medium.
In conclusion, although the majority of cases of gonorrhea treatment failure are likely to be due to re-infection, antibiotic resistance is still of growing concern and clinicians should know when a culture is necessary for antibiotic sensitivity testing. N. gonorrhoeae requires nutrient supplementation for growth, either on Thayer Martin media, or chocolate agar. Care must be taken when sampling and transporting the specimen. Clinicians also need to be aware of the requirements for sample collection for NAATs, as it is not always clear as to why one can’t simply run a test on a sample greater than 30 ml, or a clean catch urine.
-Rich Smith is a Pathology Student Fellow at University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
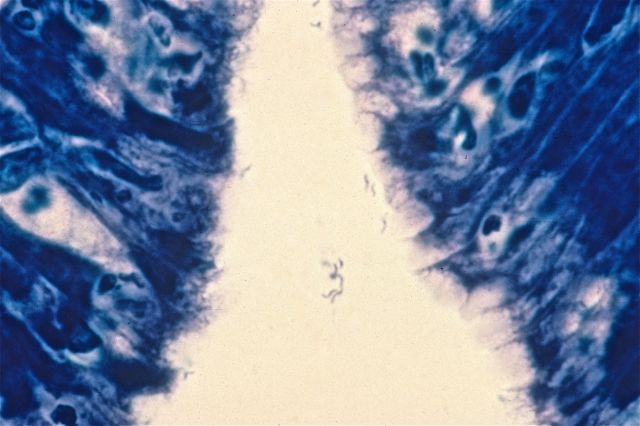
A 68 year old male presents with chronic, gnawing epigastric pain which has been getting worse over the past year. An endoscopy is performed and a representative gastric biopsy section, stained with Giemsa stain, is shown here. What organism is responsible for this patient’s symptoms?
A. Candida albicans
B. Helicobacter pylori
C. Bacillus cereus
D. Staphylococcus aureus
E. Campylobacter jejunum
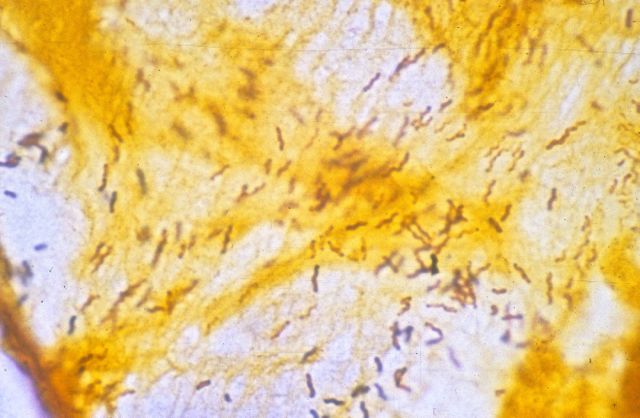
The diagnosis in this case is Helicobacter pylori. Described by Warren and Marshall in 1983, Helicobacter pylori is now known to be the cause of most cases of chronic gastritis and peptic ulcer. Helicobacter is a tiny, corkscrew-shaped bacillus, and is easily missed on routine H and E-stained histologic sections. Giemsa staining, as seen in the image above, can be helpful, as can silver staining, as seen in this image:
Helicobacter does not invade the gastric mucosa, but produces its symptoms through continual stimulation of the host immune response. Treatment involves triple therapy (e.g., omeprazole, amoxicillin and clarithromycin), and prognosis is excellent. A small number of patients, however, develop gastric adenocarcinoma or MALT lymphoma.
-Kristine Krafts, MD, is an Assistant Professor of Pathology at the University of Minnesota School of Medicine and School of Dentistry and the founder of the educational website Pathology Student.
An elementary school aged boy with a history of pre-B cell acute lymphocytic leukemia with a failed bone marrow transplant was transferred to a regional children’s hospital for leukodepletion and participation in an experimental clinical trial. At that time, his CBC was significant for 10% polymorphonuclear cells and 50% blasts. He was subsequently transferred to the ICU in respiratory failure and developed papulonecrotic lesions on his face, trunk, and bilateral legs. Prior to this, he was pancytopenic with no blasts present with cell counts of 100 WBC, hemoglobin 8.3 and 37,000 platelets. His Fungitell assay, which detects (1-3)-β-d-glucan, was positive.
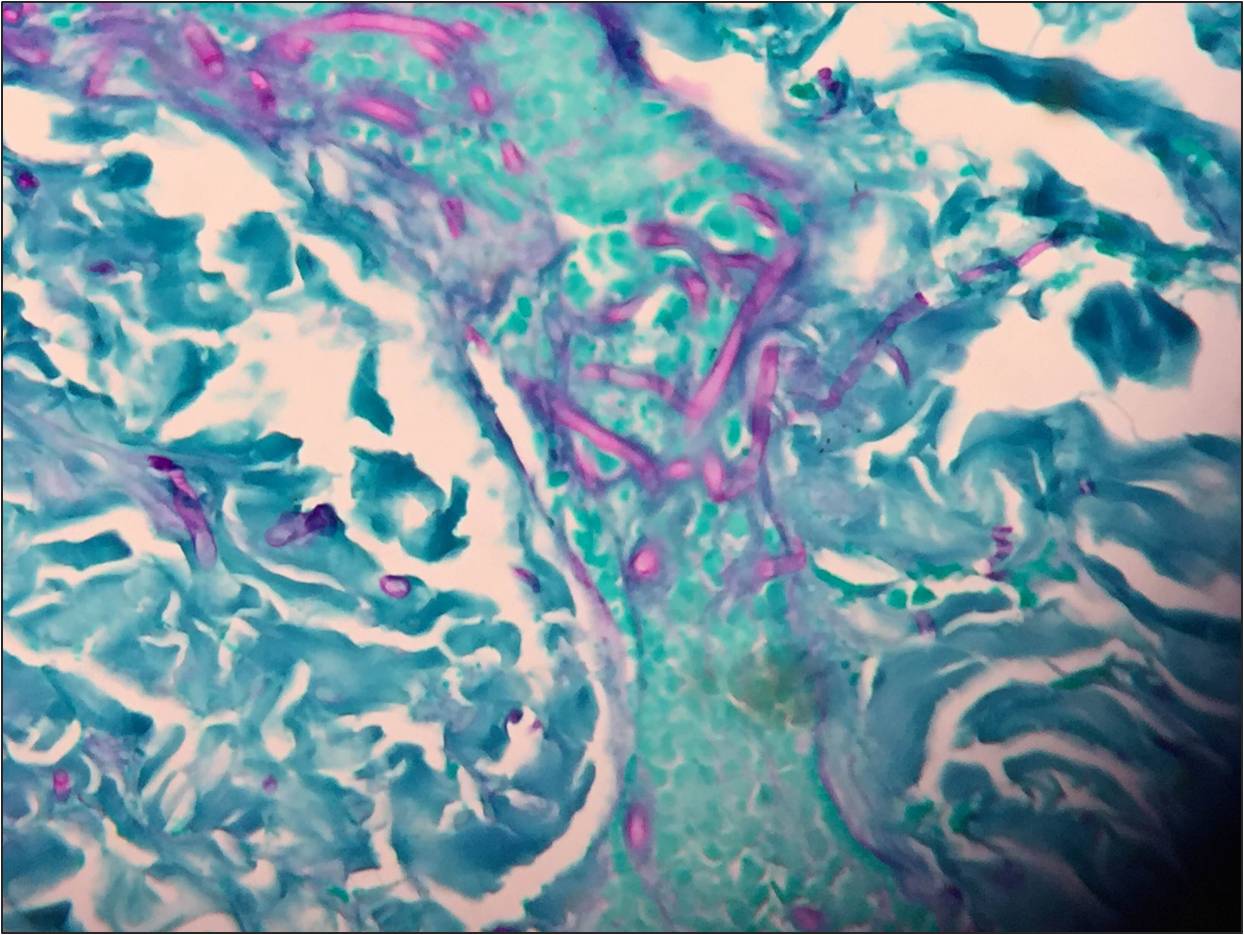
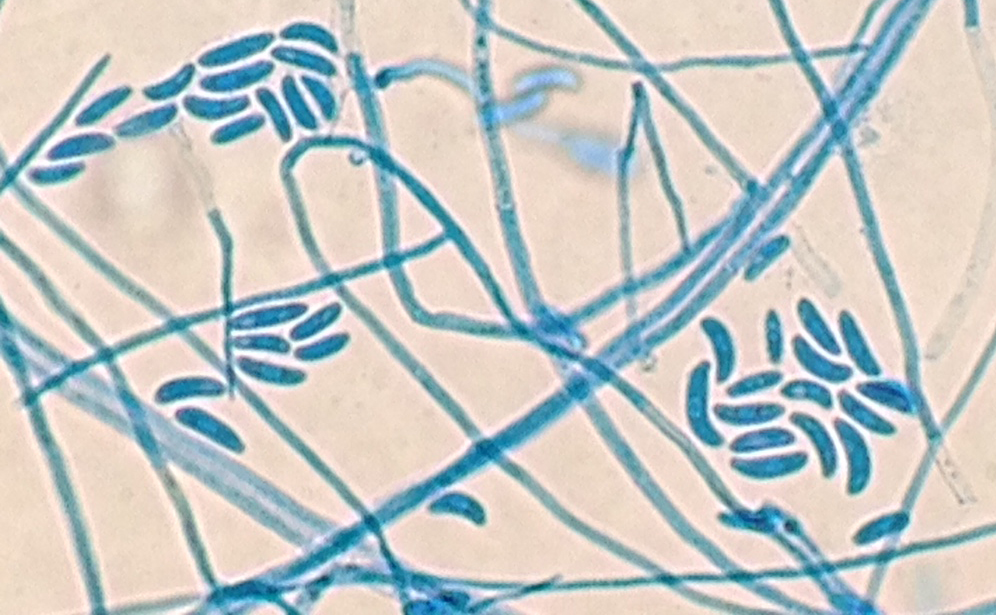
Routine blood culture, fungal culture from the endotracheal tube, and fungal culture from the skin lesion biopsy specimens all had fungal elements on KOH stain. Young growth of a whitish, fluffy mold was present on all cultures within two days. Histopathology on the punch biopsy of a skin lesion on the thigh showed septate hyphae within the dermis, epidermis, and invading the vasculature that was particularly apparent with GMS stain (Figure 1a and 1b). Within a few days, the fungal cultures showed septate hyphae with microconidia using lactophenol cotton blue tape preparation, and shortly thereafter the mold developed into macroconidia with multiple septations taking on canoe-like forms (Figure 2). The white, cotton-like colonies developed a pink tinge (Figure 3). These characteristics allowed for the identification of the growth as Fusarium sp.
Septate hyphae on GMS stained section of the skin punch biopsy.Septate hyphae on GMS stained section of the skin punch biopsy.Microscopic identification of Fusarium by lactophenol cotton blue stain.Colony of Fusarium growing on inhibitory mold agar (IMA).
Fusarium is an opportunistic hyaline mold with infection most commonly seen in immunocompromised hosts. It can cause keratitis through contamination of contact lenses, penetration due to trauma, or use of immunosuppressive steroid ophthalmic solution. It is increasingly becoming the cause of disseminated infection in neutropenic hosts with a broader spectrum of disease, which includes: skin lesions, fungemia, rhinocerebral involvement and pneumonia. In these cases, without an immune system to fight the infection, mortality is high. Inhalation of airborne conidia, ingestion from water sources or access through mucosal membranes are all potential points of entry.
The colony growth on plated fungal media is rapid, usually maturing within four days. On microscopic examination, Fusarium hyphae are septate, approximately 3-6 microns wide with acute angle branching. Microconidia are small, oval-shaped, and no larger than 4 x 8 microns in size. These can look like Acremonium sp. Macroconidia are canoe- or sickle-shaped with the largest dimension being about 80 microns in length, exhibiting 3-5 septatations.
–Jodi Music, MD, is an AP/CP resident at UT Southwestern Medical Center.
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
Case History:
A 76 year old female presents with a two year history of worsening upper back pain. Imaging revealed compression fractures of the first three thoracic vertebrae (T1-T3). Fine needle aspiration and a core biopsy of the T3 vertebral body were examined in surgical pathology. There was acute and chronic granulomatous inflammation with fungal organisms observed on histologic examination. Surgery for decompression and fusion of C5-T6 vertebrae was performed and tissue was sent for fungal culture.
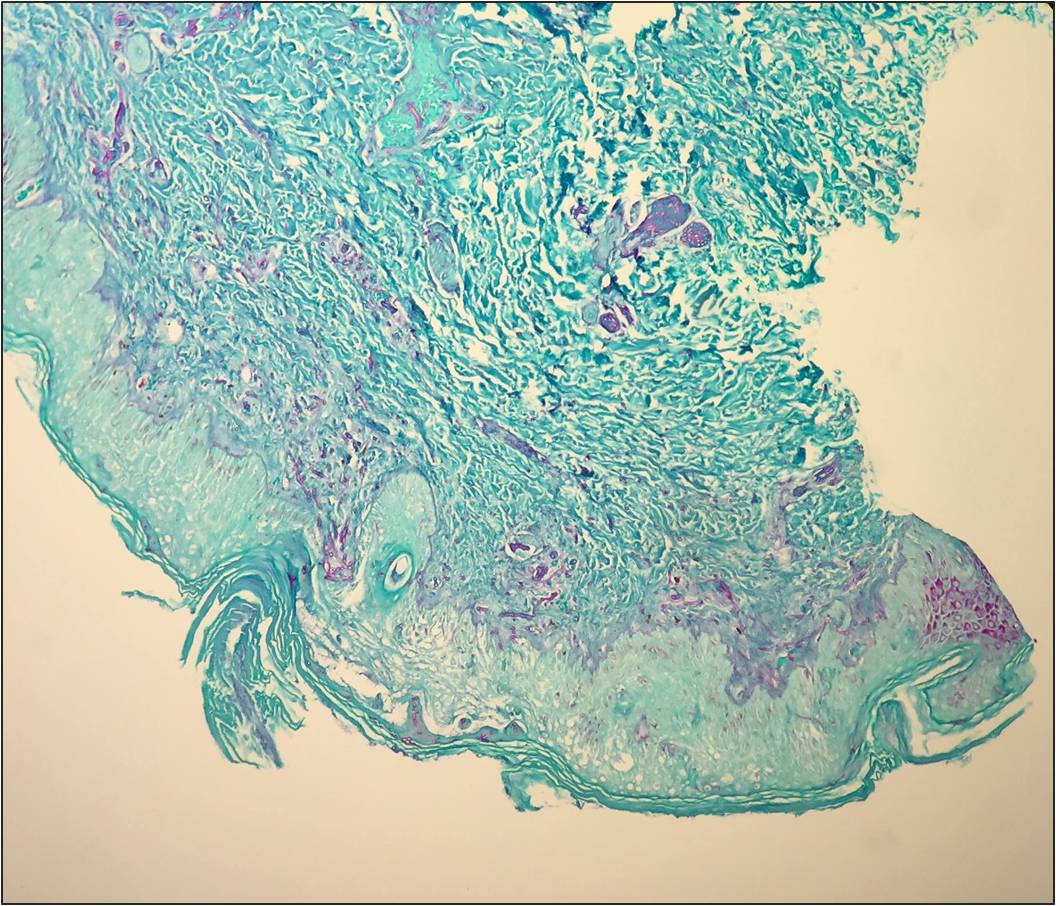
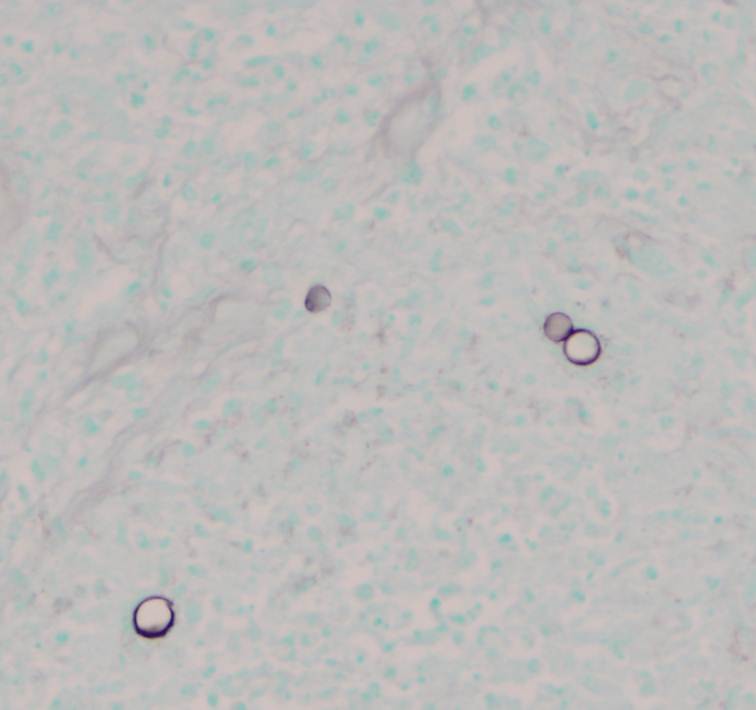
Potato flake agar shows a tan-brown fungus.Mycosel agar shows beige-white fungal growth.Scotch tape prep shows septate hyphae with unbranched conidiophores and single, terminal, “lollipop” conidia.Silver stain of involved bone with fungal organisms exhibiting broad-based budding.
Laboratory Identification:
The workup revealed a thermally dimorphic fungus with a mold form growing in the laboratory at 25°C and a yeast form present in the surgical pathology specimen. The mold form is moderately slow growing and has septate hyphae with small, round, terminal conidia often described as “lollipops.” The yeast form is large (8-15 microns) with broad based buds and double contoured cell walls. The immune system reacts to the presence of the fungus by forming granulomas and leads to acute and chronic inflammation within the involved tissue. The organisms can occasionally be seen within giant cells in histologic sections. The silver stain, as seen above, highlights the organisms.
Discussion:
The fungus described above exhibits the features of Blastomyces dermatitidis. This organism resides in soil and decaying plant matter and is endemic to eastern North America including the Mississippi and Ohio River Valleys as well as areas surrounding the Great Lakes and St. Lawrence River. The most common primary sites of involvement for Blastomyces are cutaneous and pulmonary. Following a primary infection, the disease can progress to disseminated blastomycosis which involves other sites such as bone.
The primary site of infection in this case is unknown. There was no history of cutaneous ulcers and chest imaging was unremarkable. The patient did have a remote history of bloody sputum production which she had attributed to “dental difficulties” that she was experiencing and has since resolved. This may have been evidence of a primary pulmonary infection preceding the vertebral involvement; however it is difficult to say with certainty.
The classic double contoured cell walls are not evident on the silver stain of the surgical pathology specimen in this case. This may be due to the fact that the bone required decalcification before histologic sections could be taken. The decalcification process may have caused an artifactual loss of the double contour. Despite the fact that this classic finding was not seen, the macroscopic and microscopic morphology is most consistent with Blastomyces.
The patient is being treated with long-term itraconazole and is currently doing well.
-Britni Bryant, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Just in time for Halloween: a recently-published study in mBio discusses the 2014 outbreak of Listeria monocytogenes tied to caramel apples. There’s not enough water in caramel and an apple is too acidic to support this bacterium, so how did this outbreak occur? From the study: “Our findings suggest that the 2014 listeriosis outbreak associated with caramel-coated apples can be explained by growth of L. monocytogenes occurring at the interface between two foods which, by themselves, are inhibitory to pathogen growth.”
Case history:
An 18 year old pregnant woman at 16 weeks gestation presented at the emergency department with nausea and vomiting for 3 days. Three days ago she and some of her friends ate chicken at a party. None of her friends experience her symptoms. Laboratory tests revealed urinary tract infection and a stool sample was sent to the microbiology laboratory for culture.
She was prescribed an antibiotic and was released from the ED.
Laboratory identification:
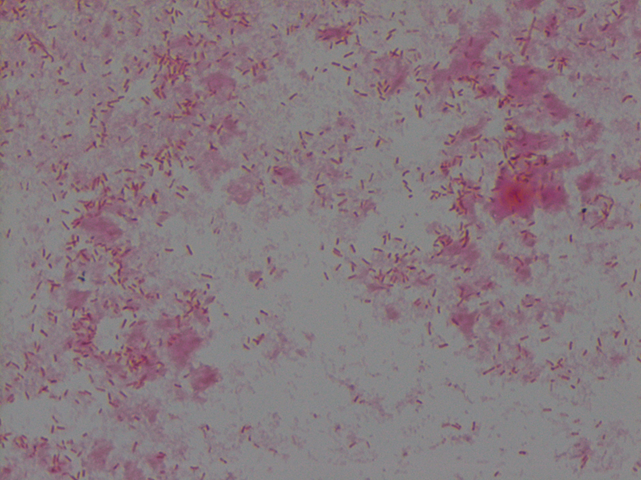
The organism grew well on MacConkey agar, and formed small colorless lactose-negative colonies. Gram stain revealed short gram-negative bacilli and MALDI-ToF confirmed the bacteria as Yersinia enterocolitica.
Non-lactose fermenting, flat colonies on MacConkey agarGram stain of Yersinia enterocolitica reveals Gram-negative bacilli
Discussion: Yersinia enterocolitica is a gram negative, short, non-spore-forming bacillus in the family Enterobacteriaceae. They can exhibit bipolar staining, especially from the primary sample. It is a facultative anaerobe can grow at temperatures ranging from 4-43oC that is motile at room temperature but non-motile at 37oC. The organism grows well on MacConkey agar, and forms small colorless lactose-negative colonies but if the clinical team is suspicious for Yersinia, a selective growth medium is recommended. The most widely used is cefsulodin-irgasin-novobiocin (CIN) agar, which inhibits the growth of competing flora and produces characteristic colony morphology (red color with “bull’s eye” appearance).
The major route of Y. enterocolitica infection is through contaminated foods or water. The primary pathogenic event is colonization of the intestinal tract where most of the pathologic effects and clinical manifestations occur. Temperature and calcium concentration regulate expression of virulence factors that guide the invading Yersinia and allow them to survive and disseminate.
The most common form of disease caused by Y. enterocolitica is gastroenteritis associated with consumption of contaminated food or water, especially raw or undercooked pork such as chitterlings. Disease can range from self-limited gastroenteritis to terminal ileitis and mesenteric lymphadenitis that can be misdiagnosed as appendicitis. Gastrointestinal infections are usually self-limiting and do not merit antimicrobial therapy. However, in immunocompromised hosts and in patients with septicemia or invasive infection, the mortality can be high (approximately 50%).
Kossivi Dantey, M.D. is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
–Christi Wojewoda, MD, is certified by the American Board of Pathology in AP/CP and Medical Microbiology. She is currently the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Antibiotic resistance is a huge concern for microbiologists. In addition to stewardship programs and regulating agricultural use of antibiotics, is it time to re-examine clinical testing paradigms?
A recent study suggests that the typical way microbiologists test for antibiotic susceptibility–meuller-hinton plates and antibiotic disks–might be fallible. When his team tested Salmonella against polymyxin using typical methods, the organism tested sensitive; when the tested the same organism against the same antibiotic using medium that more closely resembled human cells, the organism tested resistant.
Bloomberg Business discusses the paper here. The article is worth your time, even if the info-graphic gives erroneous information (it mentions meuller-hinton broth instead of meuller-hinton agar plates).
An 8 week old female was brought to an outside hospital due to pallor, decreased eating over several days, vomiting, fever, and blue color in the feet. The patient had received her two month vaccinations the day prior to presentation. Her past medical history was significant for being born at 32 weeks gestation, followed by an uneventful 4 week NICU stay. At the outside hospital the patient was in respiratory distress, tachycardic, with pallor. She was intubated and transferred to our institution due to concern for an ALTE (apparent life-threatening event). Blood and CSF specimens were drawn. Upon presentation, the patient had a white blood cell count of 19,600/mm3. Her CSF had 63 nucleated cells/mm3 (30% neutrophils, 49% lymphocytes, 11% monocytes), glucose of 23 mg/dL and protein of 212 mg/dL. Blood and CSF cultures were performed with the following results:
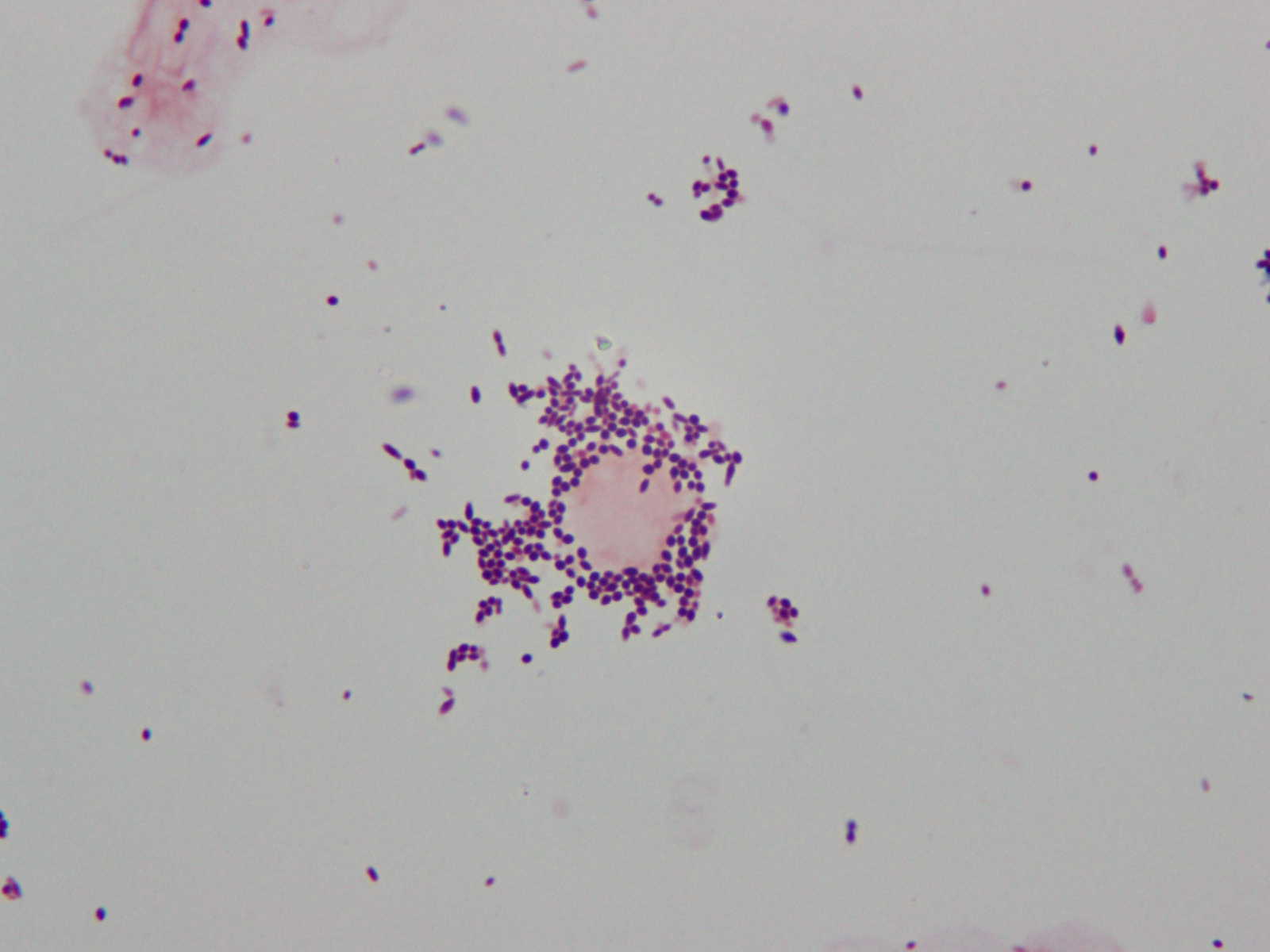
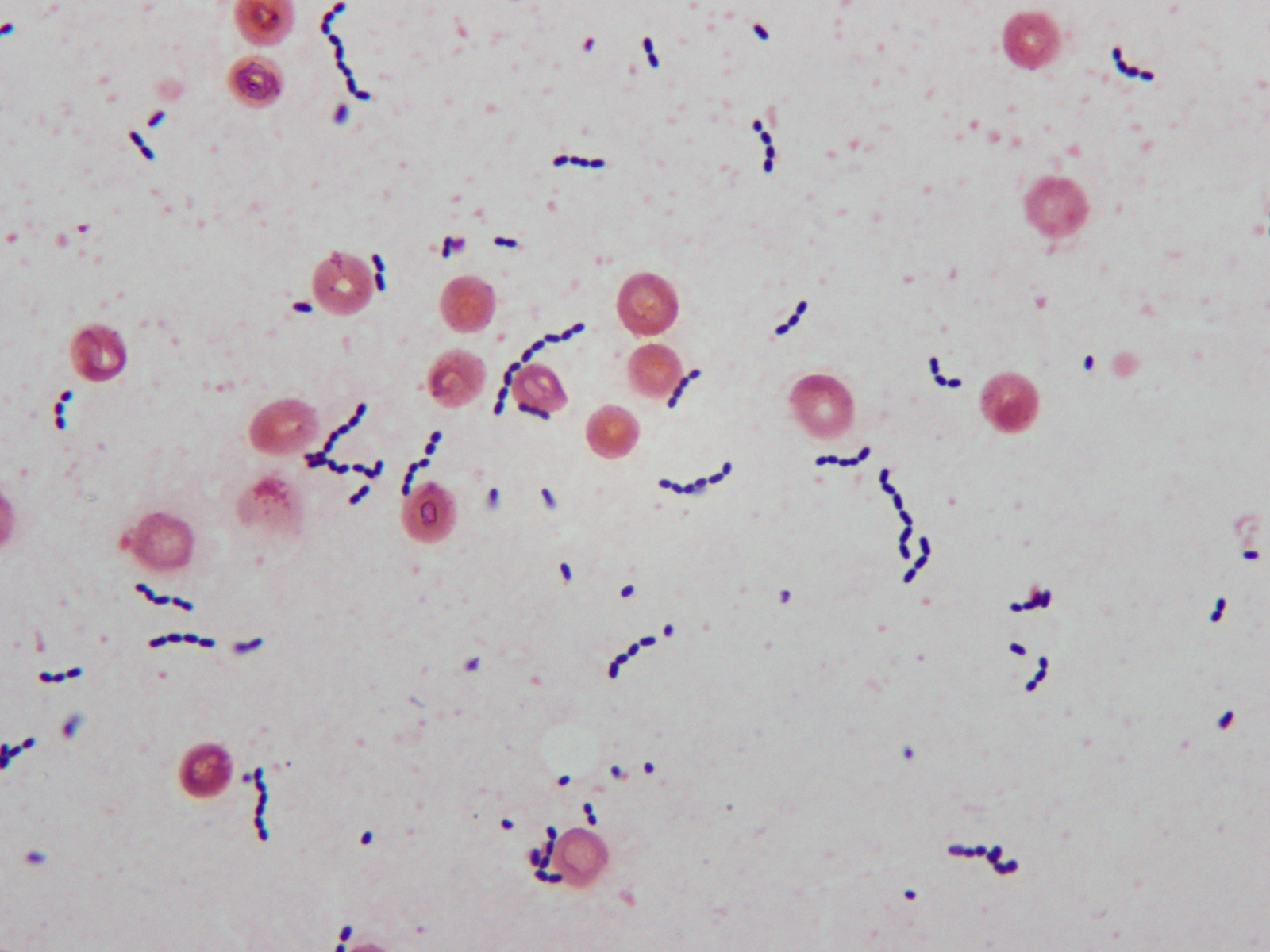
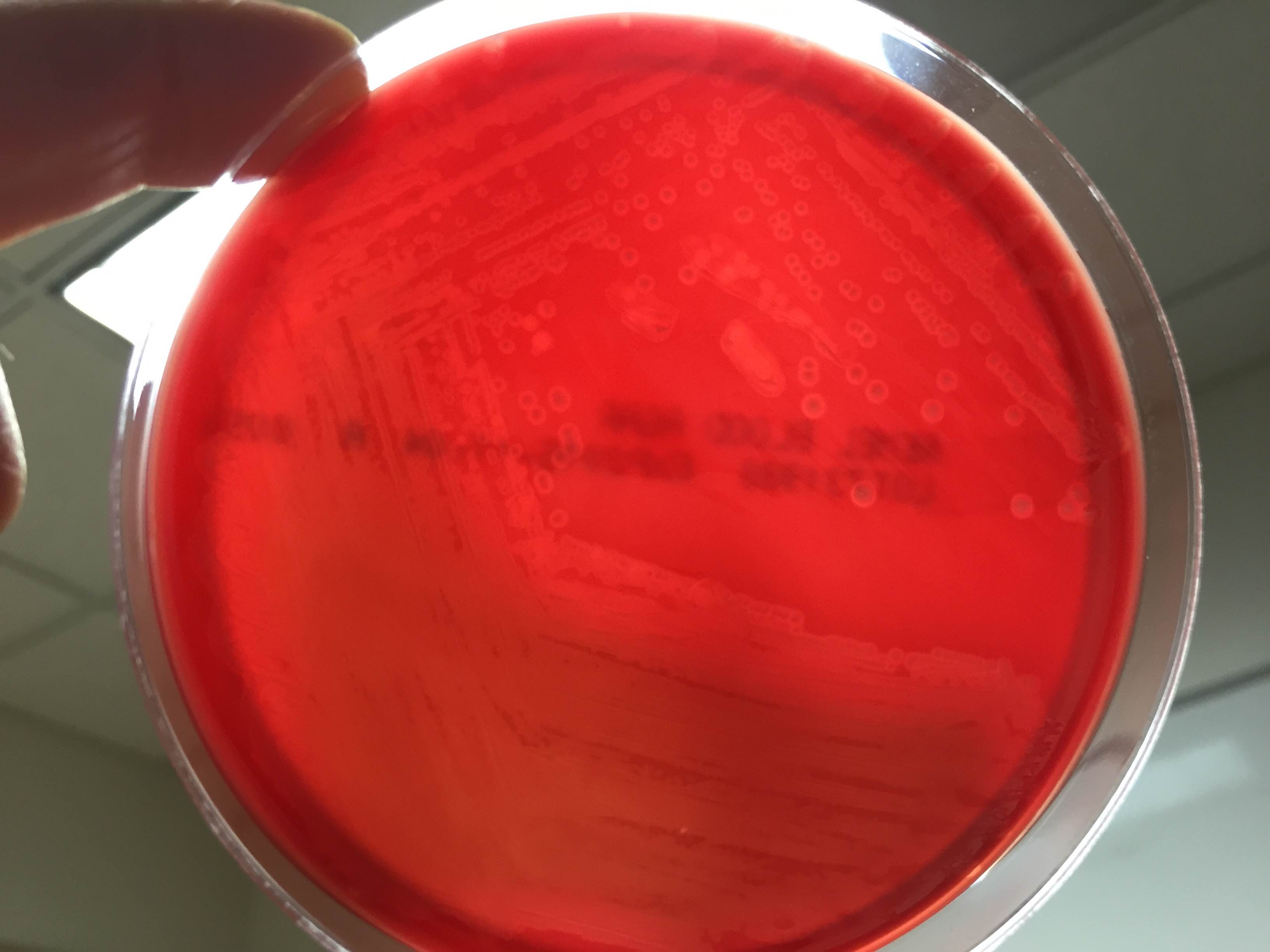
Gram stain of cerebral spinal fluid (CSF) specimen showing Gram positive cocci in singles and pairsGram stain of positive blood culture broth showing Gram positive cocci in chainsSmall zones of beta hemolysis around colonies growing on 5% sheep blood agar
Laboratory Identification
CSF Gram stain was read as many Gram-variable coccobacilli (Image 1) and blood culture Gram stain was resulted as Gram-positive cocci in pairs and chains (Image 2). The Nanosphere Verigene Gram-positive blood culture molecular assay was performed on the positive blood culture broth immediately following Gram staining. CSF and positive blood culture specimens were plated to 5% sheep blood, chocolate, MacConkey, and CNA agars. In >24 hours colonies from both specimens grew a single organism on sheep blood, chocolate, and CNA agars. On blood agar, colonies exhibited a soft zone of b-heomlysis (Image 3). Colony Gram stains showed Gram-positive cocci in chains, catalase testing was negative, and the organism typed in Lancefield antigen group B. Verigene identified the organism directly from the positive blood culture broth as Streptococcus agalactiae (aka Group B Streptococcus or GBS) and MALDI-TOF mass spectrometry confirmed the identification of S. agalactiae.
Discussion
Laboratory Considerations
As our CSF specimen demonstrated, streptococci can be difficult to interpret from specimen Gram stains. Organisms are often are pleomorphic in size and shape and they have a tendency to stain Gram-variable. This lead to the report of Gram-variable coccobacilli on our patient’s CSF culture.
S. agalactiae produces a soft zone of b-heomlysis on sheep blood agar. Unlike Streptococcus pyogenes (aka Group A Streptococcus) which produces a wide zone of b-hemolysis, soft b-hemolysis can often be very subtle, especially with young growth. Soft zones b-hemolysis can best be seen by holding plates up to a light source or my moving a colony out of the way to observe if hemolysis is present underneath. The pattern of S. agalactiae b-hemolysis is very similar to that produced by Listeria monocytogenes. Streptococcal isolates that type as Lancefield Group B, but produce large zones of b-hemolysis can create confusion and are most likely not S. agalactiae, but S. porcinus or S. pseudoporcinus.
Clinical Significance
S. agalactiae is the cause of significant neonatal disease. Early-onset infection presents as systemic infection, respiratory distress, apnea, shock, and pneumonia within the first 24 hours of life (range, 0–6 days). Meningitis is less common in early-onsetS. agalactiae infections, found in just 5-10% of cases. Late-onset disease presents at 3 to 4 weeks of age (range, 7–89 days) as meningitis and/or sepsis with other focal infection. Approximately 50% of survivors of early- or late-onset meningitis have long-term neurologic sequelae.
S. agalactiae colonizes the urogenital or gastrointestinal track of 10-30% of pregnant women. Being born to a S. agalactiae colonized mother is the most significant risk factor for development of disease in neonates. For this reason, women are screened for “Group B Strep” colonization between 35 and 37 weeks of pregnancy. Women found to be colonized receive prophylactic antibiotics immediately prior to delivery to prevent transmission to the child. Since implementation of these practices in 1996, there has been a substantial decline in early-onset S. agalactiae infections. Interestingly, these measures have not affected the incidence of late-onset disease.
Treatment
Until recently S. agalactiae was considered universally susceptible to penicillin. There have now been a few reports of S. agalactiae isolates with increased penicillin MICs due to mutations in the penicillin binding protein Pbp2x. The detection of these isolates is still extremely rare, so much so that S. agalactiae susceptibility testing for penicillin and other b-lactams is not considered necessary at this time. Penicillin and its derivatives are the preferred treatment option.
Patient follow-up
Our patient had a complicated course of late-onset Group B Streptococcal meningitis including multifocal cerebral infarctions and seizures. She was treated with a 28 day course of ampicillin. Blood cultures taken 24 hours after the start of antibiotics were negative and her CSF culture was negative when rechecked 5 days after her presentation. Due to her complicated course, the patient was hospitalized for 4 weeks. Follow-up appointments have shown the patient’s MRI is nearly normal 8 weeks post infection and the patient is doing well, although she is still followed by neurology to assess for long term sequelae.
Our patient’s mother had an unknown Group B Strep carrier status at the time of her birth, as she was born at 32 weeks, which is before routine screening occurs for pregnant women. Either way, the mother’s status would not have affected the patient’s risk for late-onset Group B Streptococcal infection.
References:
Red Book 2015
Journal of Clinical Microbiology, 10th edition
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.