A 74 year old female presented to the ED with a chief complaint of fever, right knee swelling and pain for three days. Past medical history was significant for a right total knee arthroplasty approximately 5 months prior, with no significant complications. Physical exam revealed the patient to be febrile (103 degrees Fahrenheit), a swollen right knee that was warm to the touch and erythema surrounding the surgical incision site. Routine labs were obtained while in the ED which revealed a leukocytosis with an elevated ESR and CRP. Imaging was ordered and showed a large joint effusion of the right knee with intact hardware. Arthrocentesis was performed which returned 80 cc of cloudy yellow fluid with no crystals identified by light microscopy, a nucleated cell count of 169,200/cmm of which 97% were neutrophils.
Laboratory Identification
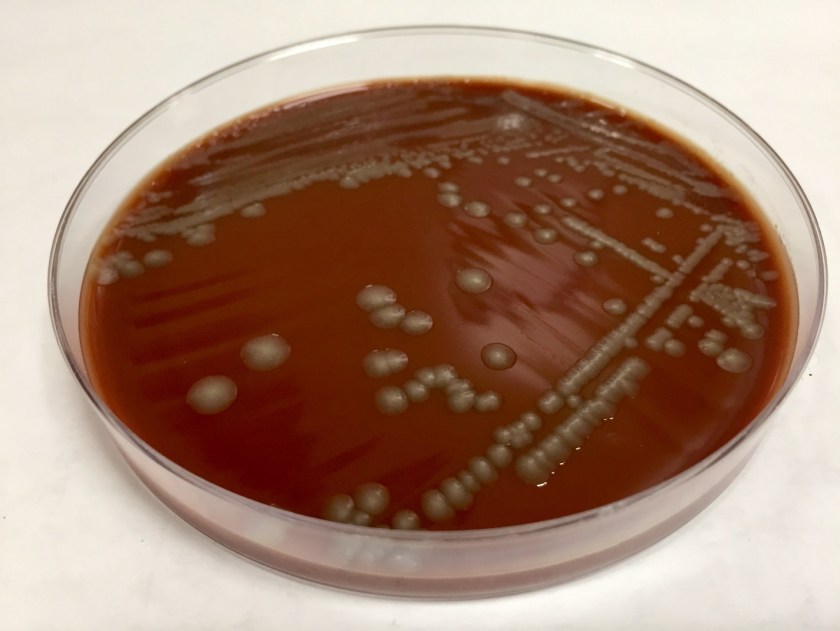
The primary gram stain was reported as polys and gram negative bacilli present. Cultures revealed a pure moderate growth on sheep blood and chocolate agar with no growth on the MacConkey agar. Colony morphology on the sheep blood agar was smooth, gray with no hemolysis appreciated. The key biochemical and physiologic characteristics of the isolate included: positivity for indole, nitrate reduction, catalase, ornithine decarboxylase, and fermentation of mannitol and sucrose; negativity for urea and maltose fermentation. The isolate was identified by MALDI-TOF as Pasteurella multocida. Upon further questioning, the patient admitted to living with two indoor cats but denied any recent history of bites or scratches.
Image 1. Chocolate agar with smooth gray colonies.
Discussion
Pasteurella multocida is a non-motile, oxidase positive, small -gram negative bacilli capable of fermenting glucose. This organism is part of the normal flora of the gastrointestinal tract and nasopharynx of wild and domestic animals. Humans who have extensive exposure to animals may be found to have Pasteurella multocida as part of their upper respiratory tract flora. With no significant virulence factors, this organism is often viewed as an opportunistic pathogen which requires mechanical disruption of anatomic barriers as occurs with bite and scratch wounds from cats and dogs. Though most infections are associated with bites or scratched from animals, infection can occur with non-bite exposure to animals. The typical disease caused by Pasteurella multocida is a focal soft tissue infection following a bite or scratch. However, chronic respiratory infections in patients with preexisting chronic lung disease and heavy animal exposure, and bacteremia with metastatic abscess formation have been documented.
Biochemical characteristics can be utilized in identifying the different Pasteurella species. The key biochemical and physiologic characteristics for Pasteurella multocida include: positivity for indole, nitrate reduction, catalase, ornithine decarboxylase, and fermentation of mannitol and sucrose; negativity for urea and maltose fermentation.
The vast majority of these organisms are susceptible to penicillin, thus susceptibility testing is generally unnecessary. Additionally, soft tissue infections caused by animal bites are frequently polymicrobial and warrant use of therapeutics with a broader spectrum. However, should the need arise to perform susceptibility testing, the Clinical and Laboratory Standards Institute (CLSI) does provide break points for Pasteurella multocida.
Koneman EW. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology. Lippincott Williams & Wilkins; 2006.
-Justin Rueckert, DO is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 62 year old Caucasian male was referred to the gastroenterology clinic with complaints of epigastric pain, diarrhea and unintentional weight loss over the past couple of weeks. Travel history was significant for a recent mission trip to rural areas of the Philippines. During his time there, he participated in building chicken coops and scuba diving. He reported he mostly ate pork & vegetables but did note he consumed a “runny, undercooked duck egg.” He did not eat any seafood during the trip. About a month after his return, he developed epigastric pain and clinically significant diarrhea, with anywhere from 2-8 bowel movements per day. Testing for blood counts, hepatitis and HIV was performed and stool was collected for culture and ova & parasite exam (O&P). He also underwent a colonoscopy with multiple biopsies.
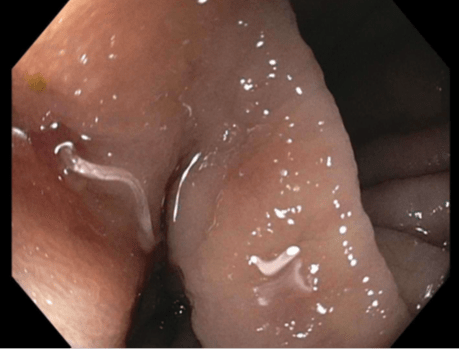
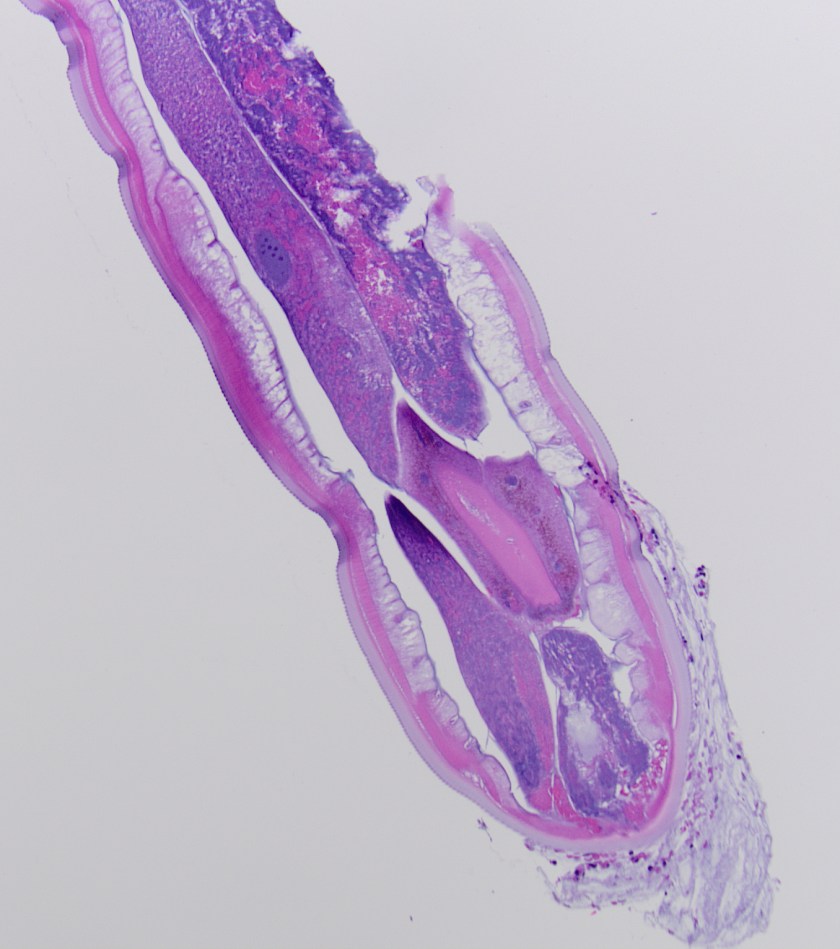
Image 1. During colonoscopy, the mucosa of the cecum was erythematous with small areas of ulceration and multiple helminths were noted.Image 2. Histologic section of an adult helminth showed a thick cuticle with annulations, thin hypodermis and a layer of somatic muscle cells (H&E, 100x).Image 3: Histologic section of a female helminth with numerous barrel shaped eggs identified (H&E, 400x).
Laboratory Identification
CBC revealed a white blood cell count of 17.9 TH/cm2 with 63.5% eosinophils. Acute hepatitis panel and HIV screen were negative as were two sets of stool cultures and O&Ps. Colonoscopy showed multiple helminths at the ileo-cecal junction (Image 1) and histology of the worms revealed architecture and eggs consistent with Trichuris trichiura (Images 2 & 3).
Discussion
Trichuris trichiura is classified as a nematode (roundworm) and is the third most common round worm causing disease in humans. It has a worldwide distribution and infections are most frequent in areas with tropical climates and resource poor settings with inadequate sanitation practices, especially among children. It is estimated that 800 million people are infected worldwide. While most cases diagnosed in the United States occur in immigrants, travelers and military personnel, T. trichiura has also been documented in the southern United States. Clinical presentations are most frequently asymptomatic or mild. Heavy infections, especially in small children, can cause gastrointestinal problems (abdominal pain, diarrhea, rectal prolapse) and possibly growth retardation due to prolonged malnutrition and anemia.
Infection occurs when embryonated eggs are orally ingested with soil contaminated food & water or due to poor hygiene practices. T. trichiura larvae are released in the small intestine and then travel to the colon where they develop into adult forms. Females begin to produce large volumes of eggs (up to 20,000 per day) about 2-3 months after initial infection. Unembryonated eggs are passed in the stool and in warm, moist soil conditions become infective in 15-30 days.
In the laboratory, diagnosis of T. trichiura is most commonly made by identification of the barrel shaped egg with mucous plugs at either end. The eggs have a double shell and are approximately 50-55 um in length. For increased sensitivity, it is recommended that multiple stool specimens for O&P be collected over the course of 7-10 days as shedding is sporadic. Occasionally, adult worms are visualized on colonoscopy and have a long, thin anterior end which attaches to the mucosa and a thicker posterior portion giving the worm a “whip” like appearance. Adult worms typically measure between 3 to 5 cm in length.
Whipworm infections are routinely treated with albendazole or mebendazole. In the case of our patient, he received multiple doses of albendazole and responded well with resolution of symptoms.
-Joy King, MD, is a fourth year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
We recently had a case that made me stop to think about the lengths we sometimes have to go to understand what the bacteria are trying to teach us.
The Issue
Not only are there several methods for the detection of oxacillin resistance in staphylococci (1,2,3), but many laboratories employ a variety of those methods (image 1). This can be a blessing…or a curse. Blessing: alternate methods can be used to referee discordant results. Curse: testing additional methods may cause more confusion. To quote Frank Lloyd Wright, “Less is more only when more is too much.”
The mecA gene encodes for the alternate Penicillin Binding Protein 2a (PBP2a), which confers resistance to oxacillin. In recent years, cefoxitin has become the preferred surrogate for oxacillin to detect methicillin resistance (1, 2). Moreover, as molecular methods become more widely adopted, we open ourselves up to scenarios where the genotype does not match the phenotype. Depending on how your laboratory reports these results, it can be confusing to clinicians. All they want to know is, “Is this MRSA, or not?”
When molecular and culture results do not agree
Many laboratories have turned to polymerase chain reaction (PCR) assays to detect MRSA because of its rapid time to result and its superior sensitivity (compared to AST and PBP2a testing). Recent advances in technology allow for the detection of MRSA direct from positive blood cultures. Rapid organism identification and detection of resistance markers greatly improve patient care by reducing the time to appropriate antimicrobial therapy. However, the problem occurs when the PCR result does not match the PBP2a and/or AST results.
In our laboratory, when a blood culture flags positive the bottles are removed from the automated instrument, a Gram stain is performed, the specimen is subcultured (blood, chocolate, and MacConkey agars) and analyzed (if appropriate) by a multiplex PCR. This workflow allows us to report organism identifications on the majority of our blood cultures on day one of the culture flagging positive (image 1). Final AST results are usually reported by day three. Of note, additional steps are added depending on the Gram stain result. For example, if the Gram stain reveals gram-positive cocci in clusters (GPCL) suggestive of Staphylococcus, then we will also drop a cefoxitin disk onto the blood agar plate.
For this particular case, on day one the Gram stain revealed GPCL and the PCR assay detected S. aureus and mecA, which indicated that the patient had MRSA bacteremia. Nothing out of the ordinary. On day two, we confirmed the culture was S. aureus, but the PBP2a result was negative. Unfortunately, the cefoxitin disk was missed when the culture was originally subcultured (image 2A). Normally, we perform PBP2a testing from cefoxitin-induced growth around the zone of inhibition, but that did not occur in this case. Because the PBP2a and PCR results were discordant, the blood culture was subcultured again to include the cefoxitin disk (image 2B).
The Solution
Image 2A shows a homogenous culture of S. aureus. Under examination no differences could be detected among the colonies; it appears to be a pure culture. Image 2B shows that the culture is actually a heterogeneous culture with both MRSA and MSSA. There are two zones of inhibition around the cefoxitin disk. The white circle highlights the cefoxitin-resistant population and the blue circle highlights the susceptible population. The isolated colonies in the third quadrant look identical; one cannot distinguish between the two populations. This example displays the heterogeneous nature of S. aureus in terms of resistance, or rather its “heteroresistance” to oxacillin and the complexity involved in detecting MRSA.
For those that use phenotypic assays, the use of a cefoxitin disk can help improve your detection rates. Because cefoxitin is both a surrogate for oxacillin resistance and a strong beta-lactamase inducer, it is the perfect aid to enhance MRSA detection (image 2). For this reason, our laboratory implemented the addition of the cefoxitin disk to positive blood cultures with GPLCs. Because we had a few false-negative PBP2a MRSA cases, we decided to start performing PBP2a testing on cefoxitin-induced growth. This intervention has helped two-fold. First, it has seemingly reduced the number of false-negative results. Second, the zone of inhibition functions as an internal control. If the zone is small or non-existent, then it seems obvious that isolate should be resistant. If the zone is large, then we would expect the isolate to be susceptible. Moreover, if we see a double zone as in image 2A, then the culture is likely mixed. [As an aside, we once had a case where the mecA gene detected was from a coagulase-negative Staphylococcus and not the S. aureus (MSSA) that was also present in the culture.]
Image 1. S. aureus workflow. From the time the specimen comes into the laboratory, it can take anywhere from one to three days before a provider knows if their patient has methicillin-susceptible S. aureus (MSSA) or MRSA. MRSA isolates are multidrug-resistant, which require broad-spectrum antibiotics, such as vancomycin (3). For patients with MSSA, narrow-spectrum beta-lactam antibiotics, such as nafcillin or cefazolin are not only the first-line therapy, but superior in terms of outcomes compared to vancomycin (4). Also, patients with MRSA may be put in isolation depending on your institution’s infection control protocol. More importantly, delay of appropriate antibiotics can significantly increase mortality, especially in the case of sepsis (5).Image 2. Cefoxitin induces methicillin resistance. A) A positive blood culture was subcultured to blood agar (no cefoxitin disk). B) The same positive blood culture was subcultured with a cefoxitin disk (30 mg). FOX= cefoxitin. Recall that cefoxitin is a surrogate for oxacillin, therefore resistance to either (oxacillin or cefoxitin) denotes resistance to methicillin.
The Conclusion
Depending on the S. aureus isolate, the detection of methicillin resistance can be a challenge regardless of which method(s) your laboratory utilizes. Fortunately, there is a clear-cut solution. CLSI recommends that isolates should be reported as MRSA if oxacillin resistance is detected by any method (1, 2).
As you saw from our case, the phenotype did actually match the genotype. A combination of heteroresistance and human error (un-induced growth for PBP2a) led us astray. As you read this, you may be thinking, “why did they do all of that?” Good question! We felt that this was a good case to teach and/or learn. “Smart people learn from their mistakes. Geniuses learn from others.” If this can help others learn, then it is all worth it. My gift to you. Merry Christmas!
References
Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; approved standard- tenth edition. CLSI document M07-A10. Wayne, PA: Clinical and Laboratory Standards Institute; 2015.
Performance standards for antimicrobial susceptibility testing. CLSI document M100-S27. Wayne, PA: Clinical and Laboratory Standards Institute; 2017.
Centers for Disease Control and Prevention (CDC). Methicillin-resistant Staphylococcus aureus (MRSA). https://www.cdc.gov/mrsa/lab/index.html. Accessed December 18, 2017.
Schweizer, M.L., Furano, J.P., Harrris, A.D., Johnson, J.K., Shardell, M.D., McGregor, J.C., Thom, K.A., Cosgrove, S.E., Sakoulas, G. and Perencevich, E.N. (2011). Comparative effectiveness of nafcillin or cefazolin versus vancomycin in methicillin-susceptible Staphylococcus aureusBMC Infect. Dis. 11:279. doi: 10.1186/1471-2334-11-279
Kumar, A., Roberts, D., Wood, K.E., Light, B., Parrillo, J.E., Sharma, S., Suppes, R., Feinstein, D., Zanotti, S., Taiberg, L., Gurka, D., Kumar, J. Cheang, M. 2006. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Care Med. 34:1589-1596. doi: 10. 1097/01.CCM.0000217961.75225.E9
-Raquel Martinez, PhD, D(ABMM), was named an ASCP 40 Under Forty TOP FIVE honoree for 2017. She is one of two System Directors of Clinical and Molecular Microbiology at Geisinger Health System in Danville, Pennsylvania. Her research interests focus on infectious disease diagnostics, specifically rapid molecular technologies for the detection of bloodstream and respiratory virus infections, and antimicrobial resistance, with the overall goal to improve patient outcomes.
A 57 year old male presented to the ED with the chief complaint of fever (103 degrees Fahrenheit), urinary retention, backache and headache. The patients past medical history is significant for penile cancer status post total penectomy with perineal urethrostomy and pelvic lymph node dissection approximately 12 months prior, recent urinary tract infection (2 weeks prior, treated with 7days of antibiotics), recent pace maker placement (2 months prior), Group B Streptococcus cellulitis of the left leg complicated by bacteremia (7 months prior). The patient requires use of in and out catheters for urination as a result of the penectomy and perineal urethrostomy; however he has had difficulty with catheterization recently secondary to urethral stenosis.
Physical examination revealed the right inner thigh to be erythematous, warm, and mildly tender, clinically consistent with cellulitis. The cellulitis appeared to be spreading along the medial aspect of the thigh and involving the lower leg. While in the ED, two sets of blood cultures were obtained and a urinalysis was significant for 1+ blood, 1+ nitrite, 1+ leukocyte esterase. He was subsequently treated with intravenous fluids and ceftriaxone and admitted to the hospital.
Laboratory Identification
Both sets of the blood cultures were positive (3/4 bottles), with the first bottle being positive after 11 hours of incubation. Gram smears of the bottles revealed the presence of gram positive cocci resembling Streptococcus. Per laboratory procedure, the positive bottles were analyzed utilizing the Luminex Verigene platform and resulted as Streptococcus species. The blood culture broth was subcultured to sheep blood agar and revealed a pure isolate of medium sized slightly opaque gray colonies with a large zone of beta hemolysis. The bacteria were found to be catalase negative and PYR negative. The organism was identified by a latex agglutination assay as Group C streptococci.
Image 1. Sheep blood agar plate with beta hemolytic colonies.
Discussion
Group C streptococci designates Streptococcus species which react with Lancefield group C typing serum. Group C streptococci are comprised of several different Streptococcus species including S. dysgalactiae subspecies equisimilis, S. dysgalactiae subspecies dysgalactiae, S. equi subspecies equi, and S. equi subspecies zooepidemicus. The most commonly isolated species in human clinical specimens is S. dysgalactiae subspecies equisimilis. Group C streptococci are considered normal flora of human skin, nasopharynx, gastrointestinal tract and genital tract. The mode of transmission for these organisms includes endogenous isolates gaining access to sterile sites and person to person transmission. No definitive unique virulence factors have been identified to date; however similar virulence factors to those of S. pyogenes and S. agalactiae are likely. The diseases caused are similar to those caused by S. pyogenes and S. agalactiae including bacteremia, endocarditis, arthritis and skin and soft tissue infections. Disease generally occurs in patients in immunocompromised states or with multiple comorbidities. There have been documented cases of zoonotic infections with S. equi subspecies zooepidemicus in patients with farm animal exposure, however not all infections are associated with animal exposure. S. equi subspecies zooepidemicus is a causative agent of bovine mastitis and has been documented as the etiologic agent in several outbreaks attributed to ingestion of inadequately pasteurized dairy products. Group C streptococci are susceptible beta-lactam antibiotics, and penicillin is considered the drug of choice for treatment.
Koneman EW. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology. Lippincott Williams & Wilkins; 2006.
Pelkonen S, Lindahl SB, Suomala P, et al. Transmission of Streptococcus equi subspecies zooepidemicus infection from horses to humans. Emerging Infect Dis. 2013;19(7):1041-8.
-Justin Rueckert, DO is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 62 year old male without a significant past medical or smoking history was referred to pulmonology for an abnormal chest CT. Three months prior to presentation, the patient had developed a cough after doing some home remodelling that involved sanding drywall. The cough became severe and blood-tinged, including some clots, so the patient sought medical attention. The patient denied any other symptoms and reported feeling well overall. Physical exam findings were all within normal limits. A chest X-ray showed a round lesion in the left lower lobe. Follow-up chest X-rays showed that the lesion had decreased in prominence but had not resolved. Subsequently, a chest CT was performed that showed a 2.8cm mass-like focal area of consolidation in the left lower lobe without associated lymphadenopathy. Because malignancy could not be excluded, the patient underwent bronchoscopy with biopsies obtained for cytopathologic evaluation as well as mycobacterial and fungal cultures.
Image 1: Cytologic preparation (alcohol-fixed, Papanicolaou-stained) of lung, left lower lobe, 2.8cm mass, fine needle aspiration.
The cytologic preparation of fluid from a fine needle aspiration (Image 1) shows granulomatous inflammation with patchy necrosis. Typically, a mixed inflammatory reaction is observed, with neutrophils, granulomas, epithelioid histiocytes, and foreign body giant cells. Examination reveals several round-to-oval yeast cells, measuring 9-13μm in diameter. Single broad-based (4-5 μm wide) buds and thick, double contoured, refractile cell walls are also characteristic of the yeast forms visualized here, leading to a rapid presumptive diagnosis.
Image 2: Scotch Tape touch preparation of one white colony growing on potato flake agar (25°C) after 10 days of incubation.
Growth of the fungus on various culture media is more sensitive than direct examination and yields a definitive diagnosis. On potato flake agar incubated at room temperature (25°C), one white colony that was tan on the reverse began growing at 8 days. Typically, colonies appear in 1-4 weeks and range from white (initially) to brown (with age). Microscopic examination of a Scotch Tape touch prepared at 10 days (Image 2) demonstrates the mold form of this dimorphic fungus has delicate, septate hyphae with right-angle conidiophores that bear single, terminal conidia (resembling lollipops). A DNA probe is used to confirm the identification of Blastomyces dermatitidis.
Discussion
As described above, Blastomyces dermatitidis is a thermally dimorphic fungus. In the environment, the mold form of B. dermatitidis is found in wet soil, particularly when enriched by animal droppings and decaying organic matter (1). When a susceptible host (healthy or immunocompromised) disrupts wet earth that contains B. dermatitidis, infectious conidia are inhaled into the lungs. Adult men are more likely to have blastomycosis, likely because they partake in outdoor activities (ex. hunting, fishing) that are associated with environmental exposure to airborne conidia.
Symptoms of blastomycosis are variable, ranging from asymptomatic or transient flu-like to severe pulmonary involvement. Patients may present with symptoms of acute pneumonia (fevers, chills, cough, hemoptysis, and dyspnea) that can be indistinguishable from viral or bacterial causes. Other patients, with chronic pneumonia, have systemic symptoms (weight loss, low-grade fevers, night sweats, productive cough, and chest pain) that overlap with pulmonary tuberculosis, histoplasmosis, or bronchogenic malignancy. In addition to the primary pulmonary infection, approximately half of patients develop extrapulmonary symptoms from hematogenous dissemination to almost any organ; most commonly to skin, bones, male genitourinary, and the central nervous system.
Regardless of symptoms, a majority of patients with blastomycosis will have chest X-ray findings, alveolar infiltrates or a mass lesion involving any location that are non-specific and may mimic malignancy. The mortality rate is 0% in healthy hosts and up to 30% in immunocompromised people, frequently due to disseminated disease. There are no guidelines for susceptibility testing of dimorphic fungi. The preferred treatment of mild to moderate pulmonary blastomycosis is itraconazole for 6-12 months. Conversely, amphotericin B is used in moderately severe disease to treat chronic pulmonary symptoms, disseminated blastomycosis, CNS involvement, immunocompromised or pregnant patients.
Reference
Saccente M, Woods GL. Clinical and laboratory update on blastomycosis. Clin Microbiol Rev. 2010;23(2):367-81.
-Adina Bodolan, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 19 year old African American male presented to the emergency department (ED) with complaints of fevers, chills, nausea, vomiting, a “head-splitting” headache and abdominal pain. He reported that his fevers and chills had increased in severity, reaching a max of 104°F, and had 7-8 episodes of non-bloody emesis on the day of presentation. Travel history was significant for a recent return from a two year visit to his home country of Ghana. He did state he was bitten by mosquitos there about a week before his symptoms began. In the ED, vital signs showed a fever of 102.6°F, increased respirations (36 per minute) and a normal pulse and blood pressure (98 beats per minute and 120/65, respectively). Initial CBC showed a hemoglobin of 13.2 g/dL and a hematocrit of 37.3%. Platelet count was decreased (31,000 TH/cm2). A malaria screen was ordered to look for the presence of blood parasites.
Laboratory Identification
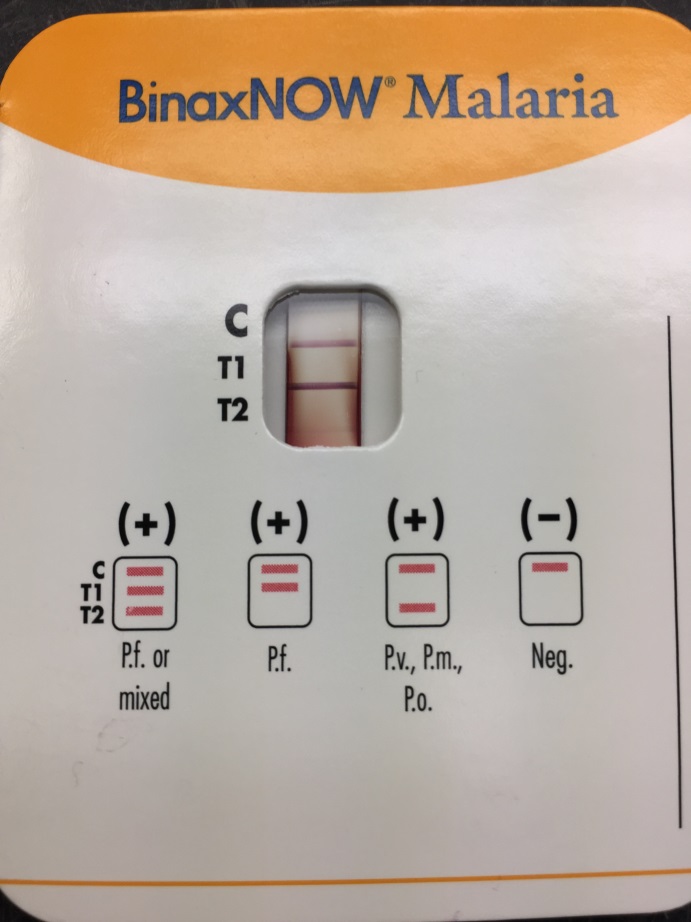
Image 1. The rapid detection test for malaria antigens showed a strong positive band for Plasmodium falciparum (T1) and a weak positive band for common malarial antigens (T2). Image 2. Giemsa blood smear revealed multiple intracellular trophozoites (ring forms) (100x oil immersion).
The BinaxNOW rapid malaria screening test was positive for both P. falciparum and common malarial antigens, making a possible mixed infection unable to be ruled out (Image 1). The thin blood smear revealed numerous trophozoites with multiple ring forms in one red blood cell and appliqué forms, findings characteristic of P. falciparum (Image 2). No advanced forms, including schizonts and gametocytes, were identified. The high level of parasitemia (approximately 5.5%) also supported the diagnosis of P. falciparum.
Discussion
Malaria is a disease infecting humans through the bite of the female Anopheles mosquito and affects many worldwide, particularly in the tropic and subtropic regions of Africa and Southeast Asia. According to the Centers for Disease Control and Prevention (CDC), an estimated 212 million cases of malaria occurred in 2015 with 429,000 deaths attributed to malaria. In the United States, the majority of cases are diagnosed in travelers and immigrants returning from endemic areas. Rapid diagnosis of malaria, especially in the most aggressive Plasmodium falciparum species, is of utmost importance in order to provide prompt treatment to the patient to minimize morbidity and mortality. Clinical findings can be non-specific, especially early in the disease course, and it is important to ask about travel and exposure history. In the case of P. falciparum, cyclic tertian fevers, chills, headache, nausea, vomiting and muscle aches are common.
Definitive diagnosis is achieved by examination of thick and thin blood smears in the clinical laboratory. These two Giemsa stained smears are prepared in order to recognize the Plasmodium organisms (thick smear) and identify the particular species causing infection (thin smear). This approach remains the gold standard for laboratory confirmation of malaria. In the case of P. falciparum, the most common microscopic findings include visualizing early intracellular trophozoites (two chromatin dots connected by a thin cytoplasm). Multiple rings in a single red cell and appliqué forms (trophozoites at the edge of the red cell) are common as well. The crescent shaped gametocyte is also a diagnostic form of P. falciparum, with schizonts being rare in peripheral blood smears.
Immunochromatographic testing is gaining popularity due to their ability to rapidly (10-15 minutes) detect malaria antigens. This makes them a useful alternative to microscopy where resources do not allow for adequate microscopic examination or trained staff is unavailable around the clock. Although these tests are useful in some clinical settings, cost, accuracy and overall performance need to be considered prior to implementation.
Following identification, another important aspect of the laboratory diagnosis is determining the level of parasitemia, as this aids in the classification of disease severity and how anti-malarial drugs should be administered and in what setting. This determined by the following equation using the thin smear: (number of infected RBCs/total number of RBCs) x 100. At least 500 RBCs should be counted, but in the case of lower levels of parasitemia upwards of 2,000 cells is recommended for the most accurate percentage. Other important points include that gametocytes should not be included in the count and red cells infected with more than one trophozoite should be counted as one infected cell.
In the case of our patient, his parasitemia level of approximately 5.5% classified him as a severe malaria infection and he was transferred to the intensive care unit for close monitoring and treatment with IV quinidine, as this drug is associated with hypoglycemia and QT prolongation. After 24 hours, his parasitemia level was 2.6% but due to significant prolongation of the QT interval on EKG from 407 ms to 560 ms, he was switched to oral atovaquone-proguanil (malarone) after consultation with experts at the CDC. Parasitemia level was 0.4% after an additional 24 hours. The patient was discharged home after completion of therapy and was well at follow up outpatient visit.
-Eric Tillotson, MD, is a second year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the director of the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
Everyone knows that the Gram stain is an essential microbiological method which aids in the differentiation of bacteria. When a specimen is sent to the clinical microbiology laboratory for culture, the Gram stain result is frequently the first information provided to the clinician. It is used to first determine a) if infection is present and b) what type of infection (i.e., gram positive vs. gram negative? monomicrobial vs. polymicrobial?). Furthermore, if organisms are observed in a normally sterile fluid/tissue (i.e., blood, cerebral spinal, fluid, cardiac tissue, etc.) the Gram stain result can be a critical result. More importantly, the Gram stain result often drives patient care.
The Issue
Although the Gram stain is an essential clinical tool, many laboratories struggle to maintain competent technologists, especially on off-shifts or in laboratories that lack microbiology expertise (generalists). The need for second review is common when performing Gram stains as they are often subject to variability due to inconsistent staining techniques, antibiotic pressure, as well as artifacts. Even under best case scenarios, Gram stain interpretation can be challenging and may require multiple reviewers.
The Solution
Telemicroscopy offers an easy to use and relatively inexpensive solution to provide formal and informal second opinions to various sections of the laboratory (microbiology, hematology, pathology). With the proper tools, telemicroscopy allows Gram stain interpretation from anywhere there is internet access. Every hospital laboratory has a microscope and a computer with internet, so the only item that may need to be purchased is a microscope camera (≥$5,000). There are also various microscope adapters available for phone cameras that provide equal results for less capital (≥$90). The microscope adapter encases the smart phone and then fits into the eyepiece of most microscopes.
Telemicroscopy utilizes technology to improve diagnostic accuracy, by providing expert consultation for technologists who are uncertain of their results. Telemicroscopy allows laboratories to “present” still or live images to a reference laboratory via a web-based software application such as Skype (or FaceTime if using an iPhone).
About Geisinger Medical Laboratories Telemicroscopy Program
Geisinger Medical Laboratories is an eight hospital integrated health service organization, serving >2.6 million residents throughout 46 counties in Pennsylvania. Geisinger Medical Center serves as the reference laboratory for 4 minimal laboratories (Gram stain reading, no culture work-up) and 2 partial laboratories (Gram stain reading, limited culture work-up). The Telemicroscopy program consists of presenting still or live images [Olympus BX40, BX41 microscope, Nikon cellSense software (version 1.7.1)] to the reference laboratory via Skype [Logitech 920 camera (version 2013)]. The telemicroscopy result, which is a consensus finding, is manually recorded and followed up with culture review to determine patient impact.
The Outcome
We evaluated the effect of implementing a telemicroscopy program on patient care. A retrospective look back at our telemicroscopy data showed that nearly 40% of consults resulted in a change to the original interpretation. The consensus Gram stain result correlated with culture 85% of the time. Overall, 49% of the cases assessed by telemicroscopy were impacted by the consult. Of which, patient care was positively and negatively impacted in 72% and 28% of cases, respectively.
The Conclusion
Gram stain consultations via telemicroscopy from remote hospital sites can improve patient care. Telemicroscopy offers a simple, inexpensive, and innovative approach to providing expert consultation services to off-shift or inexperienced staff. This is also a great way to promote interdepartmental consultation and collaboration (i.e., between microbiology and hematology or pathology).
Image 1. Telemicroscopy via traditional microscope camera. Microscope with camera attached and computer screen showing Gram stain.Image 2. Telemicroscopy via s mart phone. Close up of microscope adapter attached to microscope. Image of Gram stain displayed on phone screen.
References:
Microbiology Strong: Enhancing Microbiology Services and Technical Support in an Integrated Laboratory System. ASCP. Las Vegas, Nevada. September 2016. Oral presentation.
Martinez, R.M., Shoemaker, B.C., Riley, J.A., and Wolk, D.M. 2016. The TeleGram of the 21st Century: the Digital Gram Stain. American Society for Microbiology (ASM) General Meeting. Boston, MA. Poster presentation.
-Raquel Martinez, PhD, D(ABMM), was named an ASCP 40 Under Forty TOP FIVE honoree for 2017. She is one of two System Directors of Clinical and Molecular Microbiology at Geisinger Health System in Danville, Pennsylvania. Her research interests focus on infectious disease diagnostics, specifically rapid molecular technologies for the detection of bloodstream and respiratory virus infections, and antimicrobial resistance, with the overall goal to improve patient outcomes.
A 65 year old male with a history of systolic heart failure secondary to non-ischemic (alcohol-induced) dilated cardiomyopathy underwent cardiac transplantation on 10/11/2016. He was hospitalized between 3/1/17 and 4/15/17 for neutropenia and CMV viremia. Two days after discharge, he presented to the hospital with a gradual-onset of left-sided sharp chest pain described as “soreness” over his rib cage and exacerbated by breathing. Associated symptoms included fever, malaise, and fatigue. In the emergency department, vital signs included: BP 144/75 mmHg, T 40.2°C, RR 24/min, HR 101 bpm, SpO2 97% on room air. A CBC revealed a normal white blood cell count and a chest X-ray demonstrated a lingular opacity. The immunocompromised patient was admitted for sepsis secondary to presumed pneumonia following recent hospitalization. He was treated empirically for hospital-acquired pneumonia with vancomycin and piperacillin-tazobactam. After a urine antigen test detected the presence of Legionella pneumophila serogroup 1, antibiotic treatment was changed to levofloxacin and an induced sputum culture was obtained for Legionella surveillance.
Image 1. Sputum culture on BCYE agar with PAV shows Legionella pneumophila colonies that are circular with smooth edges, grey-white, and glistening in addition to few usual oropharyngeal flora.
Discussion
Legionnaires’ disease, caused by Legionella bacteria, is a cause of 1-9% of both community-acquired and hospital-acquired pneumonias. Symptoms of fever, chills, cough, and chest pain are similar to other causes of pneumonia; however multiple organ systems may be involved, producing additional symptoms including gastrointestinal (diarrhea, nausea, and vomiting) and central nervous system (headache and confusion) findings. Legionella was first discovered after a 1976 outbreak of pneumonia among Pennsylvania State American Legion members who attended a convention at a Philadelphia hotel that had infected water in the air conditioning system; it is reported that 29 out of 182 infected people died. At present, the mortality rate of Legionnaires’ disease ranges from less than 10% in treated community-acquired cases to approximately 30% for hospital-acquired cases.
The genus Legionella contains greater than 60 species of which approximately 20 are human pathogens. Legionella pneumophila (consisting of serogroups 1-16) is the most common cause of Legionnaires’ disease and, in particular, L. pneumophila serogroup 1 causes 70-90% of cases. The organisms are ubiquitous in nature, particularly in warm freshwater environments including lakes and streams, where they infect and multiply within single-celled host organisms. Of pathogenic concern, they can be present in high numbers in human-made complex water systems (such as cooling towers, whirlpool spas, humidifiers, and decorative fountains). After environmental aerosols are inhaled or contaminated water is aspirated into the lungs, alveolar macrophages are infected by the obligate intracellular bacteria. Host risk factors for developing Legionnaires’ disease include organ transplantation, immunocompromised state, immunosuppresion, age greater than 60 years, chronic lung disease, and smoking.
In the microbiology laboratory, Legionella are mesophilic (20-45 °C) obligate aerobes. The small, thin gram negative rods react poorly with Gram stains and are not usually stained in direct clinical samples. The patient’s Gram smear revealed moderate neutrophils, few squamous epithelial cells, and mixed gram positive and gram negative organisms present. Sensitivity for detecting the biochemically inert and fastidious bacteria is increased with culture on buffered charcoal yeast extract (BCYE) agar. For sputum samples that are likely contaminated with usual oropharyngeal flora, BCYE agar with polymyxin B, anisomycin, and vancomycin (PAV) media are used. After 3-5 days of incubation, Legionella colonies appear convex, circular, 3-4 mm in diameter, grey-white to blue-green, and glistening. This identification was confirmed by MALDI-TOF MS. Laboratory in vitro susceptibility studies are not recommended on individual isolates, as they do not correlate with clinical responses. Monotherapy with a fluoroquinolone (Levofloxacin) or macrolide (Azithromycin) is active against Legionella.
-Adina Bodolan, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A twenty-four year-old male Kenyan refugee had been in the United States for about a month when he received a mandatory health screen for infectious diseases. He had no complaints and stated that overall, he was generally healthy. Physical exam was significant only for bilateral red conjunctiva. He stated at times his eyes get irritated and have since birth. As part of routine work-up, an ova and parasite stool exam was ordered. Organisms were detected as seen in Image 1.
Image 1. Trichrome stained slides of patient’s stool sample.
Discussion
The patient’s stool examination showed Giardia cysts. Two nuclei are visible in the figure above with centrally located karyosomes. Also visible are the intracytoplasmic fibrils, seen as a darker purple area.
Giardia is a flagellated protozoan that causes giardiasis, a diarrheal illness. It is the most commonly diagnosed intestinal parasitic disease in the United States. It is known as Giardia intestinalis, Giardia lamblia, or Giardia duodenalis. The most common mode of transmission is drinking water contaminated with feces from infected mammals (1).
Symptoms vary and can last 1 week to years if untreated (2). Typical symptoms of giardia are “greasy, foul-smelling, frothy stools that float.” Interestingly, less common symptoms can be itchy skin, hives, eye and joint swelling (3). Retinal arteritis and iridocyclitis has been noted as well (4). It is possible that this patient’s eye irritation is due to a chronic giardiasis infection. Common treatment is usually with an antibiotic/antiparasitic drug like metronidazole (Flagyl).
Diagnosis of Giardia can be made by demonstrating the pear shaped trophozoites and/or ovoid cysts in feces. A key identifier for this parasite is the presence of the two to four nuclei with a central karyosome and intracytoplasmic fibrils that make the parasite look like a face under the microscope. However, because Giardia is excreted intermittently, it is recommended to sample three stool specimens on separate days (5). Due to problems in concentrating the organism for identification on a trichrome stain, a fecal immunoassay is available that is more sensitive and specific (5).
-Angela Theiss is a pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 10 year old Caucasian male presented to the pediatric emergency department due to significant pain in his right knee with exposed hardware. His past medical history was noteworthy for Perthe’s Disease, a condition leading to avascular necrosis of the femoral head. In addition, he is affected by an autosomal dominant congenital disorder and has had ischemic strokes in the past. Recently, he had surgery performed on multiple joints to correct abnormalities and they were complicated by dehiscence & infection with methicillin sensitive Staphylococcus aureus. On current admission, his mother reported he has been afebrile and was consistently taking cephalexin to treat the above infection. He was taken to the operating room for incision & drainage and hardware removal of the knee. Bacterial cultures were collected at the time of surgery and he was started on IV clindamycin.
Laboratory Identification
Image 1. Clear, spreading colonies that showed “pitting” of the agar after 48 hours incubation at 37°C in 5% CO2. Image 2. Gram stain directly from the colony showed slender gram negative rods (100x oil immersion).
On direct Gram stain, there was no organisms seen and rare white blood cells. Initially, there was no growth at 24 hours, but two morphologies were observed on the second day. The first organism was identified as the S. aureus that was previously isolated from this site. The second organism was clear with spreading colonies that pitted the agar (Image 1). A distinct bleach like odor was observed. There was no growth on MacConkey agar even though the Gram stain showed gram negative rods, making this organism most likely to be classified as fastidious (Image 2). Benchtop biochemical tests were negative for catalase and positive for oxidase. MALDI-TOF mass spectrometry identified the isolate as Eikenella corrodens.
Discussion
Eikenella corrodens is a fastidious Gram negative rod that is a member of the HACEK family. It is considered normal flora in the oral cavity and possibly the gastrointestinal tract of humans. Infection results from these endogenous sources and can be the result of poor oral hygiene, mucositis or dental procedures. E. corrodens causes juvenile and adult periodontitis and is commonly implicated in bacteremia and infective endocarditis, particularly in IV drug users who lick needles prior to injection. Infections of the abdomen, bones/joints and brain are less common.
In the laboratory, E. corrodens is slow growing and is usually present as clear, spreading colonies after 48 hours incubation at 37°C in 5% CO2 on blood and chocolate agars. A unique feature of the organism is that it pits or corrodes the agar, lending to its species name. Also, E. corrodens produces a bleachy smell due to the production of hypochlorite. It does not grow on MacConkey agar despite the fact it is a Gram negative rod. Biochemical tests are negative for catalase, positive for oxidase and negative for indole. Automated instruments and MALDI-TOF mass spectrometry are both able to identify E. corrodens with confidence.
Susceptibility guidelines can be found in the 3rd edition of the CLSI M45 document. In general, E. corrodens is susceptible to penicillin, board spectrum cephalosporins, carbapenems, azithromycin and fluoroquinolones. Resistance to narrow spectrum cephalosporins, macrolides and clindamycin has been documented. In general, susceptibility testing should be performed on E. corrodens when it is isolated from a normally sterile site or is identified in pure culture. Beta lactamase testing is recommended routinely on E. corrodens, and if positive, the isolate is resistant to penicillin, ampicillin and amoxicillin. In the case of bite wounds caused by E. corrodens, susceptibility testing may not be necessary if it is treated with amoxicillin-clavulanate acid (Augmentin) due to a high probability of susceptibility to this antibiotic.
In the case of our patient, he responded to the antibiotic therapy used to treat his S. aureus and E. corrodens infections and healed well. He was placed on long term oral antibiotic therapy until additional hardware is able to be removed at a future date.
-Rim Alkawas, MD, is a first year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the director of the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.