Case History
A 19 year old African American male presented to the emergency department (ED) with complaints of fevers, chills, nausea, vomiting, a “head-splitting” headache and abdominal pain. He reported that his fevers and chills had increased in severity, reaching a max of 104°F, and had 7-8 episodes of non-bloody emesis on the day of presentation. Travel history was significant for a recent return from a two year visit to his home country of Ghana. He did state he was bitten by mosquitos there about a week before his symptoms began. In the ED, vital signs showed a fever of 102.6°F, increased respirations (36 per minute) and a normal pulse and blood pressure (98 beats per minute and 120/65, respectively). Initial CBC showed a hemoglobin of 13.2 g/dL and a hematocrit of 37.3%. Platelet count was decreased (31,000 TH/cm2). A malaria screen was ordered to look for the presence of blood parasites.
Laboratory Identification
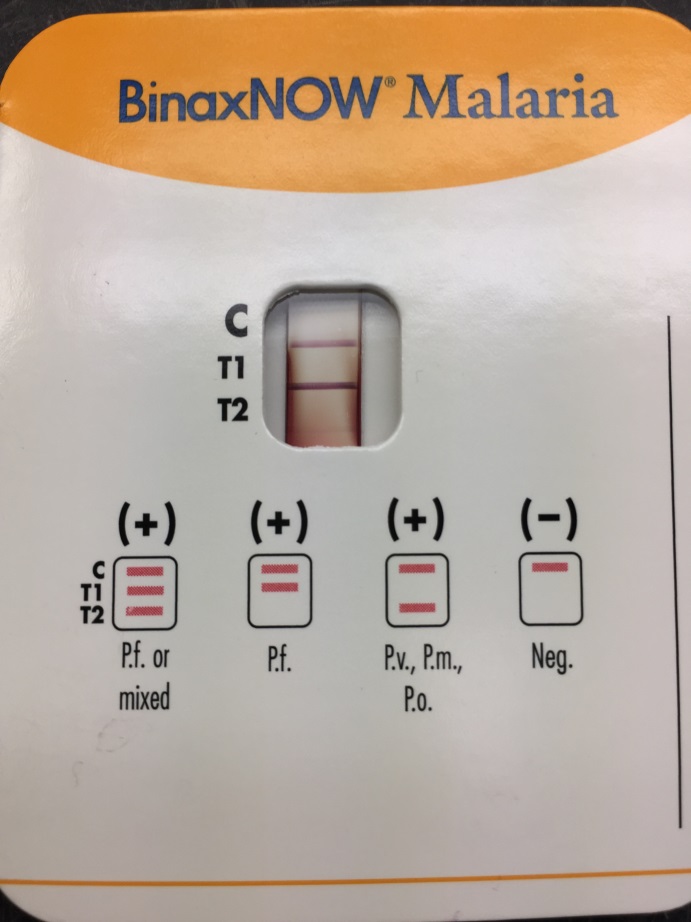

The BinaxNOW rapid malaria screening test was positive for both P. falciparum and common malarial antigens, making a possible mixed infection unable to be ruled out (Image 1). The thin blood smear revealed numerous trophozoites with multiple ring forms in one red blood cell and appliqué forms, findings characteristic of P. falciparum (Image 2). No advanced forms, including schizonts and gametocytes, were identified. The high level of parasitemia (approximately 5.5%) also supported the diagnosis of P. falciparum.
Discussion
Malaria is a disease infecting humans through the bite of the female Anopheles mosquito and affects many worldwide, particularly in the tropic and subtropic regions of Africa and Southeast Asia. According to the Centers for Disease Control and Prevention (CDC), an estimated 212 million cases of malaria occurred in 2015 with 429,000 deaths attributed to malaria. In the United States, the majority of cases are diagnosed in travelers and immigrants returning from endemic areas. Rapid diagnosis of malaria, especially in the most aggressive Plasmodium falciparum species, is of utmost importance in order to provide prompt treatment to the patient to minimize morbidity and mortality. Clinical findings can be non-specific, especially early in the disease course, and it is important to ask about travel and exposure history. In the case of P. falciparum, cyclic tertian fevers, chills, headache, nausea, vomiting and muscle aches are common.
Definitive diagnosis is achieved by examination of thick and thin blood smears in the clinical laboratory. These two Giemsa stained smears are prepared in order to recognize the Plasmodium organisms (thick smear) and identify the particular species causing infection (thin smear). This approach remains the gold standard for laboratory confirmation of malaria. In the case of P. falciparum, the most common microscopic findings include visualizing early intracellular trophozoites (two chromatin dots connected by a thin cytoplasm). Multiple rings in a single red cell and appliqué forms (trophozoites at the edge of the red cell) are common as well. The crescent shaped gametocyte is also a diagnostic form of P. falciparum, with schizonts being rare in peripheral blood smears.
Immunochromatographic testing is gaining popularity due to their ability to rapidly (10-15 minutes) detect malaria antigens. This makes them a useful alternative to microscopy where resources do not allow for adequate microscopic examination or trained staff is unavailable around the clock. Although these tests are useful in some clinical settings, cost, accuracy and overall performance need to be considered prior to implementation.
Following identification, another important aspect of the laboratory diagnosis is determining the level of parasitemia, as this aids in the classification of disease severity and how anti-malarial drugs should be administered and in what setting. This determined by the following equation using the thin smear: (number of infected RBCs/total number of RBCs) x 100. At least 500 RBCs should be counted, but in the case of lower levels of parasitemia upwards of 2,000 cells is recommended for the most accurate percentage. Other important points include that gametocytes should not be included in the count and red cells infected with more than one trophozoite should be counted as one infected cell.
In the case of our patient, his parasitemia level of approximately 5.5% classified him as a severe malaria infection and he was transferred to the intensive care unit for close monitoring and treatment with IV quinidine, as this drug is associated with hypoglycemia and QT prolongation. After 24 hours, his parasitemia level was 2.6% but due to significant prolongation of the QT interval on EKG from 407 ms to 560 ms, he was switched to oral atovaquone-proguanil (malarone) after consultation with experts at the CDC. Parasitemia level was 0.4% after an additional 24 hours. The patient was discharged home after completion of therapy and was well at follow up outpatient visit.

-Eric Tillotson, MD, is a second year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the director of the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
