Leaders’ decisions and actions have moral ramifications, both on an individual and an organizational level. There are three factors of moral development, namely moral capacity, moral courage, and moral resiliency.
Being able to recognize a dilemma as a moral issue is one of the critical aspects of leadership. Such awareness is referred to as moral capacity, which influences the characteristics and recognition of a moral issue. There are multiple aspects that influence a leaders’ moral capacity. The first aspect is their previous experiences with moral dilemmas and how much they learned from them. The second is to what extent a leader is able to see and understand the multiple perspectives of an issue. The third is how leaders view their role and whether or not that incorporates a moral view.
It is not enough to understand and recognize a moral dilemma, it is important to act on it. Such moral courage is especially important when under pressure to act immorally. Such pressure can come from peers, supervisors, or the entire organization. Therefore, the more moral courage someone has, the more likely it is that they take a moral action or make a moral decision. One important aspect of moral courage is the notion of willpower. Willpower is a muscle that people can practice with small tasks, such as drinking a glass of water before breakfast. The more people practice it on small tasks, the more likely they are to use it during challenging situation, such as making a moral decision when pressured to do otherwise.
Moral resiliency is an extension of moral courage. While moral courage focuses on the strength to make moral decisions in the short-term, moral resiliency is a process through which leaders continuously adapt their moral compass and actions. Moral resiliency is this what creates sustainable moral decision-making.
Depending on how leadership effectiveness is defined, moral behavior can either make leaders more or less effective. When looking at effectiveness in the short term, it is possible that moral behavior can impede effectiveness if measured in terms of money or short-term success. However, when looking at effectiveness in the long term, moral behavior increases leaders’ effectiveness. The more honest, and thus morally, people behave, the more effective they are. In a world that is becoming more globalized, it is critical for leaders to understand that culture influences moral and ethical behavior. In other words, what is moral in one culture might be immoral in another. To increase leaders’ effectives it is therefore important to understand the cultural implications of behavior and to be aware of the differences in appropriate and effective behavior.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
While Maria was working in Microbiology, she cut her finger while pulling reports off of the printer. It was a minor paper cut, so she ignored it, put her gloves on and continued her work back on the bench. A week later, the tiny cut was swollen and red. She decided to report the incident to her manager since it wasn’t healing. The manager asked Maria to report to the Occupational Health department, but was unsure if any treatment would be covered since the incident was not reported while she was at work.
Steve and Josh were bored during the night shift and they created a ball made from rubber bands to toss around. When Josh didn’t catch the ball, it hit the open tray of formaldehyde on the gross bench, and it splashed into Josh’s eye. He rinsed his eyes in the eyewash station for a couple of minutes, but both men were afraid to report the incident for fear of getting in trouble. Josh’s eye irritation continued to worsen, and he had to go to the eye doctor for treatment.
There are obvious consequences for injuries that occur in the laboratory, and reporting them is important for many reasons. Staff may be motivated in some instances to not report, but that creates problems for the individual, the department, for the facility, and even for other labs across the country! That may seem like a stretch, but it will become clearer with exploration.
The value in injury and accident reporting starts with medical follow-up. Those incidents which require treatment or abatement of infection can and should be dealt with quickly, and appropriate monitoring can be done if necessary. Some injuries may require immediate first aid, and a trip to the emergency department may even be necessary. Not reporting those types of injuries can be very dangerous for staff. Other incidents may require physician office visits or other monitoring, and employees who need it should be encouraged to comply.
In many work places the injury follow-up visits and treatment are covered financially by the institution, either via a structured occupational health program or through reimbursement. Some organizations may not offer financial coverage, however, if the incident that occurred at work is not reported as soon as possible. That reporting delay can raise suspicion as to whether or not the injury actually did occur while on the job, and since the written reporting protocol was not followed, there may also be no obligation for employer medical coverage.
Departmental issues will arise when incident reporting in not part of the overall lab safety culture. Sometimes there can be reprisals for unsafe behaviors which lead to accidents, but if the safety culture is good and if managers and employees coach against such practices, then there should be fewer overall incidents to report. That said, a culture of secrecy regarding injuries or exposures can also be dangerous. There is value in talking to all staff about an incident that occurred within the department. Staff can learn from the event and have a healthy discussion about how to keep it from reoccurring. A discussion of events can bring important safety issues to light, particularly if similar incidents happen with multiple people. This sharing of information can also promote awareness of good safety practices that can aid in the prevention of further incidents for all who work in the department.
OSHA requires the reporting of certain work place injuries, those that may have led to time away from work or that need medical follow up, for example. This injury data is compiled and reported nation-wide. It becomes a good source for benchmark data, a way to be able to compare your lab injury rates with others across the country. The U.S. Bureau of Labor Statistics provides this data as information labs can use. One way to utilize the information is to see if the number of reportable injuries you are seeing in your lab is comparable to a national average. That assessment can give you a starting point in determining whether or not your lab’s safety incidents are at typical levels. Of course, lab safety professionals want to see zero injuries, but if you see your lab injury numbers are very high compared to benchmark data, you can begin to see where to focus in on fixes for the lab physical environment or on creating specific safety training.
There is great value in talking about safety incidents that may result in injury or exposure in the lab setting. These “safety stories” raise awareness of safety issues, and they can act as a deterrent for repeat incidents. Create a culture where staff feel free and comfortable to report incidents, and be sure to discuss them with all staff, and record reportable injuries as well. Having reliable national data also provides helpful information to other labs, and better information can help to improve safety in laboratories everywhere!
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Recently, a new technology has become available for screening the esophagus for early detection of at-risk patients for cancer. Esophageal cancer has one of the highest mortality rates. Watch this interview with Rob Odze, a pathologist who works with the technology, and learn more about how this could impact the practice of clinicians, pathologists, and laboratory professionals involved in upper endoscopy services.
-Dan Milner, MD, MSc, spent 10 years at Harvard where he taught pathology, microbiology, and infectious disease. He began working in Africa in 1997 as a medical student and has built an international reputation as an expert in cerebral malaria. In his current role as Chief Medical officer of ASCP, he leads all PEPFAR activities as well as the Partners for Cancer Diagnosis and Treatment in Africa Initiative.
There are currently five different generations at work today: Traditionalists, Baby Boomers, Gen Xers, Millennials, and Generation Z. This means that in any work environment, you can have a group of people between the ages of 15-80. This is an exciting time to be working because we can all learn from many different generational experiences, values, and communication styles.
The two largest generations in the work place are the Baby Boomers and the Millennials. This is because these are both the largest generations in terms of population. However, with the Baby Boomers slowly moving into retirement, the Millennials are about to take over.
Traditionalists are still present in the workforce for a few reasons. First, they have tremendous experience and organizational knowledge and many organizations are trying to keep them around so that they do not lose that information. This means that Traditionalists are often Presidents of organizations or members of their Board of Directors. Secondly, Traditionalists are loyal to their organizations and they generally keep working as long as they can because of their values of security and getting the job done.
Generation X and Z are also in the workplace, but neither is very large. However, Gen Xers serve an important purpose because they are flexible and adaptable and because they value work-life balance and constructive feedback. They understand both the world without technology, so that can relate to Baby Boomers, and the world of the internet and social media, so they learn technology fast, which is appreciated by Millennials. Generation Z is only now starting to enter the workforce, so little is known about their work styles. However, they are expected to be independent, entrepreneurial, determined, and loyal.
The key to working with multiple generations is respect. Everyone wants to be respected and appreciated for what they bring to an organization. Being open and flexible to learning about different generational values and communication styles, will set any leader and employee up for success. Provide everyone with positive and constructive feedback and create a work environment that allows for more flexibility in terms of work hours, work location, and dress code whenever possible. Finally, realize that what motivates you personally is not necessarily what motivates other, especially if they are from different generations. Working with a diverse group of generational workers is a great benefit, to both the organization and to individuals.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
Video 1. Another classic excerpt from a favorite: ZDoggMD, singing about this year’s flu season and available testing options on the horizon—because, let’s face it—rapid flu tests aren’t quite cutting it anymore.
Hello again everyone! Back again to talk about a new set of recommendations from last month’s post. This time it’s about influenza. Recommendation: get vaccinated. Thank you. See you next time…
Seriously, as the 2018-2019 flu season dawns upon us, it’s time to talk about vaccines, tests, prevention, and health literacy. I’m sure many of your social media pages are filled with various debates, articles, and fake news stories on one side or another pitting science, pseudo-science, and non-science all against each other for public spectacle. In the lens of laboratory science and medicine at large, I think most if not all of us agree that preventable diseases should be prevented, and if not, at the very least detected accurately, sensitively, and early. Influenza A/B is a prime example of a consistent threat to our health and safety that has wavered responses in various socio-medical circles.
Official communication and guidance from the Centers for Disease Control and Prevention (CDC) clearly tells those of us in health-care to embrace a multi-tiered approach to protecting public health regarding the flu. That approach includes vaccination, testing, infection control, anti-viral treatment, and anti-viral prophylaxis. And why such a fuss over the flu? It’s a big deal! Last year, the CDC reported approximately 80,000 deaths associated with influenza as a primary cause. 80,000 deaths! That’s almost 7 times as many that died from H1N1/Swine Flu complications back in 2009, where only 12,000 patients were killed by the virus. And even more so, in the terrifying Ebola epidemic of 2016—in which there was a staggering 1 recorded death in the US—nearly 29,000 people were infected globally and only 11,300 died (despite under-reporting). I’m being dramatic, I know. But it’s important for us to recognize true epidemics when they happen, and even more important for societies like ours to be at the forefront of preventing them from developing any further.
Image 1. The CDC recommends you get your flu shot every year, because obviously.
Image 2. I’m not here to talk about the anti-vax elephant in the room. That’s not fair to elephants. But imagine if the CDC reported 44% of flu vaccine misconceptions were addressed!
As an aside, I’ll probably recommend that you get your annual flu shot a hundred times in this post alone. But just to have a clear reference, please look at the following table. It’s critical to be able to both distinguish common cold versus influenza symptoms for yourself, as well as educate your patients and peers about the differences between the two. This information can change the way people perceive treatments (i.e. why the doctor only recommended rest/Tylenol and didn’t give out antibiotics for their symptoms) and why it’s absolutely crucial to protect vulnerable populations from an otherwise fatal virus. So, micro-rant aside, it should be clear that by now we should be working on a way to both improve our prophylaxis with vaccines and medications as they always leave room for improvement—I’m looking at you Tamiflu and Relenza! Notwithstanding any analysis of efficacy for the flu vaccine, the CDC reports a variable and transparent success rate of vaccines. It can be difficult to predict and assess epidemiologic trends and mutations as the influenza virus continues to change annually.
Table 1. Distinguishing the common cold, and “flu-like symptoms” from a proper influenza viral infection.Image 3. CDC Report on seasonal flu vaccine effectiveness since 2004.
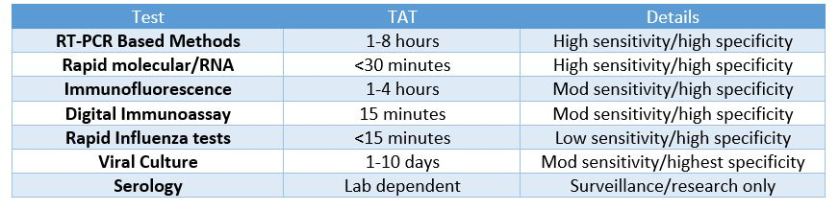
So, what was the deal with ZDoggMD plugging some PCR testing in the opening credits here? That’s a good question and one that inspired this article in the first place. Obviously, if you follow my posts you know I follow his, and at the end of this latest video he discusses new available options for influenza point-of-care testing (POCT) for clinics and emergency rooms. This was a partnership with the company Cepheid and linked with their promoting their POCT PCR-based FluA-B testing. Here’s a quick paraphrasing of the CDC recommendations on influenza testing: because of the numerous false negative tests every season, the bests tests in order of preference are RT-PCR, immunofluorescence, and rapid antigen testing. Did you catch that? Rapid Flu swabs are bottom of the barrel stuff here. UpToDate, the clinical resource for current practices and standards discusses rapid influenza tests as sacrificing turn-around-time (TAT) for accuracy: “commercially available rapid antigen tests for influenza virus yield results in approximately 15 minutes or less but have much lower sensitivity than RT-PCR, rapid molecular assays, and viral culture.” (I didn’t bold those words, they did). Most of the places I’ve worked run through boxes of rapid flu swab kits ALL DAY LONG. But what are we missing? Clinically, this is supposed to be an important “no miss” diagnosis—it’s dangerous, it’s contagious, it’s mutatable…
Who remembers learning biostatistics in school? Remember SPIN and SNOUT? “Specificity is used to rule IN, Sensitivity is used to rule OUT” So why are we relying on the LOWEST sensitivity available to us for ruling out influenza? Probably because of technological/practical limitations up to this point in time, and of course the most glaring limiting reagent of all: funding, also known as “administrative buy-in.” Have I hit enough lab management buzz words in this post? Not yet.
Table 2. Per UpToDate, these are the quick and dirty details on our favorite available flu tests currently on lab benches across the country. I’d say there’s got to be a better way, but there already is.
Sweet. So, it’s a little expensive but ultimately better for our patients, right? Done and done, whip up a cost-benefit-ratio report for the suits upstairs and let’s start a validation project! Well, yes and no. I’m a big proponent of utilizing MALDI-TOF—the mass spectrometry based system to replace traditional bacterial identifications. A 2015 study published in the Journal of Clinical Microbiology stated, “The use of MALDI-TOF MS equated to a net savings of 87.8%, in reagent costs annually compared to traditional methods. …The initial cost of the instrument at our usage level would be offset in about 3 years. MALDI-TOF MS not only represents an innovative technology for the rapid and accurate identification of bacterial and fungal isolates, it also provides a significant cost savings for the laboratory.” What promise! Cepheid’s ED POCT PCR Flu test promises 18% fewer tests needed, 17% fewer antibiotics prescribed, and overall savings per patient visit of up to $700. But this sounds like another, too familiar, recent promise from another voice in our profession. Something about quick, easy, and accurate testing on chips with micro-laboratories available commercially and only using microliters of whole blood for analysis. “Unfortunately, none of those leads has materialized into a transaction. We are now out of time,” read the goodbye letter to the company’s stockholders—Theranos, that’s the one. The moral of the story here: it’s good to remain fiscally prudent when deciding what your clinic or hospital should invest in with regard to testing. However, when something has been a proven and successful replacement which ultimately is recommended by multiple societies within the field then something’s got to give.
Image 4. MALDI-TOF saves money! You spend a little upfront, but then your hospital can write articles about how your bacteriology department has a swab-to-sensitivity TAT of a few hours. Less errors, less antibiotics, more likes on social media!
What do you see in your practice or laboratory as far as influenza testing? Are there issues I missed? What is your experience with rapid tests, or PCR testing? Is anyone else as big a fan of MALDI-TOF as I am? Did you get your flu shots yet? Leave your comments and questions below! Share with a colleague today!
See you next time!
I have absolutely no affiliation with Cepheid, financial or otherwise, but as an educational/professional resource read more information about Cepheid’s molecular rapid flu tests, read their literature at www.GetTheRightTest.com
Tran A, et al. (2015) Cost Savings Realized by Implementation of Routine Microbiological Identification by Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry. Journal of Clinical Microbiology. DOI:1128/JCM.00833-15
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student actively involved in public health and laboratory medicine, conducting clinicals at Bronx-Care Hospital Center in New York City.
Reflective judgment—the ability to evaluate and process information in order to draw plausible conclusions—is one of the most critical leadership skills. People move through three different phases (pre-reflective judgment, quasi-reflective judgment, and reflective thinking) as they learn to develop their judgment skills.
During the pre-reflective thinking period, people acquire knowledge through experience, observations, evaluation, and authority figures. All information collected is seen as absolute and the truthfulness of the data is not questioned. Problems and challenges views through this lens are resolved with well-structured assumptions and people are certain about the effect of their solutions. This phase has three stages itself. People in the first stage see knowledge as absolute and concrete. Different beliefs are not seen and/or believed. The second stage is exemplified by a similar view, namely that knowledge is certain and absolute, but it is understood that knowledge is not always immediately available. People in this stage also heavily rely on authority figures to get their knowledge from and there is no critical thinking. The third stage embodies knowledge that is either certain or uncertain for a short period of time. If knowledge is uncertain, people in this stage rely on personal beliefs. Authority figures still play an essential role in providing information and all their information is seen as absolute.
The second developmental phase for reflective judgment is the quasi-reflective thinking phase. During this period, people start to recognize and understand that not all information is completely accurate or absolute. Additionally, people acknowledge that claims from authority figures also contain some uncertainty. This uncertainty can be caused by missing or incomplete information or by the methods that were used to gather information. People in this phase use evidence to draw conclusions, but they do not yet understand to process of how to get to a sound conclusion. In this phase, there are two different stages. During the first stage, people understand that knowledge is not absolute or certain. People also acknowledge that there is always a sense of ambiguity in knowledge. In the next stage, context starts playing a significant role. People start to understand that knowledge is bound by a certain context and that it is therefore more subjective than initially assumed. Conclusions are sometimes delayed, because knowledge is created through individual perceptions of reality. During both these stages, information from authority figures are thus not seen and absolute, but as more subjective and uncertain.
The third developmental period of reflective judgment is reflective thinking. In this phase, people understand that knowledge is never certain or absolute. However, instead of becoming stuck because of this understanding, people in this phase work to make conclusions that are reasonable. Knowledge and knowledge claims are actively evaluated based on their context. Critical thinking is an important part of this phase, as knowledge is judged and reflected upon prior to making conclusions. This phase also has two different stages: in the first stage, people understand that knowledge is not absolute and certain. However, information is evaluated and judged by comparing evidence and different opinions about the information. During this stage, the solutions people create are based on certain criteria, for example if the solution is pragmatic. During the final stage of reflective judgment, knowledge is created and accepted through a reasonable inquiry process that promotes critical thinking. The solutions are evaluated based on their probability and reasonableness.
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
In last month’s post we reviewed the importance of being prepared for your regulatory inspections, as well as some tips for how to accomplish this task. This month we’ll focus on the inspection process itself – areas the inspectors may focus on, and how your preparation work last month will make the process go smoothly.
Once your formal inspection is underway, don’t panic. Based on all of your preparation work in the months prior, you should be organized and ready to answer any question the inspectors may have regarding your current procedures and policies. The focus of each inspection will vary based on the regulatory agency it is being performed by, but the following areas have a high likelihood of being reviewed.
Utilize a Patient Tracer. One of the easiest ways to evaluate your laboratory processes from pre-analytical, through analytical phase, and finally the post-analytical phase is to utilize a patient tracer. Inspectors may pick a specific date or date range, and ask to see all associated documents for a particular test.
Pre-Analytic. Gather a copy of the test requisition indicating the patient information, ordering physician, and specific tests requested. Ensure your phlebotomy team knows where your policies related to patient identification and specimen collection are located, and ensure they are following the requirements within these procedures. Inspectors may ask to observe the phlebotomy collection process, so prepare your staff ahead of time to reduce the potential for nervousness.
Analytic. All records related to the testing of the sample will need to be produced. This includes the actual instrument print-out for the sample in question and/or worksheets used to document results, quality control records for the day of testing, instrument maintenance and calibration records, as well as the training and competency records for the technologist who performed the test that day. Training and competency assessment are two different tasks – ensure you have documentation to support both of these activities at the required intervals for the staff member in question. Depending upon the actual circumstances surrounding that particular sample, there may be additional documentation requested such as corrective action logs, critical call notification records, or confirmation testing records.
Post-Analytic. Inspectors will also need to review how your results are being documented and displayed on the patient charts. They will be focusing on accurate transcription of results including units of measure and reference ranges; the correct timing of sample collection, receipt in the lab, and result reporting times; in addition to all of the patient demographics properly being displayed. They may also ask to see a corrected report to see how clinicians are notified about any changes, so patient treatment can be adjusted accordingly in a timely manner.
Proficiency Testing (PT) Results. One of the common requirements of a laboratory accreditation program is the participation in a proficiency testing program for all regulated analytes. Since the intent of this program is to ensure accuracy in your patient testing results, inspectors will be focused on any unsuccessful PT surveys, and the root cause analysis you performed to investigate the occurrence. Was this an isolated and random error, or is there a systemic quality issue which caused the inaccurate result? Did you perform a look-back to confirm accuracy of patient results being reported between the time of PT analysis and when the laboratory was notified of the unsuccessful event? Were your preventive actions implemented and sustained, or are you still continuing to experience accuracy problems with your testing? Be sure to document all steps of your investigation, and have that documentation available to inspectors for review.
Quality Metrics. Laboratory directors have a responsibility to provide oversight of their laboratory’s quality program, and to ensure that medically reliable data is being generated. There are many ways to monitor the quality of your laboratory program, and you should be prepared to speak on your methods in use to the inspectors. Although labs are not expected to be perfect, there is a responsibility to monitor for issues and initiate appropriate corrective and preventive actions when they are identified. Ensure that your monthly performance improvement metrics are reviewed and signed by your laboratory director, and any metrics not meeting performance goals have documented corrective action initiatives. Metrics should be meaningful and demonstrate continuous monitoring and improvements within the laboratory.
Be Honest and Transparent. If an inspector asks for specific documentation which you do not have, be upfront and let them know. Trying to hide a problem or misdirect an inspector away from a problem area can result in even more citations as it creates an environment of mistrust. Inspections are an opportunity to identify and improve upon the weak points in your laboratory program, and the inspectors themselves can offer ideas and suggestions on better ways to meet certain requirements that you may be struggling with. Some regulations can be interpreted differently by different individuals – ensure that your staff can speak to your practices in use and explain to the inspectors how you are satisfying the requirements.
Coming up in part 3, we’ll discuss what to do next – how to address any issues identified during the inspection process, and how to keep the overall experience positive and beneficial to your staff.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018 Top 5 in the 40 Under Forty recognition program. She has worked in the medical laboratory profession for over 18 years. In her current position, she transitions between performing laboratory audits across the entire Northwell Health System on Long Island, NY, consulting for at-risk laboratories outside of Northwell Health, bringing laboratories up to regulatory standards, and acting as supervisor and mentor in labs with management gaps.
Whether your laboratory is accredited by CAP, COLA, JCAHO, or simply adheres to local state and federal CLIA regulations, all laboratories are subject to regular inspections from their accrediting agencies. Normally the thought of an inspection places staff into panic or hiding mode (“Whew, glad I’ll be off that week!”), but if you prepare ahead of time, the inspection process can be an extremely valuable tool to access the overall quality of your laboratory program. Over the next 3 blog posts we’ll review tips on 1) how to prepare before your inspection, 2) what to expect during the inspection itself, and 3) how to address any deficiencies identified by the inspection team.
Part One: The Inspectors Are Coming!
Know the Regulations. As technology evolves and new laboratory methodology is introduced, the requirements for your respective regulatory agencies will be updated as well. Know what version of your checklists or standards you will be getting inspected on, and ensure all staff are familiar with any updates and changes. By engaging all staff in the inspection process from lab assistants up through management, everyone will be aware of what the requirements are and can actively participate to ensure the lab is meeting those requirements.
Focus on Previous Citations. Your inspectors will have access to your previous inspection results, and will be following up on any citations. Ensure that the corrective actions and preventive actions you said you were going to implement have actually gone into effect. For any procedural changes, have documentation (Read & Understand) ready to show that all staff were made aware of and have been trained on the changes. Make sure that those corrections have been sustained and are effective at addressing the noted citation. It’s great to add on new forms to document instrument maintenance – but not if your staff doesn’t have the time to complete them. Again, engage your staff to see what is working, and what needs to be reevaluated.
What is New? New regulatory requirements, new staffing, new instruments, new testing methodologies… These are all key areas that the inspectors will focus on. Have you kept current with your regulatory updates and implemented any necessary changes to address the new requirements? Do you have documented training and competency for each new staff member for each task they are performing? For new instruments, ensure they have been fully validated and correlated to similar instruments prior to being placed into use for patient testing. When adding on new tests, ensure you have a full validation summary with medical director approval and sign off, and that your testing activity menu has been updated as well.
Have a Plan. Depending upon the size and scope of your laboratory, there can be a lot to cover for your inspection preparations. If you wait until your inspection window opens to start getting ready, things will be overlooked or simple “quick fixes” will be implemented instead of finding a long term sustainable solution to any potential issues. Instead, schedule tasks throughout the year to continually review your quality assurance program. Ask management to review 3 – 5 SOPs each month for content (does SOP match the current manufacturer package insert, does SOP match current practice in use), rather than a mass annual sign off. Perform quarterly reviews of your maintenance documentation to ensure all logs have been filled out completely with corrective action documented when appropriate. Utilize calendar reminders to track proficiency testing sample results, and ensure proper follow-up for any non-satisfactory results.
Perform Meaningful Self-Audits. For most regulatory agencies, performing self-audits on your non-inspection years is a requirement. Make this task meaningful by using a fresh set of eyes to review your documents. Ask the hematology staff to inspect the chemistry department; chemistry to inspect urinalysis; urinalysis to inspect microbiology…. You don’t need to understand how to actually perform a specific weekly maintenance task on a particular instrument; you just need to ensure that all those weekly tasks have been documented every 7 days (or less). You don’t need to understand what reagent ‘XYZ’ is used for, you just need to ensure that the vial is properly labeled with an open and expiration date, and that it is not currently expired and still being used. Self-audits should not be punitive; they are meant to catch things that you may be taking for granted are compliant, when in fact they truly are not.
Stay tuned for part 2 coming out next month, where we’ll discuss the inspection process itself and what to expect from the inspection team.
-Kyle Nevins, MS, MLS(ASCP)CM is one of ASCP’s 2018 Top 5 in the 40 Under Forty recognition program. She has worked in the medical laboratory profession for over 18 years. In her current position, she transitions between performing laboratory audits across the entire Northwell Health System on Long Island, NY, consulting for at-risk laboratories outside of Northwell Health, bringing laboratories up to regulatory standards, and acting as supervisor and mentor in labs with management gaps.
Several characteristics can influence a leader’s effectiveness: self-regulation, goal orientation, self-efficacy, self-awareness, and implementation intention.
Self-regulation is one of the most essential skills a leader can have. Being able to control behavior, emotions, and cognitive processes allows leaders to adapt their behavior to specific situations and interactions. Self-regulation is similar to willpower, as both act like a muscle, meaning that leader can exercise it to make it stronger. For example, a leader can practice not to be the first one to speak even though it might be their automatic behavior. Learning how to control behavior in insignificant situations will build up the ability to control them when it is critical. Increasing a leader’s willpower and self-regulatory processes will increase a leader’s situational effectiveness as it helps a leader maintain consistency and focus to deal with challenges that arise.
A leader’s goal orientation plays a significant role in their approach to learning, which, in turn, increases leadership effectiveness. Leaders with a learning goal orientation focus on developing their competence through developing new skills. Such an orientation increases a leaders’ efforts and persistence when facing challenges, which, in turn, improves the chance of a successful outcome. Goal-orientation, therefore, indicates the current and future potential of a leader.
Internal beliefs about how well one can complete a task or handle a challenge is referred to as self-efficacy. Self-efficacy is important in leadership development because it forms the attitude towards development, which guides if a leader will participate in developmental opportunities. In other words, if a leader has a self-efficacy view that they are able to communicate effectively in all situations, this leader is unlikely to participate in opportunities to further increase their communication skills.
Self-awareness is related to self-efficacy as it revolves around the understanding of a leader’s own strengths and development areas. Self-awareness essential to leadership effectiveness because leaders need to be aware of how others respond to their communication, behavior, and leadership styles. Understanding other people’s reactions through their self-awareness, leaders can adapt their behavior to the needs of each situation and person.
Implementation intention relates both to goal orientation and self-regulation. One of the challenges of leadership is starting a task or finishing one. Implementation intention strategies can help leaders with this challenge by establishing certain behaviors that lead to goal completion. Whereas goal intention is focused on reaching a specific outcome, implementation intention revolves around performing a particular behavior when encountering a certain situation. For example, a leader’s goal intention might be to stop procrastinating on answering challenging emails, while their implementation intention might be to write a draft immediately after reading a challenging email and rereading and sending the answer an hour later. Implementation orientation guides leaders towards behavioral actions that are easy to understand and act upon. Such an orientation will guide leaders to adapt their behaviors to be more effective and will allow them to fulfill their goals proactively.
When looking at this list of leadership development characteristics, which could you further develop in order to increase your leadership potential and effectiveness?
-Lotte Mulder earned her Master’s of Education from the Harvard Graduate School of Education in 2013, where she focused on Leadership and Group Development. She’s currently working toward a PhD in Organizational Leadership. At ASCP, Lotte designs and facilitates the ASCP Leadership Institute, an online leadership certificate program. She has also built ASCP’s first patient ambassador program, called Patient Champions, which leverages patient stories as they relate to the value of the lab.
In 1950 the National Safety Council began describing a safety system known as the “hierarchy of controls.” This new model was created to show that that design, elimination and engineering controls are more effective in reducing risk to workers than ‘lower level controls’ such as warnings, training, procedures and personal protective equipment (PPE). The National Institute for Occupational Safety and Health (NIOSH) began to use the hierarchy of controls, and it has been an effective safety teaching tool for that organization and others over the years. The philosophy of the hierarchy- or the pyramid- is simple: “Controlling exposures to occupational hazards is the fundamental method of protecting workers.” It is simple, and although it may not be rocket science, it’s a powerful idea.
While this hierarchy is represented differently by multiple organizations, the basic protection levels of the pyramid remain the same; Elimination, Substitution, Engineering Controls, Administrative Controls, and PPE. The most effective part of the pyramid (Elimination) is at the sharp end, or the top, and the least effective (PPE) lies at the bottom.
Unfortunately, the top two most-effective layers of the safety pyramid do not work well in the laboratory setting. We can’t eliminate or substitute the biohazards we work with- that would mean not being able to perform our work. Laboratorians handle and analyze patient samples and chemicals, and they are a necessary hazardous part of the job. There is some substitution possible in the lab when considering chemicals (the use of a non-hazardous xylene substitute, for example), but for the most part, this level of the hierarchy of controls is not very helpful to the lab.
Engineering Controls involve the use of engineered machinery or equipment which reduces or eliminates exposure to a chemical or physical hazard. Engineering Controls are definitely favored over other levels on the pyramid for controlling existing worker exposures in the workplace because they are designed to remove the hazard at the source, before it comes in contact with the worker. Well-designed engineering controls can be very effective in protecting lab employees, and they are typically independent of worker interactions so they can provide that high level of protection. Sometimes the initial price of certain engineering controls can be high, but over the longer term, operating costs are frequently lower, and the controls can ultimately provide a cost savings. Good examples of engineering controls include Biological Safety Cabinets, Chemical Fume Hoods, centrifuges, and glove boxes.
The next level of the hierarchy is represented as Administrative Controls. These controls seek to improve workplace safety by creating safer policies and procedures in the workplace. Administrative Controls can range from the placement of warning signs throughout a lab, the provision of safety training programs, and the implementation of proper ergonomics. The part of the pyramid may be the most difficult to manage. The onus of workplace safety here begins to shift from management over to staff, and sometimes the results can be… unpredictable.
An off-shoot of Administrative Controls that is discussed often in safety models is known as Work Practice Controls. These controls are not truly part of hierarchy, but they can be important safety practices in the lab setting. OSHA describes Work Practice Controls as “procedures for safe and proper work that are used to reduce the duration, frequency or intensity of exposure to a hazard.” These are the not the actual written procedures, but the actions that put those written policies into action. Following proper hand hygiene and preventing eating or drinking in the laboratory are good examples of those actions.
PPE is at the bottom of the hierarchy of controls- by definition that means that it is the least effective method to keep employees from hazard exposure. It is the last resort for safety in the lab. That’s a powerful point, and it should be discussed when providing lab safety training. All too often lab staff carelessly perform tasks without wearing PPE, and the danger is immediate and potentially disastrous. Even though this level of protection is considered the least effective, this last barrier between the employee and the hazardous material is crucial. Lab staff are required to have PPE education, and they should be able to provide a return demonstration for the proper donning and doffing of that PPE.
The Hierarchy of Controls is typically represented as a pyramid. It’s a simple symbol, but it’s really a powerful and complex model for safety. When you look at each separate level, you can see that there is a great deal of information that can provide a lab safety professional with helpful resources. As a lab leader, you can use the model to provide education, train staff, and help to enforce good safety behaviors which will improve the lab safety culture and keep employees from harm.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.