Once again Maryn McKenna–blogging with National Geographic now–breaks down the Anglo-Saxon remedy for eye infections that set the antibiotic community ablaze last week. In short: effectiveness is one thing; getting it to market is another. You can read the full post here.
Category: microbiology
Microbiology Case Study–Pleural Thickening in Lung Transplant Patient
Case history:
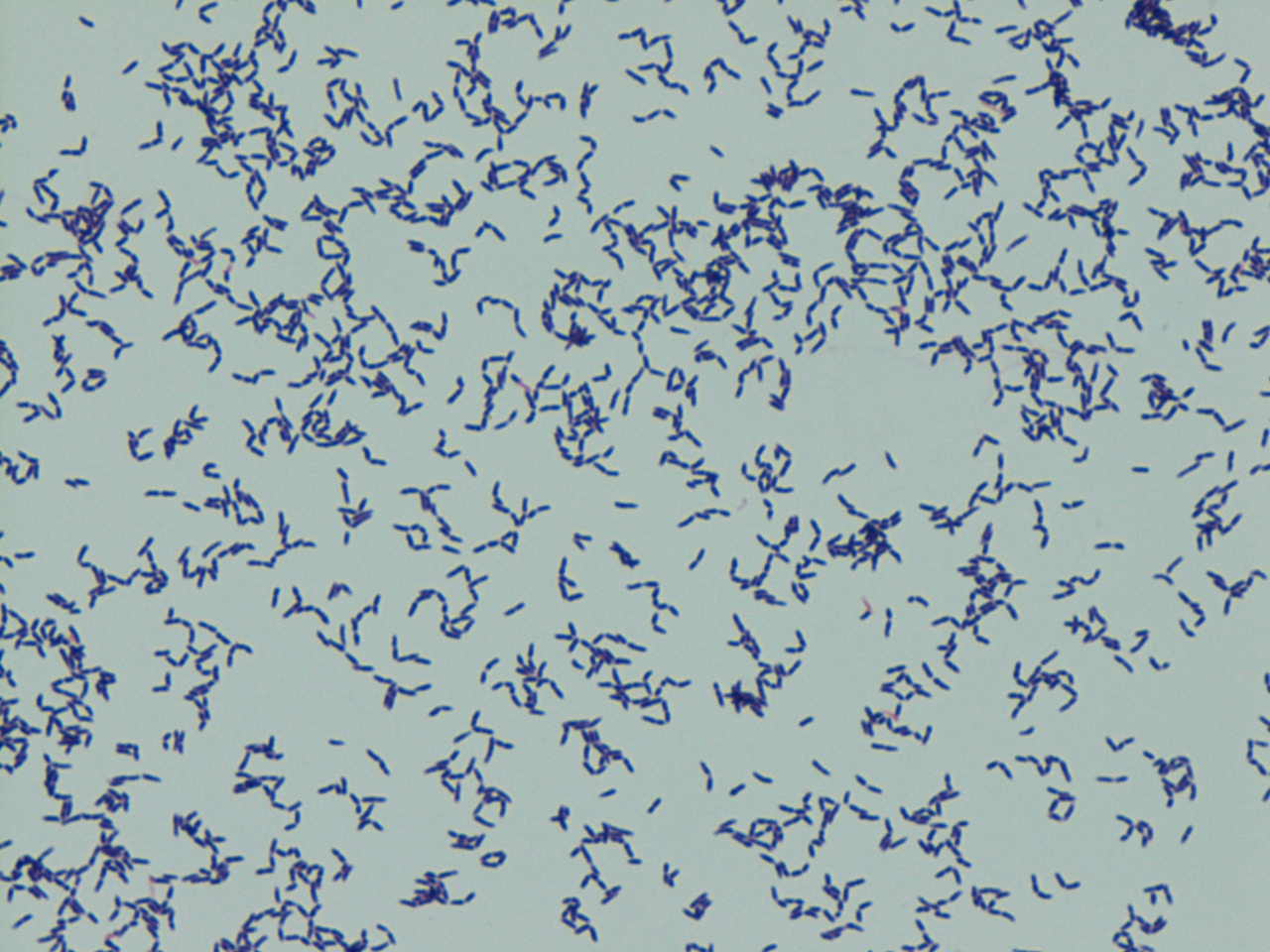
A 71-year-old man with a past medical history of idiopathic pulmonary fibrosis and asbestosis status post recent single lung transplant presented with worsening dyspnea. He had a right pleural catheter since the time of his lung transplant surgery five months ago. A chest CT scan was performed and revealed a right pleural effusion with pleural thickening. A sample of the pleural fluid was sent to the microbiology laboratory with the following gram stain and colony morphology:


Laboratory Identification:
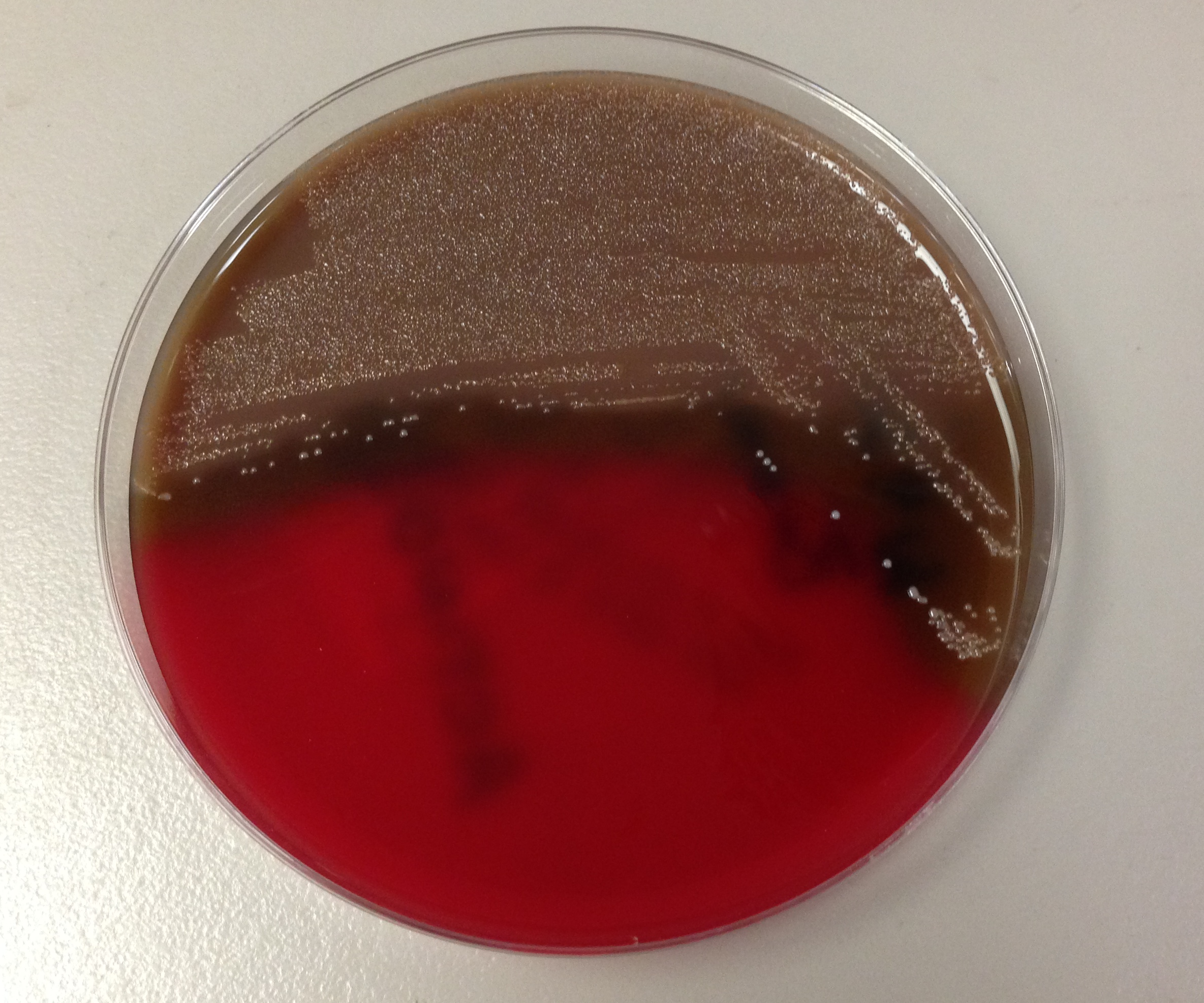
The pleural fluid grew bacterial colonies on blood agar plates as shown above. No growth was present on MacConkey agar (selective for gram negative bacteria). The colony morphology and gram stain was suggestive of Corynebacterium species. Mass spectrometry confirmed the bacteria as Corynebacterium striatum.
Discussion:
Corynebacterium striatum are gram-positive bacilli that are normal skin and mucosal membrane flora. C. striatum is commonly regarded as a contaminant but may be an opportunistic pathogen in immunocompromised patients such as the patient presented in the above case. Transmission of C. striatum most likely occurs when the patient’s endogenous strain gains access to a normally sterile site of the body. C. striatum has also been documented to spread nosocomially in patients with severe chronic obstructive pulmonary disease. C. striatum is associated with a spectrum of diseases including infectious endocarditis, bacteremia, pneumonia, lung abscess, arthritis, chorioamnionitis and foreign medical device infections. Patients with C. striatum infections are empirically treated with vancomycin because the susceptibility to other antibiotics is variable. Additionally, removal of foreign medical device should be performed if indicated.
Jill Miller, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Microbiology Case Study–Infection at Wisdom Tooth Extraction Site
Clinical
56 year old male with stage IV chronic kidney disease, hypertension, and gout who underwent a left lower wisdom tooth extraction presented two days post-op with throbbing pain on left side of his face and neck, dysphagia and dyspnea. He was sent to an outside ED by his dentist. He was given 900 mg of clindamycin, a dose of steroids and pain management and was sent to our institution. Surgical site was intact, but there was massive swelling of the floor of the mouth, submandibular gland, and neck. Symptoms worsened despite being given IV clindamycin. Infectious disease was consulted he was started on meropenem and blood cultures were drawn.
Microbiology
Two anaerobic blood culture bottles became positive at 48 and 61 hours.
Gram stain:


Plates:



Discussion:
Two organisms were identified.
Organism 1: Fusobacterium nucleatum – anaerobic gram-negative, non-spore-forming rods. They are pale-staining, long, slender, spindle-shaped rods with sharply pointed or tapered ends; occasionally the cells occur in pairs end to end. Sometimes there are spherical swellings. Cells are usually 5-10 µm long, but can be shorter. They grow well on anaerobic blood agar plates under anaerobic conditions and are killed readily by exposure to ambient air. Colonies on anaerobic blood agar are 1-2 mm in diameter, slightly convex with slightly irregular margins and have a characteristic internal flecking referred to as “crystalline internal structures”. They can have three morphologies: bread crumblike (white), speckled, or smooth (gray to gray-white). There is greening of the agar on exposure to air, they are usually nonhemolytic and fluoresce chartreuse under UV light.
The Fusobacterium species are normally found in the upper respiratory, gastrointestinal, and genitourinary tracts of humans. They are common causes of serious infections in multiple body sites. They are associated with infections of the mouth, bite wounds, and respiratory tract. F. nucleatum are the most frequently involved in anaerobic pleuropulmonary infections (aspiration pneumonia, lung abscess, necrotizing pneumonia, thoracic empyema). They are also fairly common pathogens in brain abscesses, chronic sinusitis, metastatic osteomyelitis, septic arthritis, liver abscess, and other intraabdominal infections. Fusobacterium nucleatum is the species most commonly found in clinical materials. It can cause severe systemic infection in patients with neutropenia and mucositis following chemotherapy.
They can be differentiated from similar species of Bacterioides, Prevotella, Porphyromanas, and Leptotrichia by their production of butyric acid but not isobutyric or isovaleric acid. Bacterioides and Porphyromanas species produce all three acids.
Organism 2: Parvomonas micra – formerly called Peptostreptococcus micros or Micromonas micros, are anaerobic, gram-positive cocci, <0.7 µm in diameter; occur in packets and short chains. Grow on anaerobic blood agar. Colonies are tiny, white, opaque, nonhemolytic. This is a periodontal pathogen that contributes to periodontitis.
Kirsten J. Threlkeld, MD is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Illinois Summit on Antibiotic Stewardship
Last week, I attended the Illinois Summit on Antimicrobial Stewardship at Northwestern Memorial Hospital. While the target audience was physicians, nurses, pharmacists, and administrators, as a clinical laboratory scientist I found the presentations (with a few caveats, which I’ll get to in a moment) quite informative.
The morning sessions covered the relationship between antibiotic use and resistance patterns; interpretations and implementation of the national guideless for stewardship; and using behavioral science to increase compliance with stewardship programs. Participants spent part of the afternoon in small groups to discuss designing and implementing a stewardship program.
A few notes:
-50% of antibiotics for upper respiratory infections aren’t needed; 50% of antibiotics for inpatients aren’t needed, either
-antibiotics are the only drug where use in one person impacts it effectiveness in another
-based on the literature, antibiotic stewardship programs have at least a transient effect on antibiotic effectiveness—eventually, resistance numbers begin to climb again
-hospital antibiograms are the most widely available measure of resistant organisms, but we aren’t using them as effectively as we could. For example, we typically report that, say, “62.5% of E. coli isolates are resistant to ciprofloxacin,” but we don’t say where those isolates come from. Are they urinary tract infections or upper respiratory infections? What’s the rate of resistance for infected wounds?
-a weighted antibiogram might make empirical treatments for effective. For example, “what % of urinary tract infections are resistant to ciprofloxacin?”
-it’s important to note that the IT department, hospital information systems, and laboratory information systems play a huge role in stewardship programs
-stewardship programs depend on the “5 D’s” Diagnosis, drug selection, dose, duration, and de-escalation of use
-diagnostic uncertainty—driven by lack of early organism identification—drives a significant amount of antibiotic use
-when combined with stewardship, rapid bacterial identification methods such as MALDI-ToF platforms decrease parameters such as length of patient say, time to treatment, etc.
-we can use peer pressure to drive improvements. No one wants to perform worse than the doctor next door
-our efforts might be moot, anyway; other countries take a much laxer stance on antibiotic use
While the laboratory in general and clinical microbiology departments specifically were mentioned during the presentations, I must say they were only mentioned in the context of how little perceived impact we have on stewardship. (“Well, we know the laboratory isn’t going to give us any useful information for another three days…”) It wasn’t until I participated in the small group sessions in the afternoon that attendees at my table admitted that the laboratory is an important piece of the stewardship puzzle. We have mountains of data we can assimilate (antibiogram creation, anyone?). We can bring in new technologies to make identifications faster. We can work closely with the infectious disease doctors to help guide treatment. That brings up a good point—if microbiology labs aren’t in-house, then creating an antibiotic stewardship program becomes that much harder because results can be delayed.
If you’d like to see the powerpoints from the presentations, you can do so by clicking the “downloadable content” tab at Northwestern Memorial Hospital’s antibiotic stewardship page.

–Kelly Swails, MT(ASCP), is a laboratory professional, recovering microbiologist, and web editor for Lab Medicine.
Microbiology Case Study–Diabetic Foot Ulcer
A 68 year old woman with a past medical history of type 2 diabetes mellitus presented with a foot wound clinically consistent with a diabetic foot ulcer. Imaging of the patient’s foot demonstrated a large abscess of the plantar aspect of her foot with extension to the surrounding soft tissues. The patient was taken to the operating room and incision and drainage was performed. Fluid from the wound was submitted to the microbiology laboratory and was planted aerobically and anaerobically. Growth was observed on the anaerobic blood plate with the below gram stain and colony morphology:
Laboratory Identification:
The fluid received from the patient’s wound was cultured on aerobic and anaerobic grow plates. The bacteria only grew on anaerobic plates. Additionally, the gram stain revealed pleomorphic gram positive bacilli. These findings were suggestive of Actinomyces. Actinomyces species was confirmed by mass spectrometry.
Discussion:
Actinomyces are anaerobic gram positive bacteria that are normal flora of the oral cavity and throat. Actinomyces have variable gram stain and colony morphology. Our case, as shown above, demonstrates the pleomorphic nature of Actinomyces and does not exhibit the classic textbook morphology. The typical gram stain morphology of Actinomyces is branching, filamentous, beaded bacilli. This morphology overlaps with Nocardia. Actinomyces can be distinguished from Norcardia based on its anaerobic growth pattern and lack of partial acid fast staining (Nocardia are strict aerobes that stain partially acid fast). The bacterial colonies of Actinomyces are non-hemolytic, non-pigmented and are classically described as white and nodular (molar tooth shaped). Actinomyces forms “sulfur granules” in patient specimens which are hard yellow granules composed of bacterial filaments solidified with exudative material.
Actinomyces has the potential to cause opportunistic infections when transferred from an endogenous site to a sterile site of the body. Actinomyces is involved in a spectrum of human disease including actinomycosis, wound infections, abscesses, oral infections, genital tract infections, and urinary tract infections. Of these diseases, actinomycosis is the most infamous and is characterized by abscess formation, draining sinus tracts with sulfur granules, and tissue fibrosis. Actinomycosis is most commonly cervicofacial, but may also be thoracic, abdominal, pelvic or involve the central nervous system.
Treatment of Actinomyces includes surgical debridement if indicated and prolonged antibiotics for 3-6 months depending on antibiotic sensitivity. Antibiotic sensitivity ranges from penicillin, amoxicillin, tetracycline, erythromycin, and clindamycin.
Jill Miller, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A Potential Paradigm Shift for Strep Cultures?
In a study published a few days ago in the Annals of Internal Medicine, researchers discuss the prevalence of Fusobacterium necrophorum in students with pharyngitis. Typically, severe sore throats are attributed to Streptococcus Group A, C, or G; however, sometimes patients can be symptomatic but negative for these three pathogens. The study authors found F. necrophorum in 20.5% of their symptomatic population (312 students aged 15 to 30 years).
This study does raise an interesting question: should micro labs inoculate a CDC plate as well as a blood plate for strep cultures? This organism is susceptible to penicillin, so the treatment course is the same as for typical strep throat, which would indicate the CDC isn’t really needed. However, as this Healthday article indicates, F. necrophorum infections can lead to Lemierre’s syndrome, a rare but serious complication. Knowing the causative agent of a sore throat would be beneficial.
–Kelly Swails, MT(ASCP), is a laboratory professional, recovering microbiologist, and web editor for Lab Medicine.
Microbiology Case Study–Back and Flank Pain in a Transplant Patient
Clinical Summary:
59 year old male with a history of acute myeloid leukemia, status post allogeneic bone marrow transplant complicated by graft-versus-host disease and relapse presented to the ED complaining of flank and back pain. His work-up identified multiple pulmonary lesions, thought to be infarcts and a left upper extremity deep vein thrombosis. He was started on cefepime for neutropenic fever and lovenox for the emboli. His symptoms worsened and imaging revealed progressive lesions in the lung that were concerning for invasive aspergillosis. A biopsy of one of the lesions was non-diagnostic but an aspergillus serum antigen test was positive. He was started on voriconazole. He remained hospitalized and began showing improvement, but then again developed a febrile neutropenia and became hypotensive with a decreased hemoglobin level. A CT of the abdomen showed typhlitis in the cecum and possible liver phlegmons, and a CT of the chest showed bilateral pulmonary effusions. He went into respiratory failure and passed away. An autopsy was performed and they sent lung tissue for fungal cultures.
Microbiology:
Plates:
Temperature Studies:
The mold grew at both 37° and 42°C.
Discussion:
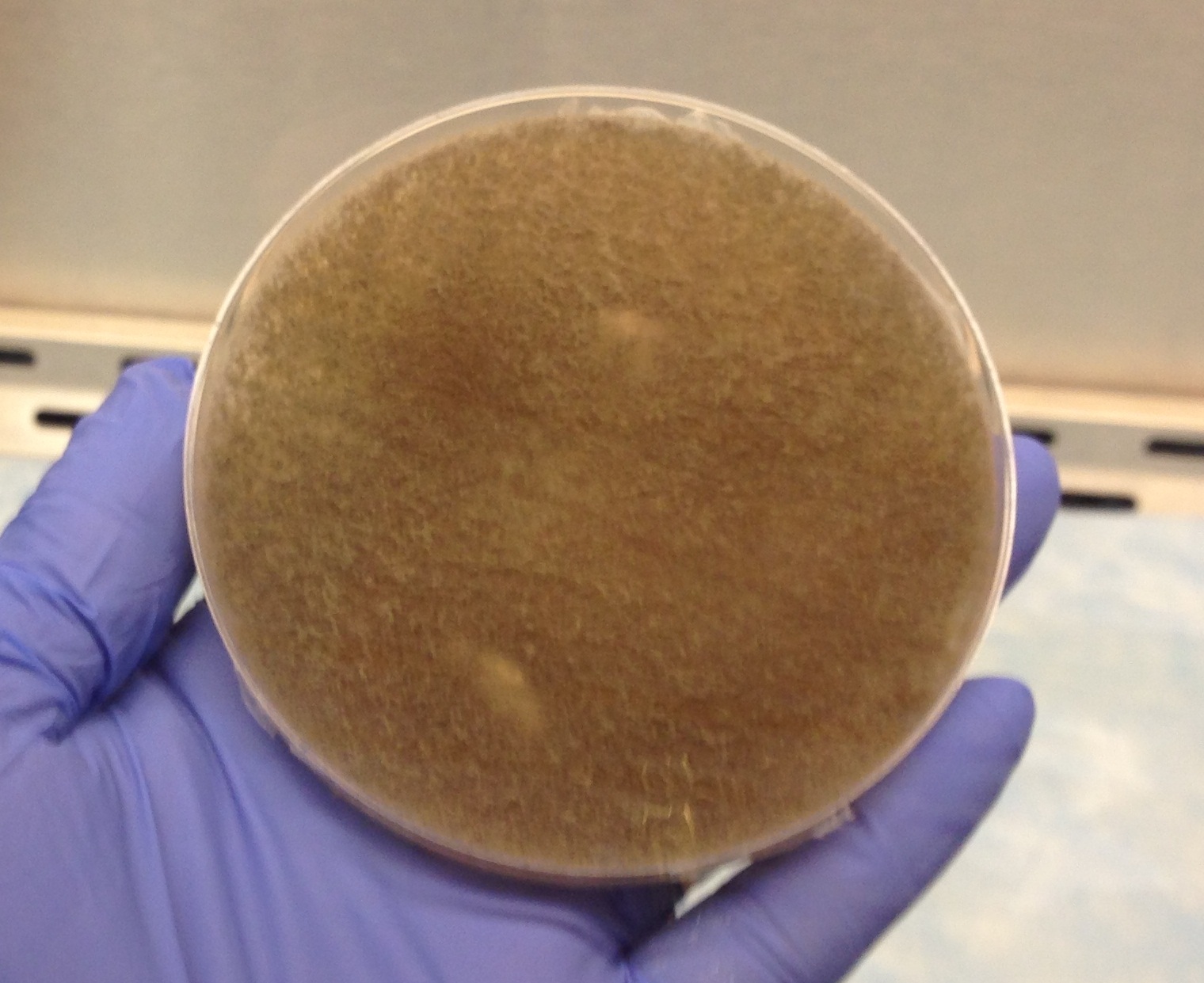
The above findings lead to the classification of a Zygomycete which are hyaline, pauciseptate molds that include Rhizopus, Mucor, Absidia, Rhizomucor, Synecephalastrum, Cunninghamella, and others.
The colonies are fluffy, white to gray or brown. They are rapid-growers and diffusely cover the agar within 24-96 hours. The hyphae appear to be coarse and fill the entire culture dish with loose, grayish hyphae dotted with brown or black sporangia. It is not possible to differentiate the organisms based on colony morphology. Temperature studies can differentiate between some species: Rhizopus grows best between 40-50°C; Rhizomucor grows best around 38-58°C; Mucor grows best at less than 37°C; Absidia grows between 45-50°. Since our specimen grew at both 37° and 42°C, that would lead us to have Rhizomucor high on our differential.
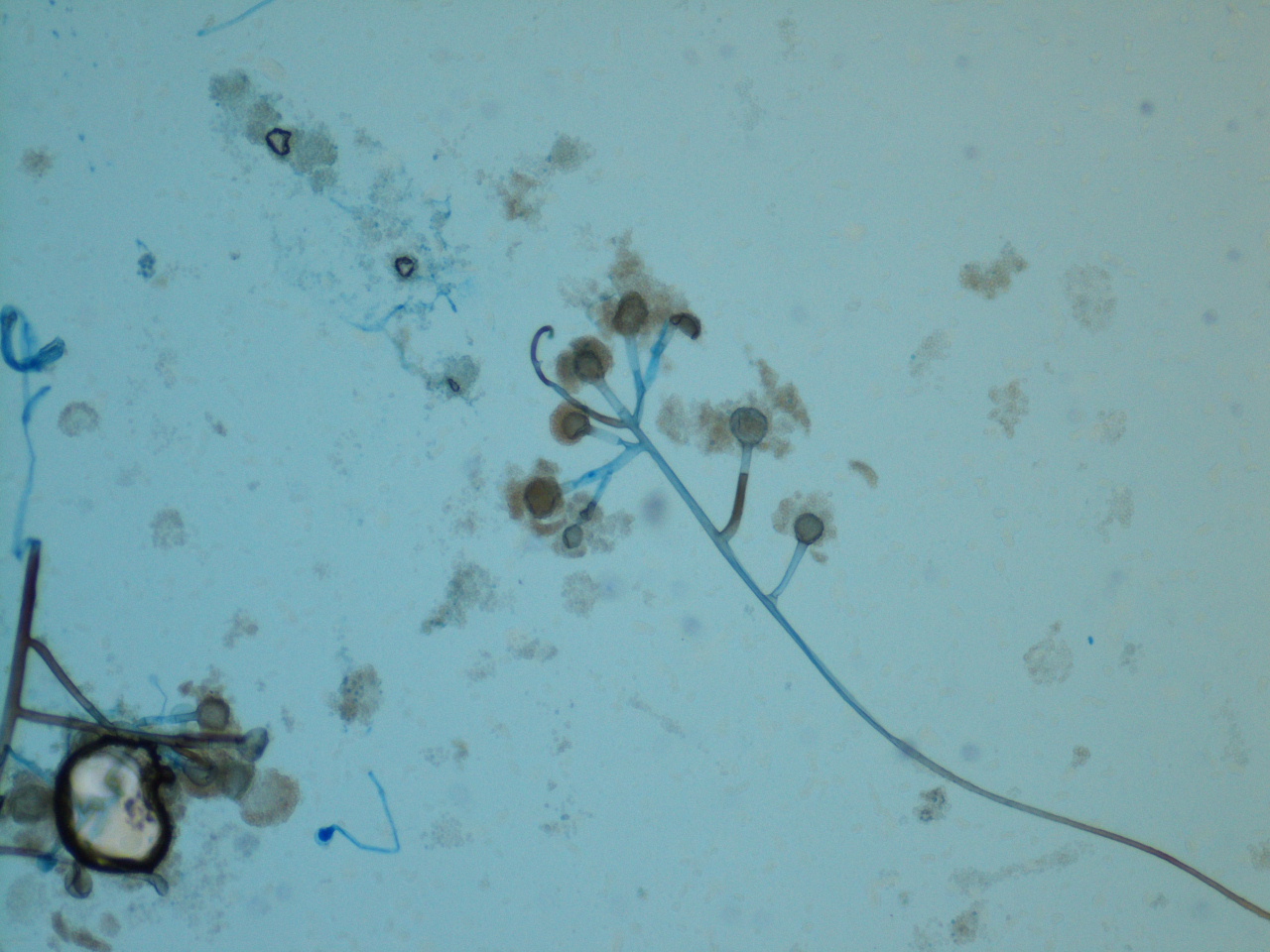
Zygomycetes produce large, ribbon-like hyphae that are irregular in diameter and contain occasional septae. Classification of specific organisms relies on identifying the characteristic saclike fruiting structures called sporangia. The sporangia produce sporangiospores, which are within the sporangia and are spherical and yellow or brown. Each sporangium is formed at the tip of a sporangiophore which is a supporting structure. The sporangiophores are connected by hyphae with occasional septations called stolons. These are contact points where rootlike structures called rhizoids attach to the hyphae. The presence and location of the rhizoids helps to identify the organism. Rhizopus has unbranched sporangiophores with rhizoids at their base where the stolon arises. Mucor has singularly produced or branched sporangiophores that have round sporangium filled with sporangiospores at their tips. It does not have rhizoids or stolons. Absidia has rhizoids that are between sporangiophores, and the sporangia are pyriform and have a funnel-shaped area called apophysis at the junction of the sporangium and the sporangiophore. Usually a septum is formed in the sporangiophore just below the sporangium. Our microscopic exam did not show any rhizoids at first, but a second exam after a longer growth period showed potential rhizoids at the base of the sporangiophores, which would lead us to have Rhizopus on our differential. Our case did not clearly define itself at the species level, so it was signed out as a Zygomycete and there were no treatment implications.
Zygomycetes are not a common cause of infection, but are an important cause of morbidity and mortality in patients who are immunocompromised. They have a worldwide distribution and are commonly found on decaying vegetable matter, soil, or old bread. Infection occurs by inhalation of spores, and once established, it is rapidly progressive, particularly in patients with diabetes mellitus who have infections that involve the sinuses. The organisms have a propensity for vascular invasion and rapidly produce thrombosis and necrosis of tissue. A common presentation is invasion within the nasal mucosa, palate, sinuses, orbit, face, and brain showing massive necrosis with vascular invasion and infarction. Perineural invasion can also occur which can spread retro-orbitally into the brain. They can also infect the lungs and GI tract as well as have disseminated infection. They can cause skin infections in patients who have severe burns and infections of subcutaneous tissue of patients who have undergone surgery.
Follow up:




The histology on H&E stain shows areas of necrosis with faint septate hyphae as well as broad, ribbon-like hyphae within the vasculature. The silver stain nicely highlights the broad hyphae which we can identify as a zygomycete. The silver stain also accentuated the massive amounts of thinner hyphae with parallel walls and 45 degree branching which is consistent with aspergillus. This patient was found to have both an aspergillus infection which caused the positive serum antigen test, but then also developed a zygomycete infection which led to his death. We did not identify aspergillus on our fungal culture which may be explained by several possibilities. Our patient had been treated with voriconazole for a potential aspergillus infection which may make it more difficult for the aspergillus to grow on fungal culture. Zygomycetes are rapid growers which could have inhibited the growth of another organism or could have inhibited our ability to identify a second organism growing on the plate.
Kirsten Threlkeld, MD is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Doctor, There’s a Snake in My Poop
Case history:
A mother brought her 5 year old son into his pediatrician with a “snake” that she found in his stool. Otherwise, the patient was completely asymptomatic.
Specimen sent for ID:


Ascaris is the most common Helminth affecting humans. It is also the largest of the roundworms (nematodes), growing up to 35 cm in length. There are several species of Ascaris however only A. lumbricoides affects humans.
Epidemiology
Ascaris occurs in areas with poor sanitation, hygiene and solid waste practices. Worldwide it is most common in tropical and subtropical areas.
Transmission & Life Cycle
Ascaris is transmitted through the fecal-oral route, and is therefore most prevalent in areas with poor sanitation and waste practices. Transmission occurs when an uninfected person swallows a fertilized egg which was originally passed through the stool of an infected person.
The adult male and female forms live in the small intestine. The female passes up to 200,000 eggs per day. If there is also a male worm living in the small intestine, these eggs may then be fertilized. Both fertilized and unfertilized eggs are eventually passed in the stool.
Unfertilized eggs are not infective and do not cause disease if ingested. Fertilized eggs are only infective after approximately three weeks of maturation. The exact amount of time required before the fertilized egg becomes infective will depend on environmental conditions, such as temperature and humidity.
Once ingested, the fertilized egg travels to the small intestine, where it hatches and becomes a larva. The larval form invades the small intestinal mucosal wall and enters the bloodstream. Upon reaching the lung, the larva invades the capillary and alveolar walls and continues to grow within the alveoli. After about two weeks of maturation, the larva then migrates up through the airspaces and into the trachea, where it is eventually swallowed and transported back down into the small intestine. The fully mature larval forms are now adult worms and will continue to live in the small intestine for the rest of their lifespan (up to 1 to 2 years).
Laboratory Diagnosis
In most cases, Ascaris is diagnosed in the egg form on ova and parasite exam. The fertilized egg is round, 45-70 microns in diameter and has a thick, mammillated outer wall which stains brown with bile. The unfertilized egg is larger (90 microns), are has a more oval shape with a less regular mammillated contour. Patients may also pass adult worms in the stool or less commonly they may cough them up through the mouth. The adult worms have tapered ends with a three-lipped mouth (“tricuspid” mouth). The female is larger than the male (female: 20-35 cm, male: 15-30 cm).
Clinical Symptoms
Clinically, most people affected with Ascaris are asymptomatic. With a very high worm load however patients may begin to develop complications related to obstruction, including abdominal pain, constipation, appendicitis and obstructive cholangitis. In younger children infection with Ascaris may result in stunted growth. Of note, immune reaction to larva in the lung may result in an eosinophilic immunologic response known as Löffler’s pneumonitis.
Treatment
Ascaris is treated with anthelminthic medication (albendazole, mebendazole or ivermectin). Therapy for Ascaris extremely effective and rids the patient of all adult, larval and egg forms.
-Javier De Luca-Johnson, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
–Christi Wojewoda, MD, is certified by the American Board of Pathology in AP/CP and Medical Microbiology. She is currently the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
CLSI and APHL to Co-Host 12th Annual AST Update Webinars
From the press release:
The Clinical and Laboratory Standards Institute (CLSI) and the Association of Public Health Laboratories (APHL) will co-host the 12th annual educational update webinars for antimicrobial susceptibility testing (AST).
Each January, CLSI updates standards for AST. It is important for clinical laboratories to incorporate the new recommendations into routine practice to optimize detection and reporting of antimicrobial resistance. In January 2015, the annual update of the M100 AST tables (CLSI document M100-S25) was published. In addition, the standards that describe performance of disk diffusion and minimal inhibitory concentration tests in versions M02-A12 and M07-A10, respectively, were updated. Some highlights for 2015 include introduction of the Carba NP test for carbapenemases and expanded recommendations for quality control testing.
These changes and several other new recommendations found in M100-S25, M02-A12, and M07-A10 will be discussed during the webinar. In addition to the webinar, an optional postprogram self-assessment will be provided that will allow individuals to assess their knowledge regarding the most important AST and reporting issues for 2015. Laboratories can use this feature to augment competency assessment requirements for their staff.
The webinar will be led by Janet A. Hindler, MCLS, MT(ASCP), Senior Specialist, Clinical Microbiology, at the UCLA Health System in Los Angeles, California, USA.
Webinar information is as follows:
The webinar will be led by Janet A. Hindler, MCLS, MT(ASCP), Senior Specialist, Clinical Microbiology, at the UCLA Health System in Los Angeles, California, USA.
Webinar information is as follows:
CLSI 2015 AST Update
February 4, 2015 • 1:00–2:30 PM Eastern (US) Time
February 5, 2015 • 3:00–4:30 PM Eastern (US) Time (repeat session)
February 4, 2015 • 1:00–2:30 PM Eastern (US) Time
February 5, 2015 • 3:00–4:30 PM Eastern (US) Time (repeat session)
Learner Level: This intermediate-level program is appropriate for laboratory professionals working in clinical and academic settings.
At the conclusion of this program, participants will be able to:
- Identify the major changes found in the new CLSI document M100-S25.
- Design a strategy for implementing the new practice guidelines into their laboratory practices.
- Develop a communication strategy for informing clinical staff of significant AST and reporting changes.
Register for the upcoming webinars at www.aphl.org/clsi.
Microbiology Case Study
Patient History:
81 year old man with a history of systemic vasculitis (present for the past 10 years ANCA negative, ANA negative, Rheumatoid factor <20) on immunosuppression (plaquenil with prednisone 40mg for flares about every 6 months), type 2 diabetes, and hypertension presented to an outside hospital with weakness and dyspnea. He was found to have a widespread purpura, ulcerative lesions, acute kidney injury (creatinine 4.7), and 3 days of hematochezia. He was started on 7 days of levoquin and zosyn for a presumed pneumonia and with no improvement was transferred to our institution. On admission, a CT scan of the chest demonstrated bilateral multifocal pneumonia and multiple cavitary nodules within the lungs. A thoracentesis was performed and was transudative (wbc 1883, N 63%, protein 2.6).
Laboratory findings:
- WBC 7000/cmm
- Hemoglobin 9 g/dL
- Platelet count 104 K/cmm
- Bacterial culture blood, no growth
- Cryptococcal antigen negative
- Pleural fluid bacterial culture and smear negative
- Pleural fluid AFB culture and smear – no acid fast bacilli, modified acid fast bacilli seen from bottle
- Pleural fluid fungal culture and smear – no fungi seen, rare modified acid fast bacilli growing
- Histoplasma urinary antigen positive
- Histoplasma antibodies negative
- Blastomyces urinary antigen negative



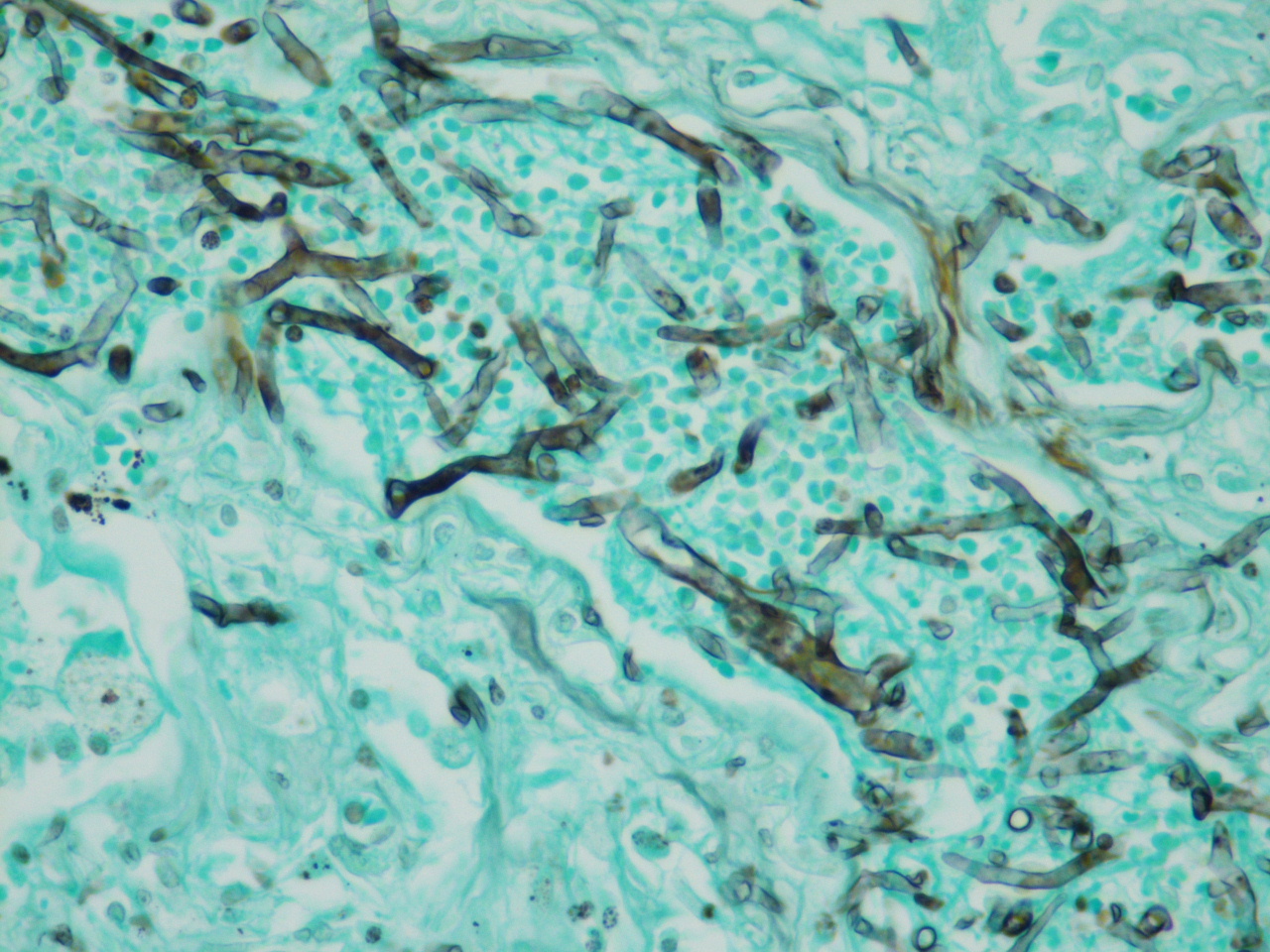
Discussion:
Based on Gram stain and modified acid fast stain, modified acid fast bacilli suggestive of Nocardia species was reported. Nocardia are strict aerobic, gram positive, filamentous rods that stain partially acid fast. This is due to the mycolic acids in the cell wall which are shorter than those of mycobacteria. Nocardia species produce many virulence factors including Cord factor (prevents intracellular killing), catalase and superoxide dismutase (which inactivate reactive oxygen species that would otherwise prove toxic to the bacteria).
Nocardia grow well on buffered charcoal yeast extract agar and at 30oC. They produce aerial hyphae and can have a chalky colony appearance. Species level identification is best done with molecular methods. This isolate was identified as Nocardia farcinica at a reference laboratory.
Nocardia species are ubiquitous in the soil. They can cause infections in immunocompromised hosts usually after inhalation or direct inoculation. Infections include bronchopulmonary disease and cutaneous infections. With bronchopulmonary disease, cavitation and spread to the pleura is common, which fits with our patient. Dissemination is also seen with common sites being brain and subcutaneous tissue.
Our patient had a positive Histoplasma urinary antigen, but negative Histoplasma antibodies. The working diagnosis was disseminated Histoplasmosis and he was being treated with amphotericin B. He expired and no postmortem exam was performed. Fungal cultures from the pleural fluid were not growing fungus at the time of this post. Fungal cultures were not obtained from sputum and a BAL was not performed.
-Dan Olsen, MD is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
