Insulin antibodies are seen in two conditions: 1, in insulin-naïve type-1
diabetic patients, insulin antibodies are developed together with some other
autoantibodies against pancreatic islet cells; 2, in patients being treated
with insulin, antibodies can be developed against exogenous insulins, in both
type-1 and type-2 diabetes. These antibodies against exogenous insulins are
found in >95% of patients treated with porcine and bovine insulins (1).
Although the prevalence has decreased after the introduction of human insulin
and insulin analogues, it is still not uncommon to detect these antibodies in
insulin treated patients (2). However, these antibodies are rarely of clinical
significance and laboratory test for insulin antibodies in insulin-treated
patients has limited clinical value, except in rare cases where these
antibodies are found to have immunologic role, causing insulin resistance. In
some of these cases, postprandial hyperglycemia and nighttime hypoglycemia are
both described due to reversible binding of insulin from antibodies (3), and
patients were reported to respond to immunosuppressive therapies, and plasmapheresis
in severe cases.
We recently
worked up a case for possible immunologic insulin resistance caused by insulin
antibodies. In this case, patient is a 45 years old female with uncontrolled
type-1 diabetes. She was found to have all four antibodies positive, including
zinc transporter 8, islet
antigens glutamate decarboxylase 65 (GADA), IA-2A, and insulin antibodies. Patient
has been on multiple dose insulin injection (MDI) therapy, including insulin
determir, aspart and lispro. She was reported to be compliant with medications
and low carb diet. However, patient has poor glycemic control and presents with
recurrent diabetic ketoacidosis. She was given high doses of insulins, but
still presented with recurrent DKA and occasional hypoglycemia. Her HbA1c was
consistently at >10% with daily glucose measured up to 500 mg/dL.
Immunologic
insulin antibody and insulin receptor antibody were considered after ruling out
more common causes of her uncontrolled diabetes. These two tests were then performed
at a reference laboratory and patient was found to have positive insulin
antibodies to analog insulin (determir and lispro) and negative insulin
receptor antibodies. Significant insulin resistance by insulin antibodies was
not found and the antibodies level did not suggest immunosuppressive therapy. Still,
given her poor controlled diabetes, patient’s insulin was switched to human
insulin and she was also recommend for pancreas transplant.
Greenfield JR, Tuthill A, Soos
MA, Semple RK, Halsall DJ, Chaudhry A, O’Rahilly S. Severe insulin
resistance due to anti-insulin antibodies: response to plasma exchange and
immunosuppressive therapy. Diabet Med. 2009 Jan;26(1):79-82. doi:
10.1111/j.1464-5491.2008.02621.x.
Hall TR, Thomas JW, Padoa CJ, Torn
C, Landin-Olsson M, Ortqvist E, Hampe CS. Longitudinal epitope analysis of
insulin-binding antibodies in type 1 diabetes. Clin Exp Immunol. 2006
Oct;146(1):9-14.
Hao JB, Imam S, Dar
P, Alfonso-Jaume M, Elnagar N, Jaume JC. Extreme Insulin
Resistance From Insulin Antibodies (Not Insulin Receptor Antibodies)
Successfully Treated With Combination Immunosuppressive Therapy. Diabetes
Care. 2017 Feb;40(2):e19-e20. doi: 10.2337/dc16-1975. Epub 2016
Dec 1.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist, currently serving as the Co-director of Clinical Chemistry at Houston Methodist Hospital in Houston, TX and an Assistant Professor of Clinical Pathology and Laboratory Medicine at Weill Cornell Medical College.
An African American male in his early 20s presented to the emergency
department (ED) with complaints of a sore throat, headache, generalized body
aches, and fatigue for the past week. He also noted intermittent fever and
chills as well as some nausea with a decrease in his appetite. He had been seen
multiple times in the ED recently for similar symptoms. His past medical
history was non-contributory and he noted no significant travel or exposure
history with the exception of attending a local party 10 days ago. His
temperature was 100.5°F and vitals were otherwise normal. His physical exam was
normal with the exception of dry mucous membranes indicating mild dehydration. Initial
laboratory testing showed a leukopenia (white blood cell count of 1.5 TH/cm2)
with 39% lymphocytes and rapid antigen testing for group A Streptococcus, influenza, and infectious mononucleosis were
negative. The patient was admitted for further work up due to the prolonged
nature of his symptoms.
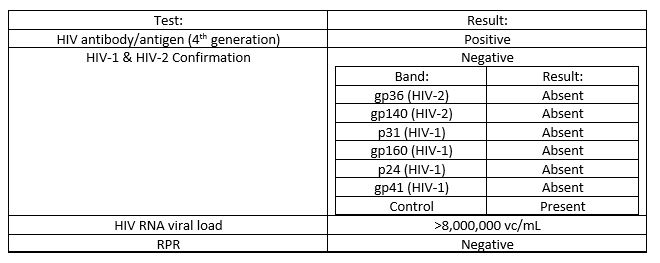
Laboratory Identification
Results from additional infectious disease testing are in the table
below.
This pattern of results is most consistent an acute HIV infection.
Discussion
Human immunodeficiency virus (HIV) is an enveloped, single stranded RNA
virus which belongs to the family Retroviridae.
HIV is most commonly sexually transmitted via body fluids such as blood, semen,
and vaginal secretions directly contacting mucosa membranes. HIV can also be
transmitted due to needle stick injuries, blood transfusions, and
transplacentally from infected mother to fetus or by breast feeding. Acute HIV
illness presents as a mononucleosis-like syndrome with fever, pharyngitis,
arthralgias, malaise, and weight loss. During this acute illness, the HIV RNA
viral load is extremely high. After a period of clinical latency, which on
average is approximately 10 years, there is a deterioration of the immune
system, the CD4 count drops, and the patient is at risk for opportunistic
infections and neoplastic diseases.
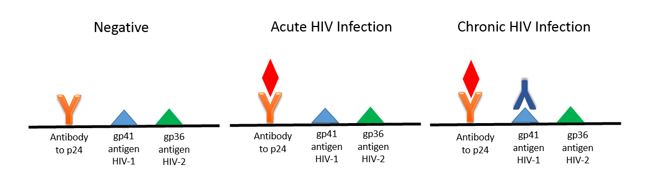
Based on the 2014 CDC/APHL guidelines, the initial screening test for
HIV is an antigen-antibody combination assay. These immunoassay based tests
detect the p24 antigen and antibodies to HIV-1 and HIV-2 (see image below). By
testing for the p24 antigen in addition to HIV antibodies the time to a
positive patient result is decreased (window period) as p24 is one of the first
viral proteins to appear, even before antibodies are present.
If the antigen-antibody test is repeatedly positive, the second step in
the testing algorithm is an antibody differentiation assay. This test has taken
the place of the Western blot and Western blot is no longer recommended in the
diagnosis of HIV. If the antibody differentiation test is positive, the
diagnosis of HIV-1 or HIV-2 is confirmed. As this step only detects the
presence of antibodies, the differentiation test will be negative in an acute
HIV infection.
If there is a discrepancy between the first two steps in the testing
algorithm or an indeterminate result is obtained, the final step involves
nucleic acid amplification testing (NAAT) to detect viral RNA. Viral RNA is the
first HIV-1 specific marker to appear following infection. In the case of an
acute or untreated long term infection, the viral load can approach levels up
to 100 million copies.
When additional history was obtained from our patient, he said he was
sexually active with a new male partner in the past few weeks and did not use
protection. He stated he had been treated with Chlamydia in the past. Further testing for CD4 count, other
opportunist & sexually transmitted infections, and HIV genotype testing was
performed and outpatient HIV care was arranged for the patient.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.
For transgender women, taking pills of estradiol is
insufficient to counteract the endogenous levels of testosterone produced by
their bodies. To counteract the undesired testosterone, anti-androgens are
employed. These include cyproterone acetate (approved only in Europe) or
spironolactone. Spironolactone is a potassium sparing diuretic that could have
unintended consequences like gynecomastia.1 This effect comes from
off-target binding of spironolactone to the androgen receptor. Like the
intended spironolactone target (mineralocorticoid receptor), the androgen receptor
localizes to the nucleus when activated and acts as a transcription factor.
Taking daily high doses of spironolactone
(100mg- 300mg daily) has been shown to be safe,1 but can increase
Potassium levels. In a cohort of 55 transgender women, potassium was actually
not higher (Figure 1).2 This was the first time a study had
rigorously measured electrolytes like potassium in transgender patients.
Current guidelines recommended checking electrolyte levels in transgender women
taking spironolactone.3 Full electrolytes were included for 126 TW
in our study and what we found was not what we were expecting.4
Figure 1.
We found no increased potassium levels in TW who had taken
hormone therapy for at least 6 months (p>0.05). However, we did see a
decrease in sodium which is consistent with the diuretic effect (p<0.0001, Figure
2).
Figure 2.
We wondered if variability in spironolactone dosing could explain why no significant potassium change was found. Luckily, we had a large number of patients who were taking various doses of spironolactone for comparison. One-way ANOVA with Tukey post-hoc tests revealed no difference in potassium levels (p>0.05)- even between the lowest (0mg daily) and highest dose (200-300 mg daily) (Figure 3). While the sodium level trended to decrease with higher spironolactone, it was not statistically significant.
Figure 3.
One reason that potassium levels did not increase is a
difference in study populations. The original population studied for
spironolactone involved patients with heart failure and hypertension whereas
our study’s population was mostly in their 20’s and 30’s with very few
co-morbid conditions.
Although sodium levels are decreased, they did not fall
below the lower limit of normal (135 mmol/L). Low sodium would put transgender
women at risk of dizziness and syncope (passing out) from low blood pressure.
Thus, the takeaway is: sodium should be clinically monitored as it can decrease
in transgender women.
References
Clark E. Spironolactone Therapy and
Gynecomastia. JAMA. 1965;193(2):163-164.
Roberts
TK et al. Interpreting Laboratory
Results in Transgender Patients on Hormone Therapy. The American Journal of Medicine. 2014; 127(2): 159-162.
Hembree WC, Cohen-Kettenis PT,
Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. Endocrine Treatment of
Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical
Practice Guideline. J Clin Endocrinol
Metab. 2017
SoRelle
JA, Jiao R, Gao E et al. Impact of Hormone Therapy on Laboratory Values in
Transgender Patients. Clin Chem.
2019; 65(1): 170-179.
-Jeff SoRelle, MD is a Molecular Genetic Pathology fellow at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and advancing quality in molecular diagnostics.
Anti-nuclear
antibody (ANA) test is commonly used to screen for systemic rheumatic disease. Indirect
immunofluorescence assay using HEp-2 cells as substrate, containing
approximately 100-150 autoantigens, is still the gold standard for ANA testing
(1). Although the test name refers to only anti-nuclear antibody, there are
often cytoplasmic staining patterns overserved in this assay. Cytoplasmic
patterns result from antibodies against cytoplasmic components, like Jo-1 or
Ribosomal P, and have clinical association with various systemic autoimmune
disease, like polymyositis, systemic lupus erythematosus or primary biliary
cirrhosis.
There is no
standardized recommendation regarding how to report cytoplasmic pattern on ANA
IFA, and laboratories independently decides whether to indicate cytoplasmic
pattern in their result. The
International Consensus on ANA Patterns (ICAP) workshop discussed this topic in
2015 and proposed two approaches for reporting ANA cytoplasmic patterns (2).
Either to regard cytoplasmic pattern as positive or negative, both approaches
recommended to include a statement of cytoplasmic staining.
We
encountered cases in our laboratory in which reporting cytoplasmic staining had
significant clinical values, and our laboratory started to report cytoplasmic
staining as an additional comment in the test result a few years ago. Here is
one of these cases:
Case: 35 year old woman with a
history of hypertension complained about increasing muscle pain, weakness, and
swelling. She had difficulties to raise her arms and had multiple falls, and
was admitted to hospital three time for rhabdomyolysis. Her initial laboratory assessment
were, CK >11,196 U/L, lactic acid 2.5 mmol/L, ALT 152 U/L, AST 416 U/L, and ALKP
42 U/L. Her ANA IFA test didn’t shown any nuclear staining, but there is very
strong cytoplasmic staining observed. The clinician was suspecting inflammatory
myositis and ordered myositis autoantibody panel to follow up. This panel detects
numerous antibodies that are either specific or associated with inflammatory
mycosis.
Her myositis autoantibody test result
was positive for antibodies against signal recognition particle (SRP). SRP is
an abundant, cytosolic, universally conserved ribonucleoprotein that targets
specific proteins to the endoplasmic reticulum in eukaryotes and the plasma
membrane in prokaryotes. Antibodies against SRP have been found in 5-8% of
adult idiopathic inflammatory myopathies and <1% juvenile myopathies. It is
closely associated with necrotizing myositis. Clinically it presents with acute
onset, rapidly progressive, severe weakness, with high CK levels and commonly
has cardiac and lung involvement.
Clinically
significant antibodies can be present in patients with connective tissue
disease that may appear as strong cytoplasmic staining on screening ANA test.
It would be helpful to add a comment in these cases to aid the clinician in
pursuing further work-up with a strong clinical suspicious of connective tissue
disease.
References:
1. Position Statement: Methodology of
Testing for Antinuclear. Antibodies American College of Rheumatology. 2009.
2. Damoiseaux
J, et al. International consensus on ANA patterns (ICAP): the bumpy road
towards a consensus on reporting ANA results. Auto
Immun Highlights. 2016 Dec;7(1):1. doi: 10.1007/s13317-016-0075-0. Epub
2016 Jan 30.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist,
currently serving as the Co-director of Clinical Chemistry at Houston
Methodist Hospital in Houston, TX and an Assistant Professor of Clinical
Pathology and Laboratory Medicine at Weill Cornell Medical College.
A 50 year old female was admitted for acute renal failure on CKD stage IV, present with gross hematuria, anemia (due to blood loss) and hypertension. The patient has a significant history of unresolved cryoglobulinemic vasculitis initially diagnosed in 2016 and has been treated by several rounds of rituximab. Other medical histories include Sjogren’s syndrome, MGUS with monoclonal IgM Kappa, coagulopathy (protein S deficiency, on anticoagulant), hyperviscosity, myalgia, deep vein thrombosis, leg edema with superficial ulcer, pulmonary embolus and membranoproliferative glomerulonephritis (MPGN). Kidney biopsy revealed intraglomerular hyaline thrombi consistent with cryoglobulinemic glomerulopathy, interstitial fibrosis tubular atrophy, arterial sclerosis, suggestive thrombotic microangiopathy. Immunohistochemistry was positive for C3, IgM, Kappa, Lambda and CD68. Bone marrow biopsy shown dyserythropoesis without malignancy. Blood testing shown negative hepatitis panel and undetectable C4.
We observed unusual cryoprecipitate test results from this patient: gelatinous appearance precipitate which accounts for more than 40% of volume was observed in both plasma and serum and cannot be cleared at 37C° after several hours of incubation. Further testing shown incubation at 56°C for 30min cleared up the serum but not the plasma. After checking the test history, we found that there was a similar situation for the patient’s cryoprecipitate test a few months back earlier in 2018, and was reported negative for cryoglobulins due to the heat-insoluble nature of the precipitate. Patient was transfused for anemia. No plasmapheresis was done. Due to the patient’s incomplete response to rituximab, Cytoxan was also added to help improve the symptoms.
Cryoprecipitate
Definition: Cryoprecipitates (or cryoproteins) are blood proteins that form precipitates or gels at temperatures lower than 37°C and typically re-dissolve after warming up to 37°C. There are two types:
Cryoglobulin (CG): precipitate from both serum and plasma; either immunoglobulins or a mixture of immunoglobulins and complement components
Cryofibrinogen (CF): precipitate from plasma only; typically composed of a mixture of fibrinogen, fibrin, fibronectin, and fibrin split products
Lab Testing done in our hospital:
Blood are collected in two pre-warmed tubes (one serum, one EDTA plasma) and kept in warm water (37°C) until the serum tube clots.
The plasma and serum are extracted at room temperature, and then stored in refrigerator for 72 hours.
If cryoprotein is present, a precipitate or gel will be seen. An aliquot of the serum is rewarmed at 37°C to verify the cryo-nature.
The precipitate as a percentage of the original serum volume is measured in an ESR tube to determine the cryocrit.
Immunofixation is ordered per pathologist to identify the immunoglobulin compositions of the cryoglobulin.
Cryoglobulinemia
Classification
Strictly speaking, cryoglobulinemia refers to the presence of cryoglobulin (CG) in a patient’s serum, which could be either asymptomatic or present with apparent clinic syndromes (i.e. cryoglobulinemic vasculitis). Cryoglobulinemia can be classified into three types (see table below [1]), with mixed cryoglobulinemia (type II and type III) representing 80% of the cases.
Clinical Manifestations
Type I cryoglobulinemia is frequently asymptomatic, while mixed cryoglobulinemia manifests clinically by a classical triad of purpura, weakness and arthralgias, as well as some other conditions including MPGN, chronic hepatitis, peripheral neuropathy, lymphoma, Raynaud’s, Sjogren’s syndrome, etc.
The presence of heat-insoluble cryoglobulins is rare, and its pathogenesis is poorly understood. On the other side, it may indicate sever clinical consequence as seen in our case and some others as mentioned above.
Essential type II cryoglobulinemia with cryoglobulin-occlusive MPGN and MGUS (Clin Chim Acta. 2009 Aug;406(1-2):170-3):79 y.o. female admitted due to edema and renal failure, cryoglobulin re-dissolved at 56°C, composed of monoclonal IgG-Kappa and polyclonal IgM.
HCV associated thrombotic microangiopathy and cryoglobulin-occlusive MPGN (Am J Med Sci. 2013 Oct;346(4):345-8):57 y.o. female, cryoglobulin re-dissolved at 47°C, composed of monoclonal IgM-Kappa and polyclonal IgG. Symptoms only partially resolved upon treatment of plasmapheresis, corticosteroids and antiviral therapy of peginterferon plus ribavirin.
Essential type I cryoglobulinemia with massive cryoglobulin-occlusive glomerulonephritis (Am J Kidney Dis. 1995 Oct;26(4):654-7):54 y.o. male progressed to ESRD prior to the detection of cryoglobulin. Cryoglobulin with white gelatinous appearance re-dissolved at 54°C, composed of monoclonal IgG-Kappa.
Primary Sjogren’s syndrome with type II cryoglobulinemia and mesangiocapillary glomerulonephritis (Nephrol Dial Transplant. 2000 Jun;15(6):917-8):82 y.o. patient with IgM-MGUS, negative BM, deposition of IgG, IgM and C3 on kidney biopsy, decreased complement levels, negative HCVAb, HBsAb, HBsAg. cryoglobulin re-dissolved at 47°C, composed of monoclonal IgM-Kappa and polyclonal IgG-Kappa.
-Rongrong Huang, PhD is a first year clinical chemistry fellow at Houston Methodist Hospital. Her interests include general clinical chemistry, genetic biochemistry and applications of mass spectrometry in clinical laboratories.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist, currently serving as the Co-director of Clinical Chemistry at Houston Methodist Hospital in Houston, TX and an Assistant Professor of Clinical Pathology and Laboratory Medicine at Weill Cornell Medical College.
We recently received a venous blood sample for blood gas analysis from the operation room. We analyzed the specimen according to manufacturer’s instructions on the ABL800 FLEX blood gas instrument (Radiometer, Copenhagen, Denmark). Multiple error codes were present for the results of ctHb, sO2, FO2Hb, FCOHb, FHHb, and FMetHb. Text messages accompanying the report read, “Detection of SHb” and “OXI spectrum mismatch.” The sample was re-tested on the ABL800 but the same error codes were flagged.
A closer look at the patient’s chart revealed that patient is heterozygous for hemoglobin M-Saskatoon variant, which causes the replacement of histidine by tyrosine in position 63 on the beta chain of hemoglobin (beta codon 63, CAT>TAT/His63Tyr). This renders the NADH methemoglobin reductase system incapable of reducing oxidized iron. A group of mutations in the globin chain gene can result in such dysfunction of ferric iron reduction and are referred to as methemoglobin forming hemoglobin variants (Hgb M).
HbM variants usually have a different absorbance spectrum from the physiologic methemoglobin. Modern day CO-oximeters use more than 100 wavelengths and can detect most unknown substances. We speculated that Hgb M in the patient is the reason the ABL800 reported error codes. The clinical team collected another venous blood sample and it was tested on the GEM5000 blood gas instrument (Instrumentation Laboratory, Bedford, MA, USA). This specimen also reported with error codes.
Non-invasive pulse-oximetry devices use two wavelengths (660 nm and 940 nm) to calculate hemoglobin oxygen saturation based on oxyhemoglobin and deoxygenated hemoglobin, and thus are unable to report interferences from dyshemoglobins. In a nut shell, Hgb M variants can possibly interfere with CO-oximetry measurements. Caution is needed to interpret the results. Pulse oximetry usage should be avoided for these patients.
References
Schiemsky T, Penders J, Kieffer D. Failing blood gas measurement due to methemoglobin forming hemoglobin variants: acase report and review of the literature. Acta Clin Belg. 2016 Jun;71(3):167-70.
Stucke AG, Riess ML, Connolly LA. Hemoglobin M (Milwaukee) Affects Arterial Oxygen Saturation and Makes Pulse Oximetry Unreliable. Anesthesiology 4 2006, Vol.104, 887-888.
-Jayson Pagaduan, PhD, is a senior year clinical chemistry fellow Texas Children’s Hospital in Houston, TX.
-Jing Cao, PhD, DABCC, FACB, is a board-certified clinical chemist, serving as the Associate director of Clinical Chemistry at Texas Children’s Hospital in Houston, TX and an Assistant Professor of Pathology and Immunology at Baylor College of Medicine.
Many clinical laboratorians received questions in the past few months from clinicians about biotin interference on laboratory tests. Although biotin interference is not something new to most clinical chemists, it became more of a concern for clinicians since FDA released a safety communication warning to the public and healthcare professionals that “Biotin May Interfere with Lab Tests” in Nov 2017.
Why does biotin interfere with some laboratory tests?
Immunoassays employed in clinical laboratories often use biotin-streptavidin linkage to separate bound antibody-antigen complex from unbound components. For example, in a sandwich immunoassay setting, analytes bind to signal antibodies and biotinylated capture antibodies, which are immobilized on streptavidin-coated solid phase via biotin-streptavidin binding. In the excess of exogenous biotin, it interferes the binding of biotinylated antibodies and streptavidin, causing erroneous results.
Owing to assay design, tests that utilize the biotin–streptavidin linkage have different tolerance on biotin interference. There has been recent publications that summarized the tolerance level of biotin on commonly used immunoassays from different manufacturer platforms (1, 2). The recommended daily intake (RDI, 30 µg/day) of biotin do not typically interferes with laboratory testing. However, many over-the-counter dietary supplements may contain biotin much higher than the RDI, and the level used for treatment of multiple sclerosis or some other diseases can be even higher. These levels of biotin can cause either falsely high or falsely low test results.
As high-dose biotin use has been increased among general population for nutraceutical purposes, it requires clinicians’ awareness of biotin interference and communication with laboratories to identify incorrect laboratory results. It may require patients to discontinue dietary supplements containing high dose biotin for a period of time before blood drawn to minimize potential biotin interference with testing.
References
Li D, Radulescu A, Shrestha R, Root M, Karger A, Killeen A, et al. Association of Biotin Ingestion With Performance of Hormone and Nonhormone Assays in Healthy Adults. Jama. 2017;318:1150–1160.
Colon P, Greene D. Biotin Interference in Clinical Immunoassays. J Appl Laboratory Medicine Aacc Publ. 2018;2:941–951.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist, currently serving as the Co-director of Clinical Chemistry at Houston Methodist Hospital in Houston, TX and an Assistant Professor of Clinical Pathology and Laboratory Medicine at Weill Cornell Medical College.
Hi everyone! Back with another piece about the life between the lab and medical school. This time, I’d like to take a minute to talk about some new and exciting developments in laboratory diagnostics happening right now: immunoassays for critical troponins are undergoing an evolution. Fourth generation testing is slowly developing into its fifth-generation upgrade. Labs across the country are starting to discuss the relatively new FDA approved fifth-gen cardiac troponin T assay which has been shown to be a high-sensitivity test. But what does this mean for labs? Specifically, what does it mean between the bench and the bedside? The hospital I’m currently on service at is rolling out the first beta-test of this assay in New York City right now, and as it turns out—it’s going to change a lot. Not only will the new understanding of cardiac enzyme reference ranges need a complete overhaul but tailoring appropriate clinical responses to those values will need to be looked at as well. I’m not a sales rep and this isn’t going to be an adventure in comparative statistical analytics, but I think it’s a great time to have a conversation early on about what these new generation assays could mean for us in the lab.
A Whole New World
When I was in graduate school, doing my MLS training we were taught the same cardiac enzyme assay history that was developed over the last 50 or so years. Early acute markers of inflammation relating to acute myocardial infarctions (AMIs) with respect to acute phase reactants AST, LDH, CRP, etc. As more technology advanced, specific biomarker analyses of individual detection of things like CK or myoglobin became useful. The WHO criteria for AMI then established (and re-established since the 1970s) the laboratory requirements for CK-MB and detectable levels of troponin to correlate with clinical findings. Further sensitivity and specificity developments, and clinical research like the GUSTO and APACE trials, showed us just how sensitive newer (then troponin T and I) cardiac assays could be. Not to mention, instead of rule-in/rule-out criteria, we had the development of risk stratification. And as instrumentation developed so did our testing—CK and LDH replaced with CK-MB and its isoforms, AST went the way of Myoglobin, and LD ratios became reliable troponins!
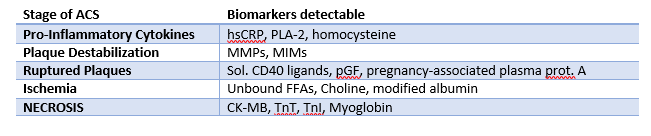
Table 1. In each stage of acute coronary syndrome (ACS) various biomarkers are available and detectable in peripheral blood. The challenge has been to find the most reliable and time-sensitive cardiac enzyme(s) to reflect appropriate staging and risk stratification. Research is helpful, but clinical intervention required critical timing.
Ask most clinicians today about cardiac enzyme, cardiac injury studies, or other related markers and you’ll hear about CPK, CK-MB 1, 2, 3 and other isoenzymes, LDH electrophoresis, and of course troponins T and I. What’s more is that the reference ranges for most of these tests haven’t really changed much either. If I called you and said your patient in 706-W has a Troponin of <0.03 you might be relieved for now. If I said that same patient’s troponin was 0.560—we might have a different story unfold. But what if I told you your patient’s troponin was 13, and was trending down from 15? What do you do with that? What if I only called to report a troponin-DELTA which was 0.0? Was there an in-service you missed? Possibly. Sounds like your institution might have 5th-gen on board.
What was wrong with the old troponin?
In a word: nothing, really. This really isn’t about buy-in for a “better” test or a better detection method. This is about creating a dialogue about improving risk stratification for our patients with coronary disease. Let’s go back to Chicago, specifically the last hospital I worked in before starting medical school: Swedish Covenant Hospital. Having been through a few hospitals in my time, I can say you’d be hard pressed to find a more streamlined, albeit small community hospital, laboratory service. Running a full gamut of SIEMENS instrumentation and critical middleware-software, the management there ran a tight ship—which included critical troponins. We ran the TnI-Ultra assay on the ADVIA Centaur/XP platform. It was your standard three-part immunoassay sandwich test with a biotin-streptavidin antigen-antibody detection. It was fast, used little reagents, was relatively stable, had a great system of QC, and was calculably-flexible between heparinized and ETDA plasma samples. Two-point calibration kept it tight between (and this is from memory, loosely) 0.006 and 0.50 ng/mL, and I believe we called our critical values at 0.40 ng/mL. This was a good test, and it’s used in many labs today still. It’s got great stability and has room to interpret ACS risk stratification based on population data in each location. People understand those results, too. But exactly how much room between, let’s say 0.10 ng/mL and >0.50 ng/mL, is there to stratify that risk? Complex decision algorithms then become hybrids of institutional cardiology recommendations, American College of Cardiology (ACC) recommendations, emergency department input, and, of course, laboratory management recommendations.
Here at Bronx Care Hospital Center (BCHC), I spoke with a laboratory manager about rolling out this brand new high-sensivity troponin (hs-cTn), and we discussed their vaildation and policies. Along with this new project, the hospital has been a vocal part of American College of Cardiology ACC17 Acute and Stable Ischemic Heart Disease program addressing topics including marijuana use and ACS, stable angina risk stratification, NSTEMI sex differences in revascularization and outcomes, treating cocaine related ACS with beta blockers, and research Anticoagulation Therapy After Anterior Wall ST-Elevation Myocardial Infraction in Preventing LV Thrombi. So, it seems fitting that this is as good as any a pilot location for cardiology departments city-wide to watch and learn from the hs-cTn roll-out!
Tell me more about this new test…
This hs-cTn assay is an electrochemiluminescence immunoassay (ECLIA) that uses two monoclonal antibodies against human cardiac troponin T. At this institution, they are using this immune sandwich assay on a Roche Cobas E with a similar biotin-streptavidin coated microparticle complex as with the previous generation testing. This is a short test with similar reagent use and stability as before, and only for lithium heparinized samples. With a relatively quick turn-around in less than 10 minutes, the new hs-cTn offers critical information for clinical correlations on the fly from potential STEMI codes coming into the ED.
Without going into horrific details about validating data on old and new troponins across patient populations, there is something interesting to note here which came up in discussion with the lab manager: new reference ranges. Now, with testing sensitivity, cross-reactivity, ranges, and interfering substances, the ranges are no longer the decimal-place values reported that we’re all used to. The ranges we work with now at BCHC are cutoff between <12 ng/L for positives and >52 ng/L for critical values suggestive of acute coronary syndrome. The analytical measuring range is much larger now between 6-10,000 ng/L. With the adjustments for limits of detection and blanks on instrumentation, the specificities of these values are normalized on a larger index for reflecting differences in male and female cardiac enzyme activity to a common cutoff of that <12 ng/L value. But more so than just a value, a new part of trending troponins becomes much more important: the delta values. These are more acutely indicative of the cardiac necrosis and/or condition of other non-specific heart tissue damage en vivo occurring in patients. Taking all this into account, you now have a much wider and broader range of values to interpret and incorporate into your clinical decision making, which brought up a few questions when I spoke with lab staff as well as cardiologists.
So, what’s wrong with the new troponin?
Okay, that’s a fair question at this point. And my answer is still: probably nothing. Sorry to be so inconclusive, but it’s still early days. There is a lot of data to support moving toward newer generation hs-cTn testing since it has been available outside of FDA-approval in Europe before January 2017. Research done in the Department of Internal Medicine and Central Institute for Medical Laboratory Diagnostics at Innsbruck Medical University in Austria show that new troponins might not be that different (read: better) than their 4th generation counterparts, at least with regard to emergency room visits. T. Ploner, et. al, argue that diagnosing AMI in the ED doesn’t really benefit from the heightened sensitivity offered by the new Roche 5th gen assay (Figure 1, Figure 1). But, when they compared the detection of other cardiac disease including AMI, unstable angina, heart failure, arrythmias, pulmonary emboli, pulmonary disease, anemia, renal disease, and several other entities, the 5th generation assay could more readily detect changes early and provide clinicians with critical data quickly (Figure 1, Figure 2).
Figure 1. Ploner et al. demonstrate here that there isn’t really any difference in the sensitivity of 4th generation vs. 5th generation troponins for detecting acute MI in the emergency room. However, there is a significant advantage in the detection of any cardiac disease, generally. (Source: Ploner et al. (2017) High-Sensitivity cardiac tropnonin assay is not superior to its previous 4th cTnT assay generation for the diagnosis of acute MI in a real-world emergency department, link: http://spo.escardio.org/eslides/view.aspx?eevtid=48&fp=P4177)
Finally, I think a review paper from the American Journal of Medicine last year summarized it best. Coming from the Department of Cardiovascular Diseases and Department of Laboratory Medicine and Pathology at Mayo Clinic in Rochester, MN, the authors discussed concern over the troubling over-sensitivity and potential pitfalls of reaching too far with hs-cTn testing. Their bottom line: collaborating on data and accuracy between cardiology, laboratory medicine, and emergency medicine, there is a great potential for this super sensitive test to provide clinicians with very useful data in the near future. We just have to process that data correctly. As always, results should be interpreted in conjunction with clinical presentation including medical history and laboratory data. But in the case of new and coming advances in critical care, there seem to be some common themes between my conversations here at BCHC and in what I read in the literature regarding how to ensure we move forward appropriately.
Multidisciplinary educational efforts are critical. The ER, the lab, and the cardiology department at each institution utilizing 5th gen troponins need to understand the new ranges, the new triaging cutoffs, the clinical correlations for consulting the ICU/CCU, and how to understand the deltas for their patient populations.
Create clear communications for your laboratory values. Will you normalize for gender or provide sex-specific confidence interval reporting? Will you provide tables for suggested value correlations with AMI/ACS protocols?
Order sets and in-service training. You’d be surprised how much the nitty gritty details of lab draws and ordering appropriate tests/tubes could slow down your institution’s advancement.
Figure 2. How the authors at Mayo Clinic establish the use of new hs-cTn assays in diagnosing and triaging potential AMI patients. (Source: Sandoval, Jaffe (2017) Using High-Sensitivity Cardiac Troponin T for Acute Cardiac Care, The American Journal of Medicine (2017) 130, 1358–1365, doi:10.1016/j.amjmed.2017.07.033)
At the very end of the day, it’s up to the institution. Clinical centers have to follow their own guidelines for cardiac pathology. ACC/ESC/AHA guidelines and Universal MI definitions are for clinical correlation across locations, but a single roll-out of a fancy new test can’t make a better ER. It really does take communication, collaboration, and accountability. We all have to push the envelope and practice at the top of our scopes in order to make health care better every day. One of the ways we might be able to do that now is by considering these new high-sensitivity troponins as a useful new clinical tool to improve patient outcomes.
Thanks for reading! See you next time!
Disclosure: I am no longer affiliated with Swedish Covenant Hospital in Chicago as an employee, and any recount of policy and/or procedure(s) specifically regarding their cardiology protocols and troponin resulting are a historical and anecdotal account of my time working there in the past. I have no affiliations with SIEMENS, Advia, Roche, or any other medical laboratory instrumentation institution. I am only affiliated with Bronx Care Hospital System as a current rotating medical student and my account of their transition to 5th gen testing is anecdotal from discussions with in-house staff, cardiologists, and laboratory management.
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.
Our patient is a 47-year-old female with a history of type II diabetes mellitus, hypertension, pancreatic insufficiency, systemic sarcoidosis with lung and liver involvement. She was admitted into the ED for severe hypercalcemia, hypokalemia and hypomagnesemia. Her total calcium concentration was at 15.1 mg/dL (ref range: 8.3-10.2 mg/dL, critical: >13.0) at admission and albumin was low. Further testing revealed 25-hydroxy vitamin D (25(OH)D) of 23.2 ng/mL, which is considered insufficient, and decreased PTH of < 15 pg/mL (ref range: 15 – 65). From these results, primary hyperparathyroidism was ruled out. PTH related peptide (PTHrp) was tested given her sarcoidosis history.
PTHrp is produced by some cancers, especially kidney, breast and lung cancers, and as well as lymphoma and leukemia. It has the same N-terminal and binds to the same receptor as PTH, therefore sharing some functions of PTH. In patients with hypercalcemia associated with malignancy, PTHrP may be evaluated. There are also case reported sarcoidosis-related hypercalcemia due to production of PTHrp. In the case, PTHrp was normal at 0.4 pmol/L (ref range: < 2.0).
Further tests showed that 1, 25-dihydroxyvitamin D (DHVD) was elevated at a concentration of 93.3 pg/mL (ref: 18.0 – 78.0). In the presence of decreased 25(OH)D, this result suggested that the 1-alpha-hydroxylase could be the cause of hypercalcemia. DHVD is the active form of vitamin D. It promotes intestinal calcium absorption and, in concert with PTH, skeletal calcium deposition. 25(OH)D converts to DHVD via 1-alpha-hydroxylase, which is almost exclusively expressed in the kidney, but can also be found in some extrarenal tissues, including inflammatory cells of the monocyte/macrophage lineage commonly seen in sarcoidosis and other granulomatous diseases. DHVD produced in extrarenal tissues is PTH-independent, and moreover, elevated calcium induced by extrarenal DHVD can inhibit PTH production via calcium-sensing receptor (CaSR) on parathyroid cells.
Sarcoidosis is a multisystem inflammatory disease of unknown etiology manifests as granulomas found predominantly in the lungs and lymph nodes. Hypercalcemia is seen in about 10-13% of patients. Overproduction of 1-alpha-hydroxylase and production of PTHrp can both contribute to the hypercalcemia in some patients with sarcoidosis. In this case, PTHrp was normal and elevated 1-alpha-hydroxylase was found to be the cause of hypercalcemia.
In addition to treatment of the underlying disorder, treatment of hypercalcemia in sarcoidosis is aimed at reducing intestinal calcium absorption and DHVD synthesis. Besides dietary interventions, glucocorticoids and bisphosphonates have also been used successfully to treat hypercalcemia in sarcoidosis:
Glucocorticoids: inhibit DHVD synthesis by the activated mononuclear cells (major contribution), inhibit intestinal calcium absorption and osteoclast activity
Bisphosphonates: inhibit the resorption of bone by osteoclasts
-Rongrong Huang, PhD is a first year clinical chemistry fellow at Houston Methodist Hospital. Her interests include general clinical chemistry, genetic biochemistry and applications of mass spectrometry in clinical laboratories.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist, currently serving as the Co-director of Clinical Chemistry at Houston Methodist Hospital in Houston, TX and an Assistant Professor of Clinical Pathology and Laboratory Medicine at Weill Cornell Medical College.
Patient was a 1-week-old infant in the level 2 NICU born at 37 weeks. This infant was initially born with indirect hyperbilirubinemia but now also has increasingly elevated level of direct bilirubin (see measurements in table below). Neonatologist requested conjugated and unconjugated bilirubin test due to increasing elevated level of direct bilirubin. Conjugated bilirubin test is not routinely performed in our hospital laboratory and needs to be send out.
Question: What’s the difference between conjugated bilirubin and direct bilirubin? When does conjugated bilirubin need to be assessed?
Ref Range
3/6/18
3/7/18
3/9/18
3/10/18
3/12/18
Bilirubin total, neonatal
1.0-10.5 mg/dL
9.2
8.7
10.8
10.2
8.6
Bilirubin direct, neonatal
0.0 – 0.6 mg/dL
0.5
0.7
1.8
1.8
2.1
Discussion
Neonatal jaundice is commonly seen in newborns in the first few days of life, mainly due to increased bilirubin formation from break down of red blood cells and limited conjugation of bilirubin. Total bilirubin normally peaks at day 2-3 and should decline by day 4-5. Sample is collected via heelstick in green top tube and protected from light. Measurement of total bilirubin is interpreted based on the Bhutani Nomogram to assess risk of hyperbilirubinemia. Most often, unconjugated bilirubin is elevated in neonatal jaundice owing to hemolytic causes. In cases with prolonged jaundice, conjugated bilirubin needs to be determined to rule out cholestasis.
Conjugated bilirubin refers to bilirubin conjugated with one or two glucuronic acid, and this term “conjugated bilirubin” is often used interchangeably with direct bilirubin. Direct bilirubin refers to bilirubin fractions that can directly react with diazo reagent without the addition of accelerator, such as methanol or ethanol. This fraction usually includes conjugated bilirubin and delta bilirubin. Delta bilirubin is formed by covalent bonding between conjugated bilirubin and albumin, and has a similar half-life as albumin, 21 days. Therefore, direct bilirubin measurement overestimate conjugated bilirubin and in cases with persist or atypical jaundice, clear differentiation between conjugated and direct bilirubin is important. Clinician should know what the laboratory is measuring when interpreting the bilirubin fraction results.
In laboratories, conjugated bilirubin can be assessed by the VITROS BuBc dry slide, which simultaneously measures unconjugated (Bu) and conjugated (Bc) bilirubin by use of a mordant. In the presence of the mordant, the visible spectra of conjugated and unconjugated bilirubin are different, allowing measurement of both species from a single slide. Fractions of bilirubin can also be separated by HPLC, but this is not practical to use in a routine clinical laboratory. In this case, conjugated bilirubin was measured by VITROS BuBc slide test, and result came back elevated at 1.0 mg/dL (ref range: < 0.3 mg/dL).
-Megan Ketcham, MD is a 4th year anatomic and clinical pathology resident at Houston Methodist Hospital. She will be completing both hematopathology and dermatopathology fellowships. Her interests include pathology resident and medical student education and skin lymphomas.
-Xin Yi, PhD, DABCC, FACB, is a board-certified clinical chemist, currently serving as the Co-director of Clinical Chemistry at Houston Methodist Hospital in Houston, TX and an Assistant Professor of Clinical Pathology and Laboratory Medicine at Weill Cornell Medical College.