Clinical History
An African American male in his early 20s presented to the emergency department (ED) with complaints of a sore throat, headache, generalized body aches, and fatigue for the past week. He also noted intermittent fever and chills as well as some nausea with a decrease in his appetite. He had been seen multiple times in the ED recently for similar symptoms. His past medical history was non-contributory and he noted no significant travel or exposure history with the exception of attending a local party 10 days ago. His temperature was 100.5°F and vitals were otherwise normal. His physical exam was normal with the exception of dry mucous membranes indicating mild dehydration. Initial laboratory testing showed a leukopenia (white blood cell count of 1.5 TH/cm2) with 39% lymphocytes and rapid antigen testing for group A Streptococcus, influenza, and infectious mononucleosis were negative. The patient was admitted for further work up due to the prolonged nature of his symptoms.
Laboratory Identification
Results from additional infectious disease testing are in the table below.
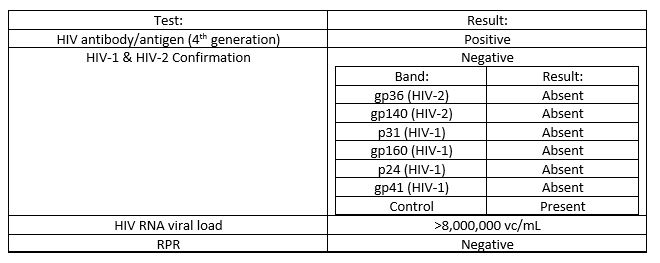
This pattern of results is most consistent an acute HIV infection.
Discussion
Human immunodeficiency virus (HIV) is an enveloped, single stranded RNA virus which belongs to the family Retroviridae. HIV is most commonly sexually transmitted via body fluids such as blood, semen, and vaginal secretions directly contacting mucosa membranes. HIV can also be transmitted due to needle stick injuries, blood transfusions, and transplacentally from infected mother to fetus or by breast feeding. Acute HIV illness presents as a mononucleosis-like syndrome with fever, pharyngitis, arthralgias, malaise, and weight loss. During this acute illness, the HIV RNA viral load is extremely high. After a period of clinical latency, which on average is approximately 10 years, there is a deterioration of the immune system, the CD4 count drops, and the patient is at risk for opportunistic infections and neoplastic diseases.
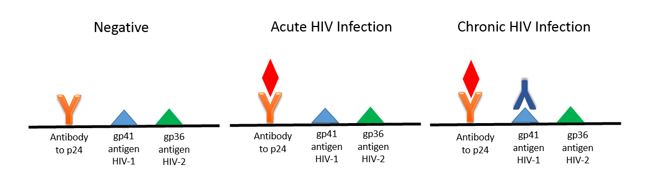
Based on the 2014 CDC/APHL guidelines, the initial screening test for HIV is an antigen-antibody combination assay. These immunoassay based tests detect the p24 antigen and antibodies to HIV-1 and HIV-2 (see image below). By testing for the p24 antigen in addition to HIV antibodies the time to a positive patient result is decreased (window period) as p24 is one of the first viral proteins to appear, even before antibodies are present.
If the antigen-antibody test is repeatedly positive, the second step in the testing algorithm is an antibody differentiation assay. This test has taken the place of the Western blot and Western blot is no longer recommended in the diagnosis of HIV. If the antibody differentiation test is positive, the diagnosis of HIV-1 or HIV-2 is confirmed. As this step only detects the presence of antibodies, the differentiation test will be negative in an acute HIV infection.
If there is a discrepancy between the first two steps in the testing algorithm or an indeterminate result is obtained, the final step involves nucleic acid amplification testing (NAAT) to detect viral RNA. Viral RNA is the first HIV-1 specific marker to appear following infection. In the case of an acute or untreated long term infection, the viral load can approach levels up to 100 million copies.
When additional history was obtained from our patient, he said he was sexually active with a new male partner in the past few weeks and did not use protection. He stated he had been treated with Chlamydia in the past. Further testing for CD4 count, other opportunist & sexually transmitted infections, and HIV genotype testing was performed and outpatient HIV care was arranged for the patient.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement, and resident education.
