29-year-old woman with a history of ITP (immune mediated thrombocytopenia) diagnosed in 2008. She had previously been treated with steroids, IVIG (intravenous immunoglobulin) and splenectomy. She also received Romiplostim for 1 year prior to its discontinuation. She had also been diagnosed with lupus one year previous.
Follow up visit after having her platelets evaluated in the office 2 weeks ago revealed a platelet count of 9 K/uL on CBC which was flagged by the instrument due to platelet clumping.
- WBC: 7.5 K/ul
- HGB: 12.2 g/dl
- HCT: 37.3 %
- PLT: 9 K/ul *
*On manual count the platelet count was deemed to be 74 K/uL.
Peripheral smear review:
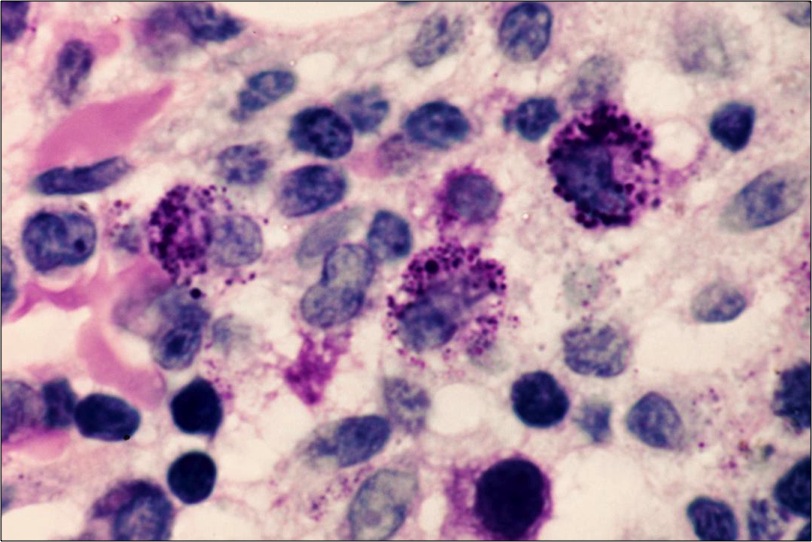
Numerous large and some giant platelets, platelet clumping and basophilic Dohle body like inclusions in nearly all neutrophils.

Characteristic giant platelet with poorly defined granulation. Normal-sized platelet is also present. Neutrophil contains large, well-defined, basophilic, peripherally placed cytoplasmic inclusion body (resembling Döhle body).

The value of peripheral smear review is very well highlighted by this case. As the smear was never reviewed earlier in the disease course, diagnosis of MHA was not made and the patient was diagnosed as ITP entirely based on clinical presentation. Perhaps earlier review of peripheral smear would have significantly altered the clinical management of the case.
After discussion with pathologist who reviewed the peripheral blood smear, diagnosis of May-Hegglin anomaly was confirmed and appropriately documented in the patient’s chart.
May-Hegglin anomaly (MHA):
May-Hegglin anomaly (MHA) is a rare autosomal dominant disorder characterized by various degrees of thrombocytopenia that may be associated with purpura and bleeding; giant platelets containing few granules; and large (2-5 um), well-defined, basophilic, cytoplasmic inclusion bodies in granulocytes that resemble Döhle bodies.
MHA is one of a family of macrothrombocytopenias characterized by mutations in the MYH9 gene present in chromosomal region 22q12-13. The mutation results in disordered production of nonmuscle myosin heavy-chain type IIA, which leads to invariable macrothrombocytopenia secondary to defective megakaryocyte maturation.
Clinical features:
The rarity of MHA has led to conflicting literature regarding the risk for bleeding. Asymptomatic patients have been described however, abnormal bleeding has also been documented. The bleeding risk is increased by taking drugs that decrease platelet function. The risk for excess bleeding with surgical procedures is unclear. Rare reports have described arterial thrombotic events associated with May-Hegglin anomaly, though the risk remains unclear. Patients are often asymptomatic. The bleeding tendency associated with MHA is generally mild and is thought to mainly depend on the degree of thrombocytopenia.
Clinical Features of MYH9 -Related Thrombocytopenias
| Condition | Macrothrombocytopenia | Granulocyte inclusions | Nephritis and Deafness | Cataracts |
| MHA | Yes | Döhlelike | No | No |
| Epstein syndrome | Yes | Absent or faint | Yes | No |
| Fechtner syndrome | Yes | Spherical granules | Yes | Yes |
| Sebastian syndrome | Yes | Spherical granules | No | No |
Differential diagnosis:
In addition to acute immune thrombocytic purpura, the differential diagnosis for thrombocytopenia associated with large platelets (elevated mean platelet volume) includes Bernard-Soulier syndrome, Montreal platelet syndrome, gray-platelet syndrome, and Alport syndrome.
The differential diagnosis for thrombocytopenia due to ineffective thrombopoiesis includes Bernard-Soulier syndrome, Wiskott-Aldrich syndrome, Greaves syndrome, thrombopoietin deficiency, and megaloblastic anemia.
The differential diagnosis for leukocytic inclusions, sometimes called Döhle bodies, includes septicemia, myeloproliferative disorders, and pregnancy.
Laboratory investigation:
- The complete blood count (CBC) is essential in assessing MHA. The platelet count is decreased (usually in the range of 40-80 ´ 109/L), but the degree of thrombocytopenia varies.
- The disorder is also characterized by giant platelets. Platelets are enlarged (>15 µm in diameter), and the mean volume of MHA platelets can be as high as 30 fL. Platelet morphology is otherwise normal.
- On electron microscopy, platelets are seen to contain normal organelles (alpha granules, dense granules, lysosomes, and mitochondria). The most conspicuous ultrastructural feature of the platelets is an increased amount of disorganized microtubules.
- Cytoplasmic inclusion bodies particularly in the neutrophils but also in monocytes, eosinophils, and basophils. The inclusions are large (>5 µm), spindle-shaped, pale, blue-staining bodies that consist of ribosomes, segments of endoplasmic reticulum, and microfilaments. They are located in the periphery of the cytoplasm and resemble Döhle bodies.
- Ultrastructural studies reveal that these bodies consist of clusters of ribosomes oriented along parallel myosin heavy-chain filaments 7–10 nm in diameter. Neutrophil function is considered to be normal, and patients have no increased susceptibility to infections.
- Immunocytochemistry can detect NMMHCIIA complexes within the leukocytes and is a useful confirmatory test.
- The bleeding time is prolonged in concordance with the degree of thrombocytopenia.
- Platelets usually aggregate normally in response to various agonists. The glycoprotein composition of the platelet surface is normal.
Management
Most patients with MHA do not appear to have clinically significant bleeding problems, and specific treatment is not required.
- Corticosteroids and splenectomy are ineffective
- In rare patients with severe bleeding, platelet transfusion may be required
- Bleeding risk is not significantly increased by normal vaginal delivery
- For patients scheduled to undergo surgery, intravenous desmopressin acetate (DDAVP) may be valuable; routine prophylactic platelet transfusions are not usually indicated, but platelets should be kept available
- Depending on circumstances, refraining from participation in contact or collision sports may be prudent.

-Neerja Vajpayee, MD, is an Associate Professor of Pathology at the SUNY Upstate Medical University, Syracuse, NY. She enjoys teaching hematology to residents, fellows and laboratory technologists.