Case History
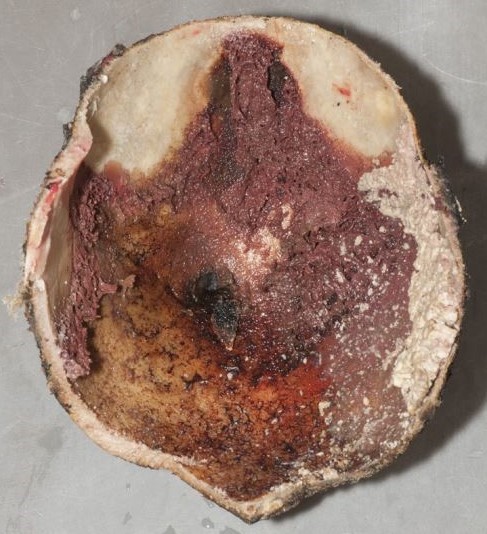
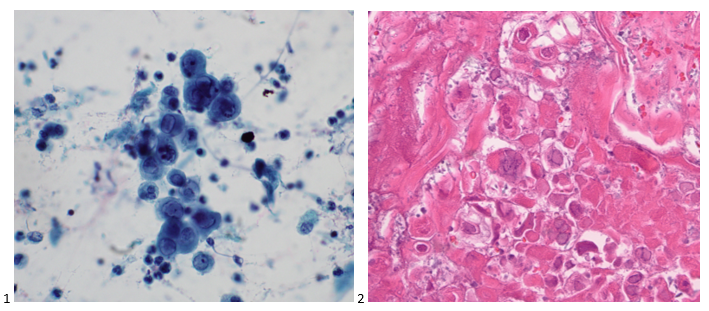
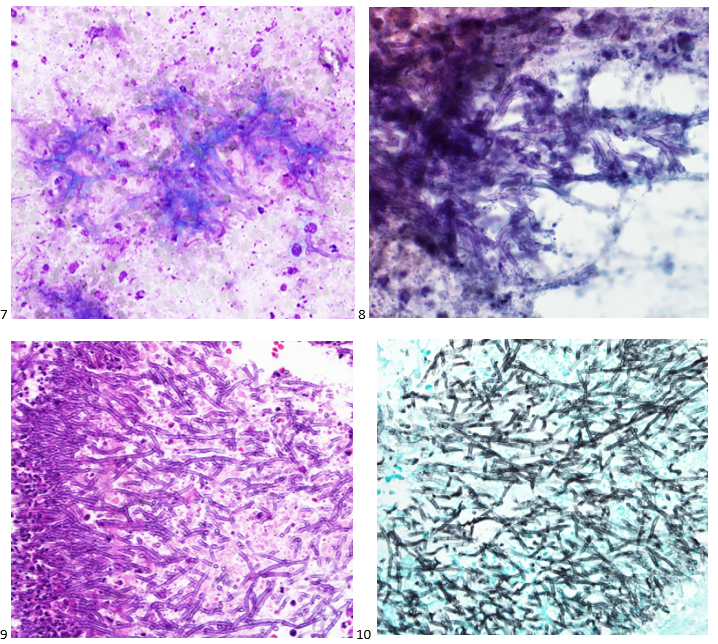
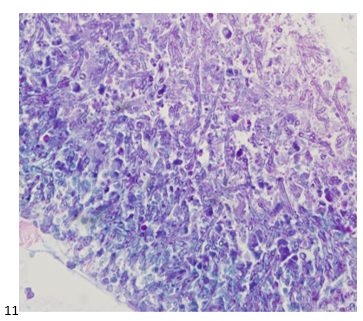
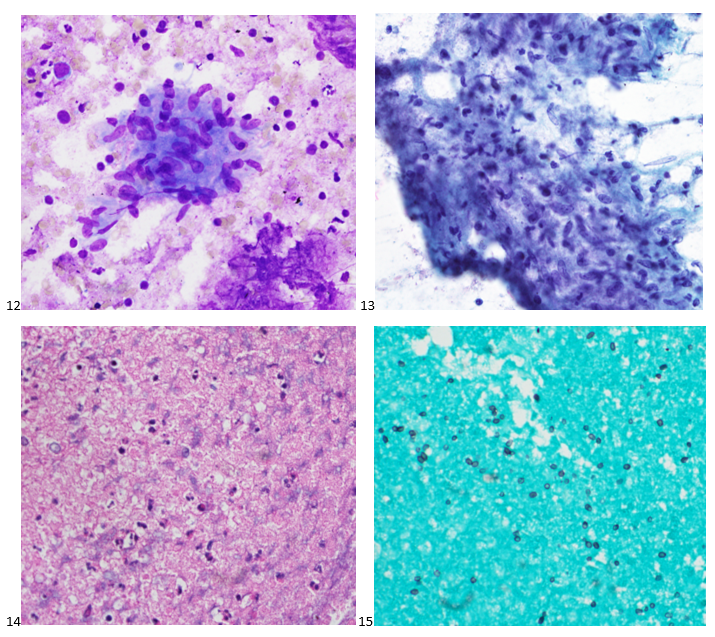
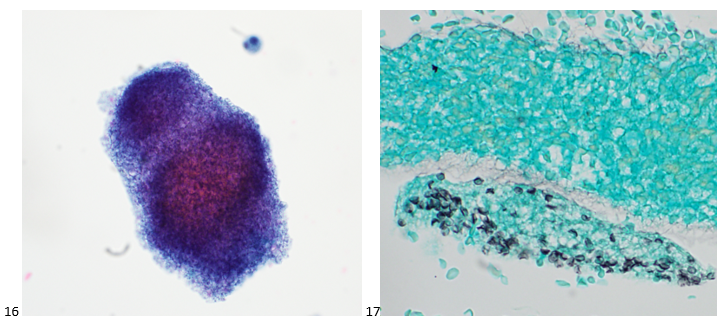
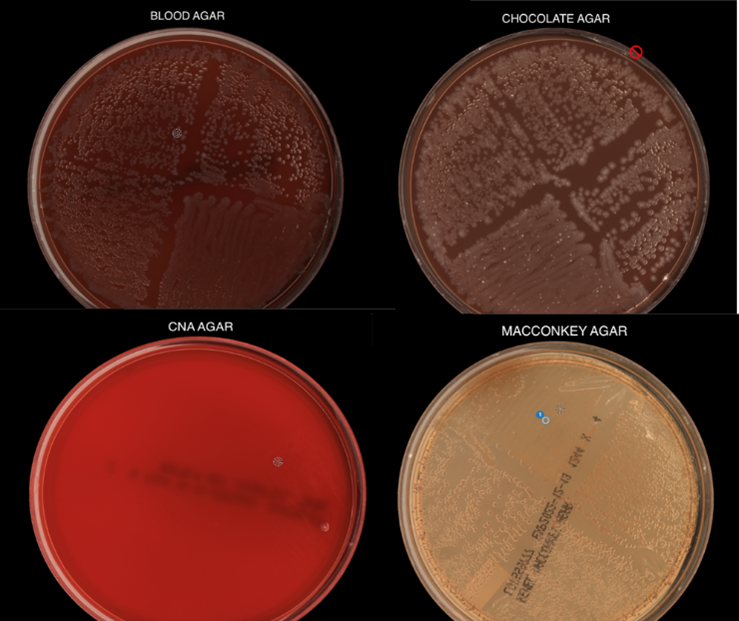
A 40-year-old woman with past medical history of polysubstance use disorder (cocaine, IVDU-heroin) presented with shortness of breath on exertion, weight loss, and weakness. Cardiac ultrasound showed aortic valve endocarditis with mild thickening of the aortic valve, vegetation and severe aortic regurgitation without stenosis. The patient was taken to the operating room for aortic valve replacement. A tissue biopsy was sent for surgical pathology workup and microbiology cultures. H&E staining of the right and left coronary cusp and noncoronary cusp and showed focal giant cell reaction, and acute inflamed granulation tissue consistent with vegetation/infective endocarditis. The Gram stain of the tissue specimen revealed gram positive cocci but no bacterial growth was seen. Fungal and mycobacterial cultures were also negative. Broad Range Bacterial PCR and Sequencing (BRBPS) of the heart valve detected Streptococcus mutans.

Discussion
The first step of BRBPS is performing polymerase chain reaction (PCR) targeting the 16S ribosomal RNA (rRNA), a conserved gene across many bacterial species including mycobacteria. If PCR is negative, then sequencing is not performed but if PCR is positive, sequencing such as Sanger sequencing or Next generation sequencing will be followed. Subsequent bioinformatics analysis of the sequencing results will allow identification of the specific bacteria.1,2 In the patient here, the PCR for 16S rRNA was positive and sequencing revealed S. mutans.
S. mutans is part of the viridans-group of Streptococcus and can be identified as a gram positive cocci with growth that is alpha-hemolytic, optochin resistant, and bile insoluble. Viridans group Streptococcus invade the bloodstream following dental treatment or dental procedures and can be associated with high risk for infectious endocarditis in patients with underlying heart disorders. S. mutans first gained medical attention due to its role in dental caries.3 S. mutans is considered part of the normal flora of the oropharynx, more specifically the dental plaque, and can form biofilms on the hard surface of the tooth. Bacterial strains that cause endocarditis have been shown to be able to bind to type I, III, and IV collagen, which are major components of the host cardiovascular tissues.4 The bacteria also have virulence factors that can cause strong adhesion to human endothelial cells. Additionally, aggregation and interaction with fibrinogen, platelets, and completement allow this bacteria to successfully cause cardiovascular diseases.5
In infective endocarditis, 20% of the cases are negative by conventional methods such microbiology cultures.6 Several studies have shown that in specimens from patients with endocarditis, 16s rRNA sequencing can correctly detect the organism that was grown in culture but also successfully detect organisms in specimens where there was no growth, allowing clinical teams to accurately treat patients, similar to our case here.7,8 For prosthetic heart valve tissue, the sensitivity of sequencing versus culture is 93% and 35%, respectively. A study describing periprosthetic joint infections using elbow joint fluids showed that sequencing was positive in 47 specimens but 8% of those were negative by culture.10 Additionally, 16s rRNA sequencing has been useful in identifying bacterial tick-borne organisms not typically grown in culture such as Borrelia, Anaplasmsa, Ehrlichia, and Rickettsia].11
The BRBPS test is validated for and ideally be tested on specimens from sterile sources (joint fluid, blood, heart valves, CSF) and ideal specimens are those where bacterial organisms can be visualized using microscopy. Limitations of BRBPS is that this test only detects bacterial organisms and will not detect viruses, fungi, and parasites. False-positive results are possible if the specimen is contaminated with patient flora. False-negative results may occur due to sequence variability affecting how the primers bind, presence of PCR inhibitors, or the quantity of nucleic acid material below the limit of detection. Clinical tests utilizing sequencing approaches may be costly at the moment in time; those who order sequencing tests need to understand the purpose of different sequencing tests so the most appropriate test is ordered. For example, if fungal pathogens are suspected, a sequencing test based on amplifying 28S rRNA or ribosomal ITS genes for the conserved genes found in fungal pathogens is appropriate.12 Such tests where you selectively enrich for specific targets such as 16s or ITS are ‘targeted NGS tests’ which have higher sensitivity for detection of microorganisms in sample types with large amounts of DNA. In comparison, metagenomics is a more agnostic approach and allows for detection of all nucleic acid in the specimen (including both host and microbial reads). While metagenomics can successfully detect pathogens involved in an infection, it can also detect the microbiome present in the same specimen. Hence, the one limitation is the background noise from human nucleic acid and the microflora [13-14. Another type of sequencing is whole genome sequencing where the microbial genome of a particular organism is sequenced and assembled. WGS aids in identification, typing, and determining the microbial susceptibility. WGS is helpful in identifying outbreaks or for epidemiological purposes, but the limitation is that a pure culture is needed. WGS requires a pure culture so this is a limitation for organisms that are non-viable in culture [13-14].
References
- Rosey AL, Abachin E, Quesnes G, Cadilhac C, Pejin Z, Glorion C, Berche P, Ferroni A. Development of a broad range 16S rDNA real-time PCR for the diagnosis of septic arthritis in children. J Microbiol Methods. 2007 Jan;68(1):88-93. doi: 10.1016/j.mimet.2006.06.010. Epub 2006 Aug 14. PMID: 16904782.
- Broad Range Bacterial PCR and Sequencing, Varies. Mayo Clinic Laboratories. https://www.mayocliniclabs.com/test-catalog/Overview/65058
- Loesche WJ. 1986. Role of Streptococcus mutans in human dental decay. Microbiol Rev 50:353–380.
- Nomura R, Naka S, Nemoto H, Inagaki S, Taniguchi K, Ooshima T, Nakano K. 2013. Potential involvement of collagen-binding proteins of Streptococcus mutans in infective endocarditis. Oral Dis 19:387–393. doi: 10.1111/odi.12016.
- Otsugu, M., Nomoura R., Matayoshi, S., Teramoto, N., Nakanoa, K. Contribution of Streptococcus mutans Strains with Collagen-Binding Proteins in the Presence of Serum to the Pathogenesis of Infective Endocarditis. Infect Immun. 2017 Dec; 85(12): e00401-17.
- Baddour LM at al; American Heart Association Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and Stroke Council. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals from the American Heart Association. Circulation. 2015 Oct 13;132(15)
- Peeters, B., Herijgers, P., Beuselinck, K., Verhaegen, J., Peetermans, W.E., Herregods, M.-C., Desmet, S., Lagrou, K. Addd diagnostic value and impact on antimicrobial therapy of 16s rRNA PCR and amplicon sequencing on resected heart valves in infective endocarditis: a prospective cohort study. Clinical Microbiology and Infection. 2017 Nov; 23(11): 888.e1-888.e5
- Premru, M.M, Zupanc, T.L., Klokocovnik, T., Sabljic, E.R., Cerar, T. Broad-Range 16s rRNA PCR on Heart Valves in Infective Endocarditis. J Heart Valve Dis. 2016 Mar; 25(2):221-22
- Miller, R. J.H., Chow, B., Pillai, D., Church, D. Development and evaluation of a novel fast broad-range 16S ribosomal DNA PCR and sequencing assay for diagnosis of bacterial infective endocarditis: multi-year experience in a large Canadian healthcare zone and a literature review. BMC Infect Dis. 2016 April 12:16:146
- Flurin, L.; Wolf, M.J.; Greenwood-Quaintance, K.E.; Sanchez-Sotelo, J.; Patel, R. Targeted next generation sequencing for elbow periprosthetic joint infection diagnosis. Diagn. Microbiol. Infect. Dis. 2021, 101, 115448.
- Kingry, L.; Sheldon, S.; Oatman, S.; Pritt, B.; Anacker, M.; Bjork, J.; Neitzel, D.; Strain, A.; Berry, J.; Sloan, L.; et al. Targeted Metagenomics for Clinical Detection and Discovery of Bacterial Tick-Borne Pathogens. J. Clin. Microbiol. 2020, 58, e00147-20.
- Yeo, S.F.; Wong, B. Current status of nonculture methods for diagnosis of invasive fungal infections. Clin. Microbiol. Rev. 2002, 15, 465–484.
- Mitchell SL, Simner PJ. Next-Generation Sequencing in Clinical Microbiology: Are We There Yet? Clin Lab Med. 2019 Sep;39(3):405-418
- Hilt, E.E., Ferrieri, P. Next Generation and Other Sequencing Technologies in Diagnostic Microbiology and Infectious Diseases. Genes (Basel). 2022 Aug 31;13(9):1566. doi: 10.3390/genes13091566.

–Rami Abdulbaki, MD is a Pathology Resident (PGY-4) at The George Washington University Hospital. His academic interest includes hematopathology and molecular pathology.

-Maikel Benitez Barzaga, MD is a Pathology Resident (PGY-2) at The George Washington University Hospital. His academic interest include hematology, microbiology, molecular and surgical pathology.

–Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.



















{kind=link}