A 21 year-old female presented to the emergency department with a sore throat. Her symptoms started two weeks prior to presentation. She was seen at student health last week and given Tamiflu, but her sore throat has grown progressively worse. She now has pain with swallowing and cannot swallow liquids. Upon examination the patient has no rash, no fever, and is not in respiratory distress. She does have left tonsillar fullness causing her uvula to be slightly deviated to the right along with an enlarged left cervical lymph node. Her complete blood count (CBC) was elevated at 19.7 x103/ul (reference range 4-10 x103/ul) with 12% lymphocytes, 2% monocytes, and 83% neutrophils. A rapid antigen test for S. pyogenes or Group A Streptococcus was negative. A CT exam of the neck was performed and a peritonsillar abscess of 1 x 1.3 x 1.6 cm was identified. The abscess was drained resulting in 1 ml of yellow purulent fluid which was sent to the microbiology lab for culture. The following was Gram stain was prepared from the abscess material.
Discussion
The Gram stain of this abscess showed 4+ PMNs and 4+ small, pleomorphic gram negative bacilli. Anaerobic culture grew Fusobacterium necrophorum, identified by MALDI-TOF MS with a confidence score of 2.2. F. necrophorum is a non-motile, non-pigment forming, pleomorphic gram negative bacilli. It is a strict anaerobe that tests catalase negative, indole positive, and lipase positive on egg yolk agar. Anaerobic antibiotic disk testing for this organism shows susceptibility to kanamycin and colistin with resistance to vancomycin.
The two most clinically relevant species of Fusobacterium are F. nucleatum and F. necrophorum. Because they are strict anaerobes which are often not recovered in culture, Fusobacterium spp. are an under-recognized cause of disease. F. necrophorum colonizes the oral cavity, and like other colonizing anaerobes, it tends to cause infections near the mucosal surface where it resides. F. necrophorum most commonly causes pharyngitis, recurrent tonsillitis, and other odontogenic infections. In adolescents, 10% of tonsillitis that is not caused by S. pyogenes can be attributed to F. necrophorum. These infections can progress to septic thrombophlebitis of the internal jugular vein (Lemierre’s syndrome), bacteremia, and rarely F. necrophorum can cause abscesses throughout the body. Because it is an anaerobic bacterium, susceptibility testing is rarely performed on isolates of F. necrophorum. They are highly susceptible to β-lactam–β-lactamase inhibitor combinations, carbapenems, and metronidazole.
Lemierre’s syndrome was of great concern in our patient since it is most commonly observed in adolescents and young adults that were previously healthy, like our patient. Fortunately, CT scan of the neck showed no indication of thrombophlebitis in our patient. After drainage of the abscess, she felt much better and was able to tolerate liquids. The patient was discharged from the ED with a course of amoxicillin/clavulanate (augmentin). Upon follow up in ENT clinic she gave a more through history of 4-5 episodes of sore throat over the past year.
References
Manual of Clinical Microbiology, 11th edition
Principles and Practices of Infectious Disease, 7th edition
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois.
As an unscheduled post, I’d like to make a quick side note separate from public health, zika, and medical school. You may have seen a post I wrote last January about the potential stereotypes and stigmas we might face in laboratory medicine. But, just because we as laboratory professionals operate behind-the-scenes most of the time, we’re still healthcare professionals—and clinician burnout can affect any of us.
I recently watched a video of Dr. Zubin Damania, also known as “ZDoggMD,” a primary care physician and founder of Turntable Health in Las Vegas. He’s a brilliant and passionate doctor with great opinions and an even greater creative sense of humor. Among his many parodies, and “rounds” Q&A questions, ZDoggMD recently had a guest on one of his Facebook shows called “Against Medical Advice” to address the serious issue of suicide and depression in medicine. Janae Sharp was the guest on this episode speaking about her husband, John, a physician fresh into his residency who committed suicide. They go on to talk about her life after this tragedy and how if flipped her and their children’s’ lives upside down. Janae’s described John as a father, a writer, a musician, an idealist, who always wanted to become a doctor. My interest was definitely piqued by this—I tend not to miss most of Dr. Damania’s content—and this is something I’ve been hearing more and more about as my path through medical school continues. But, at one point in the interview my heart just stopped: John was a clinical pathologist. Too close to home, for me at least. I was admittedly surprised.
Pathologist’s don’t have that much stress to make depression and suicide part of that life, I thought. But that is a cold hard assumption. Depression affects so many people at large, and when you’re in healthcare it almost seems like a risk factor on top of issues one might be struggling with. Med school is touted as one of the hardest intellectually, physically, and emotionally grueling experiences you could go through—I will personally vouch for Dr. John and Dr. Damania’s statements about how much these experiences push you to your limits. No sleep, no recognition, no support, fear of failure, imposter syndrome, a wealth and breadth of knowledge that makes you feel like you’re drowning—not to mention that if you do ask for help you’re immediately “lesser” for doing so.
Video 1. ZDoggMD interviews Janae Sharp about her tragic loss, her husband John’s suicide, and the rampant problem of depression and burnout in medicine. Against Medical Advice, Dr. Damania.
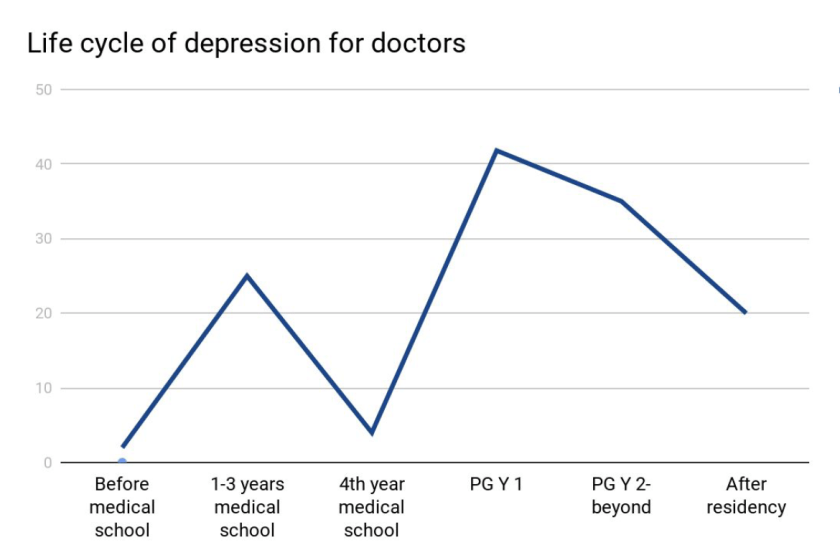
Last month, I was fortunate enough to attend a grand rounds session at my current hospital about this very topic. Presented by Dr. Elisabeth Poorman, internal medicine attending physician, and clinical instructor at Harvard Medical School, who talked about how (because of stigmas) medical trainees don’t get the help they need. She demonstrated that prior to med school students are pretty much on-par with their peers with regard to depression. However, once medical school starts, those peers all plummet together as depression rates rise and fall dramatically throughout the various stages of their careers. (I’m just going to go ahead and vouch for this too.) Dr. Poorman shared several case studies that effectively conveyed just how hard it can be when it seems like you are a source of help for many, but no one is there to help you. Story and story recounted the same model of apparent—and often secretive—burnout which ultimately led to a decrease in the quality of care, and in some instances suicide. Dr. Poorman was also brave enough to share her own story. No stranger to depression, herself, it was something that she encountered first hand. She connected herself with this increasingly difficult picture of inadequate support for those of us spending our lives serving others.
Figure 1. Dr. Poorman’s data reveals that depression rates for medical school classmates in a cohort generally rise and fall as their duties and responsibilities change during their career trajectory. I’m currently on the slope downward between the first 1-3 years of school’s peak and the 4th year trough.
There are clear problems facing those of us in healthcare jobs. An ironic consequence, however, of modern scientific advancement is the “doubling time” of medical knowledge. While not necessarily a problem, this refers to the amount, depth, and scope of knowledge physicians and medical scientists are expected to master in order to effectively treat, make critical clinical decisions, and educate our patients. While in 1980 it took 7 years for all medical knowledge to double in volume, it only took 3.5 years in 2010, and in 2020 it’s expected to double every 73 days!1. The problems come as a result of this knowledge because more data means more to do. More time on the computer, higher critical responsibility, and less time to focus on your own mental health all lend themselves to a cyclic trap of burnout. Physicians commit suicide at a rate of 1.5 – 2.3 times higher than the average population.1
Physicians, nurses, clinical scientists, lab techs, administrators, phlebotomists, PCTs—we’re all over worked, under-supported, fall victim to emotional fatigue, and have some of the highest rates for depression, substance abuse, PTSD, and suicide.1 Sometimes, reports from Medscape or other entities will report that burnout is a phenomenon of specialty, hypothesizing that critical nature specialties have more depression than lesser ones2 (the assumption that a trauma surgeon might burn out before a hematopathologist). But truthfully, this is just part of the landscape for all providers. A May 2017 Medscape piece wrote “33% chose professional help, 27% self-care, 14% self-destructive behaviors, 10% nothing, 6% changed jobs, 5% self-prescribed medication, 4% other, 1% pray.”3
So I’m talking about this. To get your attention. So that people reading know they’re not alone. So that people with friends going through something can lend a hand. I’m talking about this. ZDoggMD is talking about this. Jamie Katuna, another prolific medical student advocate, is talking about this. Dr. Elisabeth Poorman is talking about this. This is definitely something we should come together to address and ultimately solve.
What will you do to help?
This was a heavy topic. So in a lighter spirit, I have to share this with all of my laboratory family. If you haven’t heard or seen Dr. Damania’s videos yet, this is the one for you:
Thanks! See you next time!
References
Poorman, Elisabeth. “The Stigma We Live In: Why medical trainees don’t get the mental health care they need.” Cambridge Health Alliance, Harvard Medical School. Grand rounds presentation, Feb 2018. Bronx-Lebanon Hospital Center, New York, NY.
–Constantine E. Kanakis MSc, MLS (ASCP)CM graduated from Loyola University Chicago with a BS in Molecular Biology and Bioethics and then Rush University with an MS in Medical Laboratory Science. He is currently a medical student at the American University of the Caribbean and actively involved with local public health.
The patient is a 69-year-old man with a history of high-risk MDS (MDS-MLD-RS) diagnosed 1 year prior to his current visit. He was successfully treated with chemotherapy and bone marrow transplantation. For the next year, several marrow examinations were normal and chimerism analysis revealed >98% donor cells. Currently, he presents with vague symptoms and a CBC demonstrates marked thrombocytopenia of 4K/μL. The low platelet count is initially thought to be related to GVHD; however, a bone marrow examination is performed to assess the status of his disease.
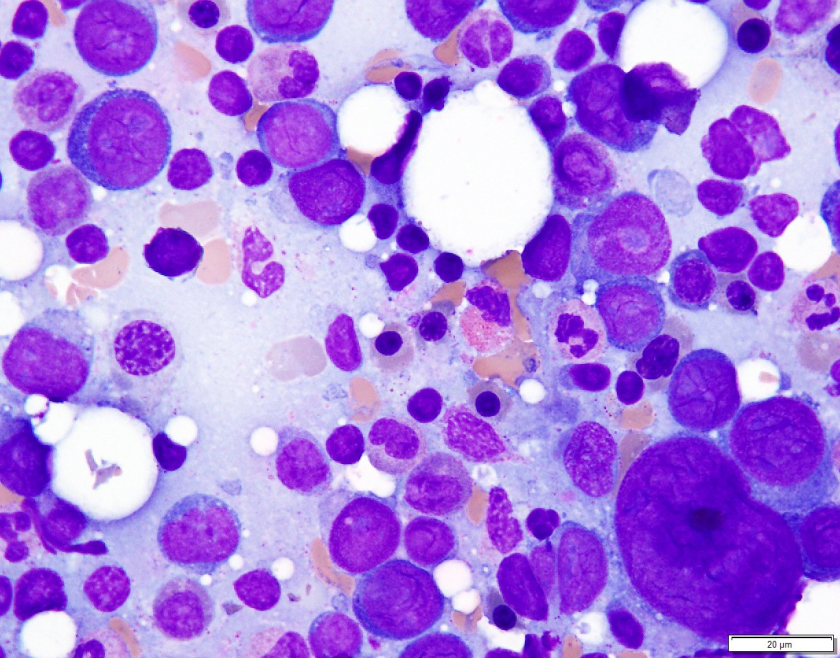
Examination of the bone marrow reveals a markedly hypercellular marrow for age with a proliferation of abnormal erythroid cells comprised of sheets of immature and maturing red cell precursors with basophilic cytoplasm. There is a marked increase in larger cells with deeply basophilic cytoplasm, prominent nucleoli, dispersed chromatin, perinuclear hoffs, and a high nuclear to cytoplasmic ratio consistent with pronormoblasts. These pronormoblasts comprised 31% of a 500-cell cell count. Additionally, the background marrow revealed a total of 81% erythroid precursors with marked morphologic atypia and dyspoiesis. Significant dysmegakaryopoiesis is noted. There is no significant increase in myeloid blasts.
Immunophenotyping
Immunohistochemical staining for E-cadherin, CD61 and CD34 is performed. These stains confirm no increase in CD34 positive blasts. CD61 highlights numerous dyspoietic megakaryocytes with widely separated nuclear lobes. E-cadherin staining is impressive, with over 80% of marrow cellularity shown to be comprised of E-cadherin positive erythroid cells.
Diagnosis
The patient’s history of MDS with current dyspoiesis, presence of >80% immature erythroid precursors with >30% proerythroblasts is diagnostic of Acute Myeloid Leukemia, NOS (Pure Erythroid Leukemia) per 2017 revision of the World Health Organization classification of myeloid neoplasms.
While successive chimerism reports thus far had shown >98% donor cells, the chimerism associated with this marrow biopsy reveals a decrease in the percentage of donor cells to 44% confirming the relapsed nature of his myeloid malignancy.
Discussion
Di Guglielmo syndrome, known as M6 leukemia in the FAB classification, was named after Giovanni Di Guglielmo, an Italian hematologist who first characterized the disease in 1917. After a few iterations in different classification schemes, the 2008 WHO Classification characterized two types of ‘erythroleukemia’ the erythroid/myeloid type and the pure erythroid leukemia. The former category of erythroid/myeloid type was removed in the 2017 update of the WHO classification with cases meeting criteria for that diagnosis now falling under the category of MDS. ‘Pure Erythroid Leukemia’ remains, and comes under the AML, NOS category, requiring >80% erythroid progenitors with > 30% proerythroblasts.
An extremely rare leukemia, PEL usually occurs as a progression of previous MDS and very uncommonly as de novo disease. Morphologically, PEL reveals proerythroblasts with deeply basophilic, agranular cytoplasm which is usually vacuolated. Occasionally, smaller ‘blasts’ with scant cytoplasm may resemble lymphoblasts. PEL is an exception to the rule of needing 20% ‘myeloid blasts’ to make an acute leukemia, since often the true myeloblast count is low.
In trephine core biopsies erythroid progenitors may take up an intra sinusoidal growth pattern with a sheet-like arrangement and typically reveal some element of background dysmegakaryocytopoiesis. When PEL lacks specific erythroid differentiation, it may be difficult to differentiate from other types of AML such as Acute Megakaryoblastic Leukemia. Park and colleagues recently categorized some under reported morphologic features of PEL and recurrent cytogenetic abnormalities associated with this disease. These findings included (but were not limited to) a broad morphologic spectrum of erythroblast morphology from undifferentiated blasts to proerythroblasts. They reported bone marrow tumour necrosis in trephine biopsies in over 70% of their cases. Of the cases wherein karyotyping was available, there was a highly complex and monosomal karyotype noted involving the TP53 gene locus.
PEL is associated with an aggressive course with a median survival of 3 months.
References
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, Bloomfield CD, Cazzola M, Vardiman JW. The 2016 revision to the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia. Blood. 2016 Jan 1:blood-2016.
Wang W, Wang SA, Jeffrey Medeiros L, Khoury JD. Pure erythroid leukemia. American journal of hematology. 2017 Mar 1;92(3):292-6.
Park DC, Ozkaya N, Lovitch SB. Acute leukaemia with a pure erythroid phenotype: under-recognized morphological and cytogenetic signatures associated universally with primary refractory disease and a dismal clinical outcome. Histopathology. 2017 Aug;71(2):316-321. doi: 10.1111/his.13207. Epub 2017 May 5.
-Michael Moravek, MD is a 2nd year anatomic and clinical pathology resident at Loyola University Medical Center. Follow Dr. Moravek on twitter @MoravekMD.
-Kamran M. Mirza, MD PhD is an Assistant Professor of Pathology and Medical Director of Molecular Pathology at Loyola University Medical Center. He was a top 5 honoree in ASCP’s Forty Under 40 2017. Follow Dr. Mirza on twitter @kmirza.
Former Lablogatory contributor Dr. Kristine Kraft has a great breakdown of an anemia multiple-choice question on her site Pathology Student. Check it out!
Case History
A 68 year old man presents with complaints of generalized weakness that started 3 weeks after his trip to the United Kingdom. The patient endorses night sweats, myalgia, fever, headaches, decreased appetite, mild nausea but no vomiting or diarrhea. He denied any history of recent rashes or arthralgia. The patient lives in a tick endemic area in the Northeastern part of the United States. Approximately 2 months ago he noticed an engorged tick while in the shower for which he completed a prophylactic course of doxycycline. He has sufficient titers for Lyme antibody; however no antibodies were present for Anaplasma. Blood smears were ordered for review.
Lab Identification
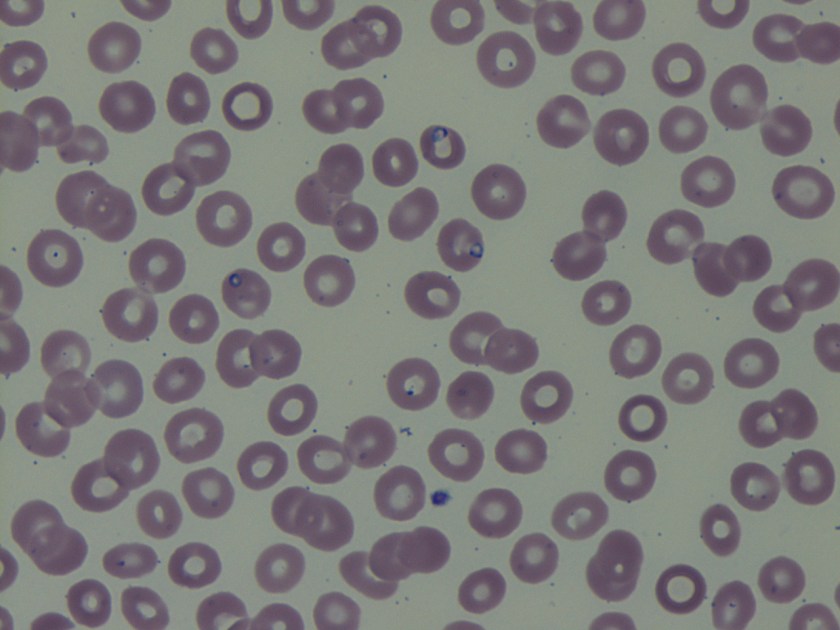
On the thin blood smears, there were multiple vacuolated, pleomorphic, ring-form like organisms seen in multiple infected red blood cells. No extracellular organisms were identified.
Image 1. Protozoa species on thin blood smears stained with Giemsa (100x oil immersion).
The organism was identified as a species of Babesia with 0.8% parasitemia and confirmed by PCR as Babesia microti.
Discussion Babesia species are infectious protozoa which infect and cause lysis of red blood cells. Symptoms develop over the course of weeks to months and vary in severity. The most common symptoms are nonspecific flu-like symptoms (e.g., fever, chills, body aches, weakness, fatigue). If left untreated patients can develop hemolytic anemia, thrombocytopenia, disseminated intravascular coagulation, hemodynamic instability, and possibly death.1
The main agents of human babesiosis are B. microti in the northeastern and upper midwestern regions of the United States, B. duncani in the western regions of the United States, and B. divergens in Europe. Occasionally on blood smears Babesia parasites can be difficult to differentiate from Plasmodium falciparum; Babesia species however are pleomorphic, vacuolated, and can appear inside red blood cells or outside red blood cells whereas Plasmodium falciparum are typically only seen inside red blood cells.1 In most cases the diagnosis for babesiosis can be made on the basis of morphological features on thick and thin smears. However, for patients with subclinical symptoms, very low parasitemia with undetectable organisms on blood smears and a high clinical suspicion for babesiosis serologic and molecular testing can be offered. Serologic testing has 88-96% sensitivity and 100% specificity in patients with no concurrent history of malarial infections. There is some possibility of cross-reactions in serum specimens in patients with malarial infections.2 Molecular techniques such as PCR are excellent tools for the purposes of screening and in addition can help to differentiate amongst the different variants of Babesia species.3 As in this case PCR was used to rule out possible infection with B. divergens due to the patient’s recent travel history to the United Kingdom. The two major antimicrobial regimens for babesiosis are atovaquone plus azithromycin for mild infection or quinine plus clindamycin for more severe infections.1
Krause PJ, Telford S RI, Ryan R, et al. Diagnosis of babesiosis: Evaluation of a serologic test for the detection of Babesia microti J Infect Dis 1994;169:923-926.
Hojgaard A, Lukacik G, Piesman J. Detection of Borrelia burgdorferi, Anaplasma phagocytophilumand Babesia microti, with two different multiplex PCR assays. Ticks and Tick-borne Diseases 2014 (5):349–351.
-Noman Javed, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.