Case History
A 42-year-old female presented with a right breast mass at an outside hospital that was concerning for carcinoma. A core needle biopsy was performed of right breast mass and the case was sent for expert consultation.
Diagnosis


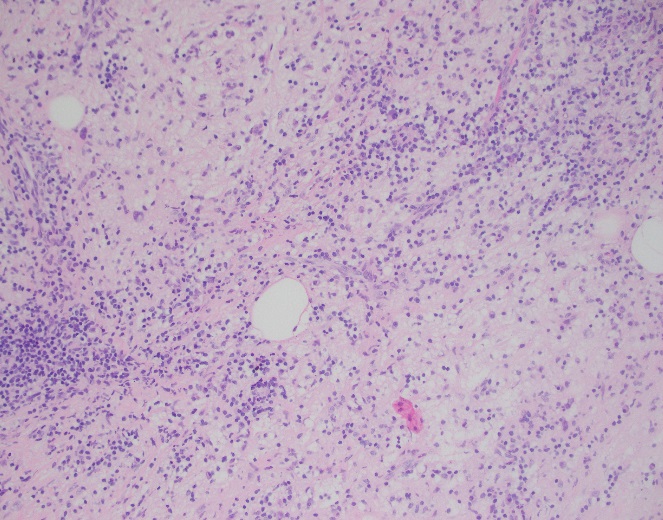
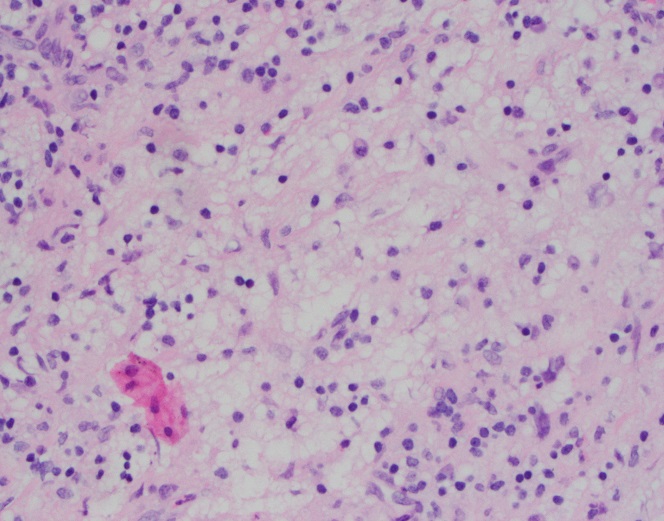
Sections of core needle biopsy material are composed primarily of adipose tissue shows a dense lymphohistiocytic infiltrate with histiocytes being the dominant cell type. Admixed plasma cells are present within the infiltrate. The histiocytes have abundant granular cytoplasm with irregular nuclear contours and some nuclei containing inconspicuous nucleoli. Frequent lymphocytic emperipolesis is identified. Immunohistochemistry performed at the outside facility show positivity for S100 and CD163 within the histiocytes, further highlighting the lymphocytic emperipolesis. Cytokeratin immunostains are negative.
Overall, the morphologic and immunophenotypic findings are consistent with a diagnosis of extranodal sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease).
Discussion
Sinus histiocytosis with massive lymphadenopathy (SHML) was first described by Rosai and Dorfman in 1969, however, similar findings may be present in extranodal sites thus earning the designation of Rosai-Dorfman disease (RDD). Although primarily present in lymph nodes, RDD may involve extranodal sites with sinuses and skin being the most frequently affected tissue types. Clinically, RDD often maintains a benign and self-limited course but may undergo exacerbations and recur, requiring surgical management. On histologic examination, RDD involves a rich inflammatory infiltrate with histiocytes, plasma cells, and lymphocytes. The histiocytes usually display a unique phenotype in which lymphocytes are phagocytosed, a process termed emperipolesis. By immunohistochemistry, these histiocytes are positive for S-100 and histiocytic markers (CD68 and CD163) and are negative for CD1a1.
The largest cohort studied involved 423 cases with 182 having extranodal manifestations2. Chest involvement was first reported by Govender et al. in 1997 in a 34-year-old female3. Overall, RDD is considered rare with a slight male predilection and young African-Americans being the most commonly affected. Sites involved ranging from most common to least common include lymph nodes, skin, upper respiratory tract, and bone4.
Extranodal sinus histiocytosis with massive lymphadenopathy, also known as Rosai-Dorfman disease, is a rare pathologic entity that histologically shows a dense lymphohistiocytic infiltrate and emperipolesis, a hallmark of the disease. Although lymph nodes are the most common site of involvement, extranodal sites may be affected and RDD should remain in the differential for lesions that contain abundant histiocytes, plasma cells, and lymphocytes as well as the classic feature of emperipolesis.
References
- Komaragiri et al.: Extranodal Rosai–Dorfman disease: a rare soft tissue neoplasm masquerading as a sarcoma. World Journal of Surgical Oncology 2013 11:63.
- Penna Costa AL, Oliveira e Silva N, Motta MP, Athanazio RA, Athanazio DA, Athanazio PRF: Soft tissue Rosai–Dorfman disease of the posterior J Bras Pneumol 2009, 35:717–720.
- Govender D, Chetty R: Inflammatory pseudotumour and Rosai–Dorfman disease of soft tissue: a histological continuum? J Clin Pathol 1997, 50:79–
- Montgomery EA, Meis JM: Rosai–Dorfman disease of soft tissue. Am J Surg Pathol 1992, 16:122–129.

-Phillip Michaels, MD is a board certified anatomic and clinical pathologist who is a current hematopathology fellow at Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA. His research interests include molecular profiling of diffuse large B-cell lymphoma as well as pathology resident education, especially in hematopathology and molecular genetic pathology.
