A 47-year-old male originally from Dominican Republic, with a recent diagnosis of acquired immunodeficiency syndrome (AIDS) and diffused large B cell lymphoma (DLBCL), was admitted because of seizures and a rapidly increasing left neck mass. MRI of the brain showed a 2.5 x 1.2 cm (about 0.47 in) lesion in the left inferior parietal lobe – (1.4×0.7cm) in the right frontal lobe, plus multiple scattered bilateral lesions. Because of this, he underwent craniotomy/craniectomy for possible resection. A biopsy was taken from the right temple lesion and sent for aerobic, anaerobic, fungal, mycobacterial culture, surgical pathology and Toxoplasma PCR (Polymerase Chain Reaction).
Gram stains, KOH prep, acid-fast stains, and Toxoplasma PCR of the tissue were all negative. Aerobic and anaerobic cultures did not show any growth.
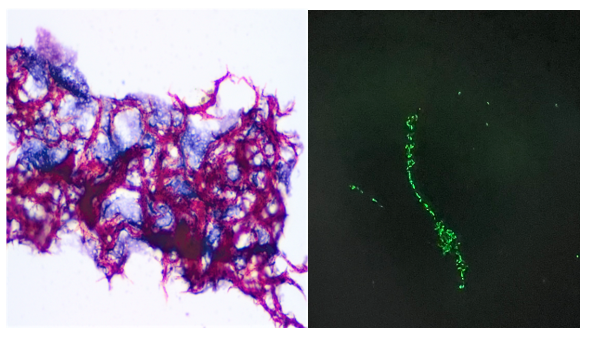
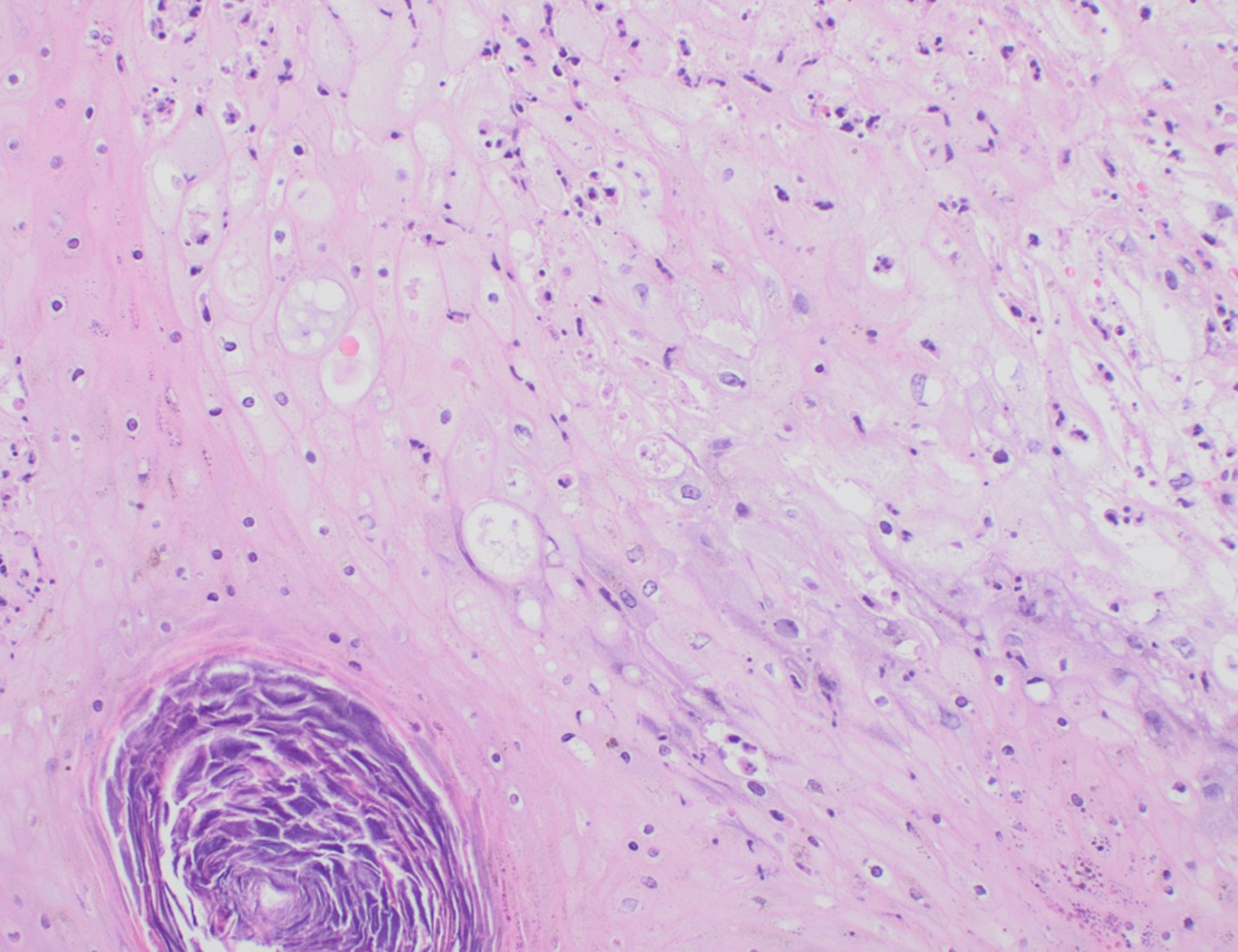
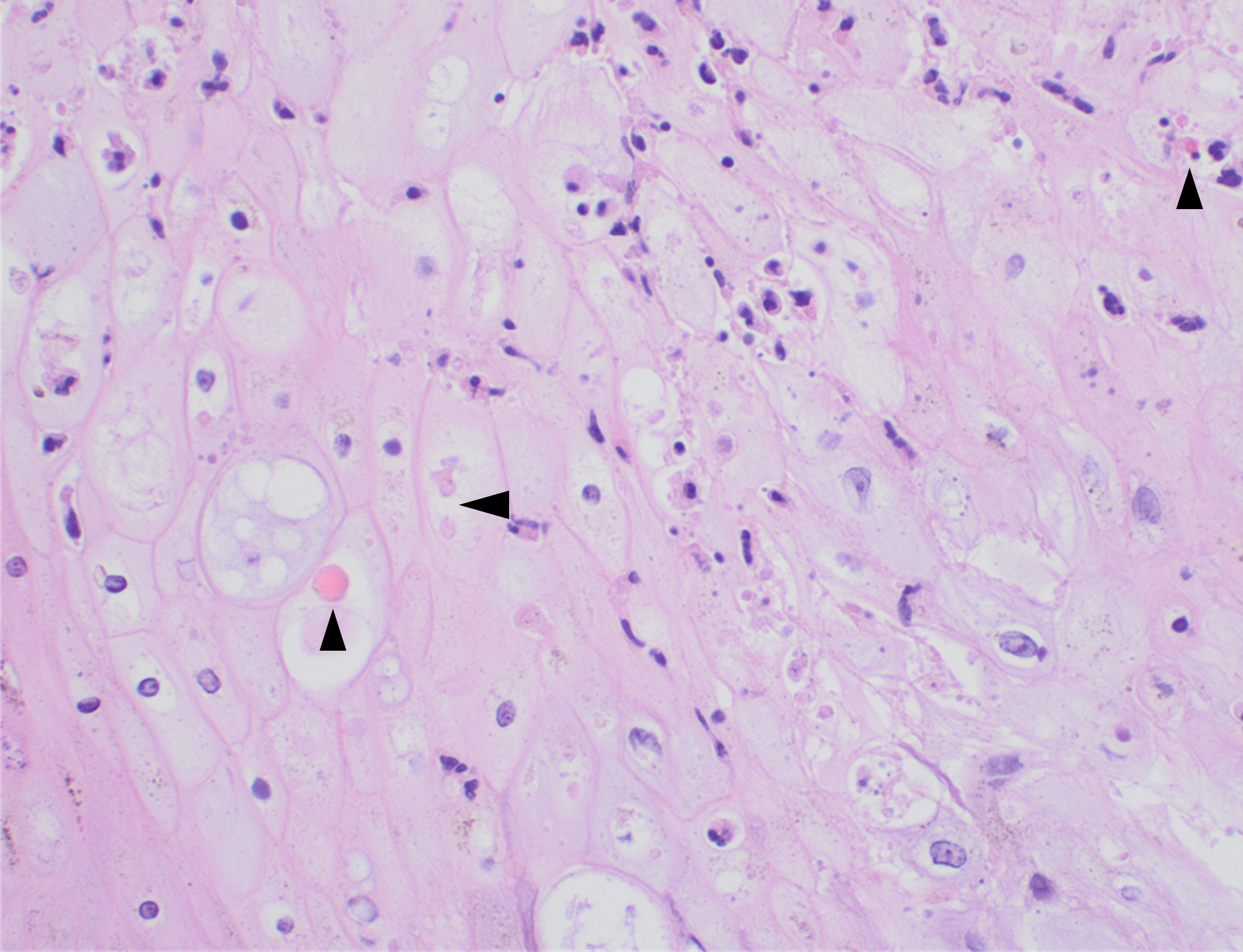
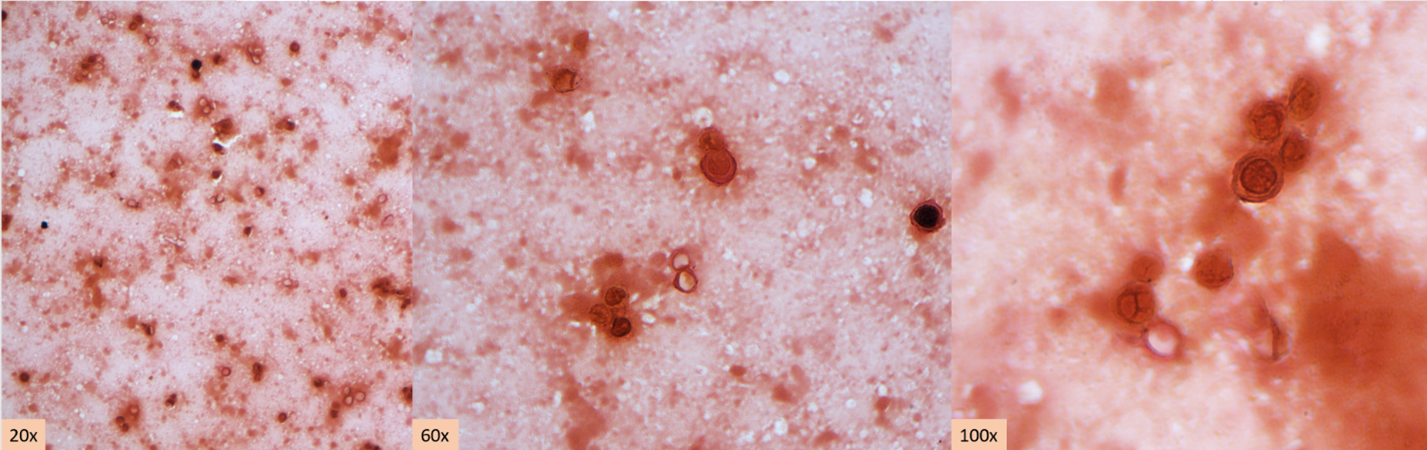
Histopathology slides (GMS and H&E stains in Fig A and B) show budding yeasts morphologically consistent with Cryptococcus. Mucicarmine stain was also positive. Lumber puncture was performed the next day and Cryptococcal antigen was positive, with a titer of 1:640. Interestingly, the CSF culture and Gram stain did not reveal any organisms.
Figure A. H&E shows encapsulated variably sized transparent/gray color yeasts with thin walls. Black arrows show organisms. Figure B. GMS stains highlight very faint staining of capsule (black arrow). Yellow arrow highlights background inflammatory cells.
Discussion
Among several species of Cryptococcus,C. neoformans and Cryptococcus gattii are pathogenic, with C. neoformans causing meningitis in immunocompromised patients worldwide whereas C. gattii has a preference for immunocompetent individuals.1 Cryptococcal disease remains a major opportunistic infection and a leading cause of mortality in patients infected with HIV in much of the developing world. Most HIV-related meningitis cases are caused by Cryptococcus neoformans.2
Cryptococci are found in soil, due to contamination with pigeon droppings. The infection occurs through inhalation, with or without symptoms of pneumonia, with subsequent dissemination to the central nervous system (CNS) via blood. Imaging findings are often unspecific or negative. CT or MRI examination of the central nervous system is performed to rule out alternative diagnoses. The diagnosis of ‘meningitis’ is made with a lumbar puncture, which typically shows lymphocytosis, an increased protein and decreased glucose concentration. Few neutrophil granulocytes are often found in CSF. This is likely because neutrophil migration is inhibited by specific polysaccharides that are part of the cryptococcal capsule.3
Cryptococci can be seen directly in the sediment of centrifuged CSF stained with India ink. The sensitivity and specificity of India ink is poor; therefore, CSF Gram stain and culture, multiplex meningitis/encephalitis PCR, and lateral flow antigen (LFA) tests have replaced the use of India ink. The cryptococcal lateral flow antigen test should be performed in CSF and serum, in addition to Multiplex ME PCR panel, and is a preferred test because of high sensitivity (93-100%) and specificity (93-98%).4
High organism burden at baseline (indicated by quantitative CSF culture or CSF antigen titre) and abnormal mental status are the most important predictors of death, while high opening pressures and a poor inflammatory response in the CSF have also been associated with poor outcome.5
On H&E it has the characteristic appearance ofencapsulated variably sized yeasts (2-20 microns) with thin walls which can be highlighted with the GMS stain. Although the presence of a capsule differentiates Cryptococcus from Histoplasma capsulatum and Blastomyces dermatitidis with the H&E or mucicarmine stain, additional confirmation can be made with Fontana-Masson stainin the absence of capsules.6 Since both C.neoformans and C. gattii produce melanin, the pathology report by FM silver or H&E/GMS stain cannot further distinguish these two closely resembled species.
Occasionally, cryptococcal meningitis cases with sterile CSF culture and/or negative Cryptococcal CSF antigen are observed in HIV individuals, regardless of the CD4 counts.7,8 However, serum Cryptococcal antigen and blood culture may be positive in those individuals.7 In our case, the diagnosis of Cryptococcal meningitis was made by the pathology report and positive CSF Cryptococcal antigen.
-Fnu Sapna is a 2ndyear AP/CP pathology resident in the Department of Pathology at Montefiore Medical Center in Bronx, NY.She completed her Medical education at Chandka Medical College in Pakistan.Her interests are putting efforts to improve screening guidelines for diagnosis of preventable gynecological and breast cancers.
-Phyu Thwe, Ph.D, D(ABMM), MLS(ASCP)CM is Associate Director of Infectious Disease Testing Laboratory at Montefiore Medical Center, Bronx, NY. She completed her medical and public health microbiology fellowship in University of Texas Medical Branch (UTMB), Galveston, TX. Her interests includes appropriate test utilization, diagnostic stewardship, development of molecular infectious disease testing, and extrapulmonary tuberculosis.
A 74-year-old female from El Salvador with a medical history of hypertension, diabetes, osteoarthritis presented with persistent productive cough. The patient states that the symptoms started on November 2022 which was believed to be associated with ongoing COVID-19 infection. Despite recovery from COVID-19 infection, significant productive cough still remained. A visit to her primary care doctor revealed streptococcal throat infection and despite completing a course of Zithromax antibiotics, a subsequent chest x-ray revealed potential right upper lobe pneumonia and she reported productive cough with occasional blood streaks. Blood work up in the Emergency Department revealed leukocytosis (20.22 x10e3/mcL) with neutrophilia (14.56 x10e3/mcL neutrophils) and monocytosis (3.03 x10e3/mcL monocytes). A chest x-ray showed bilateral reticular and airspace opacities with an air-fluid level containing opacity overlying the left mid lung, likely representing a cavitary lesion. A follow up with a computerized tomography of the chest identified innumerable randomly distributed pulmonary nodules or cavities with upper lobe predominance. The largest cavity measures approximately 6.6 cm with air-fluid levels and debris. Additionally, a small pericardial effusion with thickened pericardium was also noted. A sputum sample was submitted for Acid-fast bacilli (AFB) culture and molecular testing. AFB stain was positive for acid-fast bacilli (Figure 1). The GeneXpert MTB/RIF assay detected M. tuberculosis with no rifampin resistance marker. Growth on the Lowenstein-Jensen agar after two weeks showed buff colored rough and dry colonies and was confirmed as M. tuberculosis on the MALDI-TOF.
Figure 1. Visualization of acid-fast bacilli directly from patient specimen. Using acid-fast stain, cording was observed (Figure 1A, left) and using fluorescent staining, fluorescent rods were observed (Figure 1B, right).
Discussion
Mycobacteria are aerobic, nonmotile, thin rod shape, non-spore forming bacilli that possess mycolic acid in its cell wall giving its acid-fast stain characteristics. Tuberculosis (TB) is an airborne disease caused by Mycobacterium tuberculosis (MTB). TB remains to be the leading cause of death from a single infectious agent worldwide. According to the CDC a total of 1.6 million people died from TB in 2021 (including 187, 000 people with HIV) 1,2. The M. tuberculosis complex (MTBC) includes M. tuberculosis, M. bovis, M. bovis, Bacille Calmette-Guérin strain (BCG), M. caprae, M. pinnipedii, M. mungi,M. africanum, M. microti, and M. canettii3. M. tuberculosis produces cord factor, a glycolipid which is also known as trehalose dimycolate, that causes the bacteria to grow in parallel strands and that appeared like cord, or rope when cultured in liquid media (Figure 1A). The cord factor is present in the outer envelope and protects the bacteria from the host response 4.
The pathogenesis of human tuberculosis involves a complex interaction between host immune system and bacterial factors 4. M. tuberculosis is carried in airborne particles generated by infected individuals. The droplet nuclei traverse the mouth or nasal passages, upper respiratory tract, and bronchi to reach the alveoli of the lungs. The bacteria are then phagocytosed by alveolar macrophages and can inhibit maturation of phagosome and block formation of phagolysosome, allowing its unchecked replication in the macrophage which results in bacteria proliferation in the alveolar macrophage and air spaces. In immunocompetent hosts, the immune response (via TLR2, TLR9, Th-1 and IFN- ꝩ cascades) may contain the infection before significant tissue destruction or systemic illness 1-4. However, in the immunosuppressed hosts, the primary infection results in a broad clinical spectrum such as meningitis, miliary tuberculosis and extrapulmonary granulomas. Post-primary/secondary tuberculosis (reactivation TB) usually begins months to years after the establishment of systemic immunity in primary TB mostly in a period when the host immune response is weakened, following exogenous or a large inoculum of virulent bacilli overwhelming the host immunity system. Extrapulmonary manifestations will develop based on the organ system affected 5.HIV infection is the greatest risk factor for reactivation of TB as the virus causes functional abnormalities in CD4+ T cells and CD8+ T cells which confer protection against active TB. Other risk factors that promote the reactivation TB include aging, malnutrition, diabetes mellitus, renal failure, cancer and immunosuppressive therapy 5. The disease typically affects the lungs (pulmonary TB) but can affect other sites as regional lymph nodes, apex of the lung, larynx, kidneys, brain, bone, joints and pleura 1,2,5.
Diagnostic tests for TB detect either the bacteria or host immune response. Specimens recommended for diagnosis of mycobacterial infection are sputum, bronchial brushing/washings /biopsies, gastric aspirates (children) urine, blood, CSF, BM, body fluids, stool (only in HIV) 5,8. Specimens from sputum and other nonsterile sites should be liquefied with N-acetyl-L-cysteine and decontaminated with NaOH and for gastric aspirate neutralized with buffer 6-8. For diagnostic purposes, all persons suspected of having TB disease at any site should have at least three consecutive sputum specimens collected in 8 to 24 hours with at least one being an early morning one for AFB smear and culture 1,8.
The organisms can be visualized under a microscope using two principal methods: carbolfuchsin staining (e.g., Acid-fast stain), or using a fluorochrome (auramine-rhodamine and auramine-O stains) procedure (Figure 1B). Microscopy is the most rapid diagnostic method for the detection of tubercle bacilli but is less sensitive; it requires a minimum of 10,000 bacilli/mL of sputum to produce a positive result. Culture is the gold standard and more sensitive method for the detection of tubercle bacilli and is necessary for performing antimicrobial drug drug-susceptibility testing and genotyping. 6,9 However culture requires 3–6 weeks for growth which delays the initiation of anti-tuberculosis drug therapy. Two types of solid media are used for mycobacterial culture: egg based (Löwenstein-Jensen) and agar based (Middlebrook 7H10, 7H11, and selective 7H11). Colony morphology of Mycobacterium tuberculosis on solid media are dry, rough, raised, wrinkled, off white to buff colored. M. tuberculosis is commonly positive for niacin, nitrate reduction test, pyrazinamidase test, but negative for 68C catalase, tween 80 hydrolysis, and 5% NaCl tolerance. Molecular techniques such as nucleic acid amplification tests revolutionized tuberculosis diagnosis since M. tuberculosis nucleic acid material can be detected directly from specimen in less than 2 hours. Two commercial NAATs for the detection of M. tuberculosis complex are available in the United States: The Amplified MTD (Mycobacterium Tuberculosis Direct) test (Hologic, Marlborough, MA) and the Xpert MTB/RIF (Cepheid, Sunnyvale, CA).
Common serological approaches for detection of M. tuberculosis are the Tuberculin skin test (TST) or IFN- ꝩ release assays (IGRA’s) 1,9,10. The tuberculin skin test is performed by intracutaneous injection of purified protein derivative of M. tuberculosis, which induces a visible and palpable induration that peaks in 48 to 72 hours. A false-positive tuberculin skin test may result on individuals with prior vaccination with BCG (Bacillus Calmette-Guerin), an attenuated strain of M. bovis. BCG immunization does not affect the test result of IGRA assay. The IGRA are blood tests that measure a person’s immune reactivity to M. tuberculosis. Both T-Spot and QuantiFERON can aid in diagnosis M. tuberculosis but do not differentiate latent infection from tuberculosis disease. IGRAs are in vitro tests that measure the IFN- γ production by T cells responding to stimulation with specific TB antigens ESAT-6, TB7.7, and CFP-10, which are not present in the M. bovis strains. Results can be interpreted both qualitatively (positive, negative, or indeterminate) and quantitatively.
The regimen currently recommended for treatment of TB is isoniazid, rifampin, ethambutol, and pyrazinamide. The initial M. tuberculosis isolate should be tested for resistance to first-line medication. Second-line drug susceptibility testing should be limited to specimens from patients who have prior TB disease treatment, contact with a patient with known TB drug resistance or positive cultures after more than 3 months of treatment 10. Multidrug-resistant TB (MDR TB) disease is defined as resistance to isoniazid and rifampin, and Extensively drug-resistant TB (XDR TB) is characterized with resistance to isoniazid and rifampin, any fluoroquinolone, and at least one of three injectable second-line drugs (i.e., amikacin, kanamycin, or capreomycin). The duration of therapy depends on the drugs used, the drug susceptibility test results, and the patient’s response to therapy. Most patients are started with a 6-month regimen plan. A difficult challenge to M. tuberculosis treatment is patient compliance with lengthened therapy. Without treatment mortality rate for tuberculosis is more than 50% 11.
Kamholz, S. L. 1996. Pleural tuberculosis, p. 483-491. In W. N. Rom and S. Garay (ed.), Tuberculosis. Little, Brown and Co., Boston, Mass.
Yanti, B., et al. The role of Mycobacterium tuberculosis complex species on apoptosis and necroptosis state of macrophages derived from active pulmonary tuberculosis patients. BMC Res Notes. 2020; 13: 415. doi: 10.1186/s13104-020-05256-2
Smith, Issar.Mycobacterium tuberculosis Pathogenesis and Molecular Determinants of Virulence Clin Microbiol Rev. 2003 Jul; 16(3): 463–496. doi: 10.1128/CMR.16.3.463-496.2003
Wells, C.D, et al. HIV infection and multidrug-resistant tuberculosis: the perfect storm. J Infect Dis. 2007 Aug 15;196 Suppl 1:S86-107. doi: 10.1086/518665.
Dunn, J.J., Starke, J.R., Revell, P.A. Laboratory Diagnosis of Mycobacterium tuberculosis Infection and Disease in Children. J Clin Microbiol 2016 Jun;54(6):1434-1441. doi: 10.1128/JCM.03043-15.
Parashar D, Kabra S, Lodha R, Singh V, Mukherjee A, Arya T, Grewal H, Singh S. 2013. Does neutralization of gastric aspirates from children with suspected intrathoracic tuberculosis affect mycobacterial yields on MGIT culture? J Clin Microbiol 51:1753–1756.
Clinical and Laboratory Standards Institute. 2008. Laboratory detection and identification of mycobacteria; approved guideline—1st edition. CLSI document M48-A. Clinical and Laboratory Standards Institute, Wayne, PA.
Pai M, Nicol MP, Boehme CC. Tuberculosis Diagnostics: State of the Art and Future Directions. Microbiol Spectr 2016; 4.
Dheda, K. et al. The epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant, extensively drug-resistant, and incurable tuberculosis. Lancet Respir Med. 2017 Mar 15;S2213-2600(17)30079-6.
-Dr. Carla Ayala-Soriano was born and raised in Bayamon, Puerto Rico. She attended Universidad Autonoma de Guadalajara School of Medicine where she received her doctorate degree. She completed a Bachelor of Science in Biology at the University of Puerto Rico. She spent an additional year completing a Post Bachelor Certificate in Cytotechnology. Her academic interests include Cytopathology and Gynecologic Pathology. In her spare time, Dr. Ayala-Soriano enjoys cooking, traveling, listen to music, and outdoor activities. She is pursuing AP/CP training.
-Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.
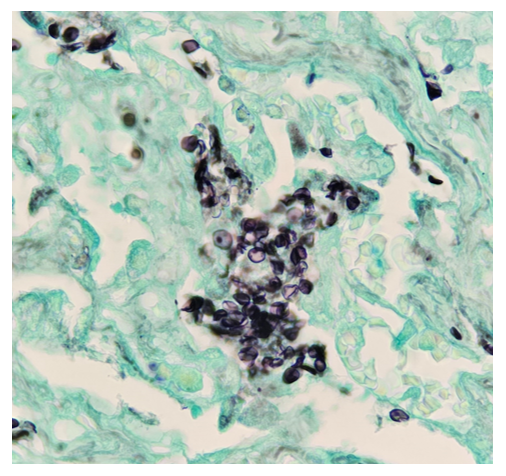
A 21-year-old male with no significant past medical history presented to the emergency department for acute hypoxemic respiratory failure. He also reported a productive cough with green sputum and unintentional 30 lb weight loss over the past 5 months. On presentation, his oxygen saturation was in the 80s on room air and initial labs were significant for lactic acidosis and a reactive HIV Ag/Ab. His HIV viral load was 1,359,029 copies/mL with a CD4 count of 37 cells/mm3 . Imaging included a chest X-ray and chest CT, which revealed left sided pneumothorax and diffuse ground glass opacities with scattered areas of consolidation. Based on his clinical presentation and CD4 counts <200 cells/mm3, the patient was started on trimethoprim/sulfamethoxazole (TMP/SMX) for PCP prophylaxis. A bronchoalveolar lavage was performed but had no growth on bacterial and fungal cultures. On hospital day 5, the left-sided pneumothorax was persistent despite multiple chest tube placements and a right-sided pneumothorax had formed, and the patient underwent video-assisted thoracoscopic surgery and pleurodesis. During the procedure, a ruptured bleb was found at the apex of the upper lobe of the left lung and a limited apical wedge resection was performed. Pathologic examination of the resection was significant for foamy exudate-filled alveoli on H&E staining. GMS stain revealed cup-shaped organisms confirming the presence of Pneumocystis jirovecii. The patient was continued on TMP/SMX for 21 days total and weaned off supplemental oxygen with follow-up scheduled at an HIV clinic.
Figure 1. Hematoxylin and Eosin lung tissue sections show alveolar spaces filled with pink, foamy amorphous material (20x and 100x magnification)Figure 2. GMS stain show alveolar spaces filled with Fungi 4 – 6 microns, cup / boat shaped cysts (100x magnification)
Discussion
Pneumocystis jirovecii pneumonia (PCP pneumonia) is a life-threatening infection found in immunocompromised patients, with approximately a third of patients affected being HIV-positive.1 Although the incidence of infection in HIV-positive patients is declining with modern therapies, it is still commonly seen in undiagnosed HIV-positive patients who present late in the course of the disease.2
Clinically, PCP pneumonia is characterized by dyspnea, tachypnea, cough, and fever in an immunocompromised patient. Chest imaging features include bilateral interstitial infiltrates and a “ground glass” appearance on CT. Because Pneumocystis is extremely challenging to culture, diagnosis relies on these clinical findings with confirmation by staining or PCR testing of bronchoalveolar lavage fluid or lung biopsy.3 Stains that can be used to identify PCP pneumonia include Gromori-methenamine silver (GMS) stain, calcofluor white (CW) stain, Toluidine Blue O (TBO) stain, with GMS and CW stains having the highest sensitivity.3,4 On GMS stain, the cyst wall of Pneumocystis will appear black with a “crushed ping-pong ball” or crescent shaped appearance.
Treatment with TMP/SMX should be started in patients with suspected PCP pneumonia while work-up is pending. Corticosteroids can also be added to the treatment regimen in patients with more severe respiratory symptoms (5). After completion of 21 days of therapy, a lower-dose of TMP/SMX should be continued in HIV-positive patients with CD4+ counts less than 200 for prophylaxis.5
References
Roux, Antoine, et al. “Pneumocystis Jirovecii Pneumonia in Patients with or without AIDS, France.” Emerging Infectious Diseases, vol. 20, no. 9, 2014, pp. 1490–1497, https://doi.org/10.3201/eid2009.131668.
White, P. Lewis, et al. “Pneumocystis Jirovecii Pneumonia: Epidemiology, Clinical Manifestation and Diagnosis.” Current Fungal Infection Reports, vol. 13, no. 4, 2019, pp. 260–273, https://doi.org/10.1007/s12281-019-00349-3.
Bateman, Marjorie, et al. “Diagnosing Pneumocystis Jirovecii Pneumonia: A Review of Current Methods and Novel Approaches.” Medical Mycology, vol. 58, no. 8, 2020, pp. 1015–1028, https://doi.org/10.1093/mmy/myaa024.
Procop, G. W., et al. “Detection of Pneumocystis Jiroveci in Respiratory Specimens by Four Staining Methods.” Journal of Clinical Microbiology, vol. 42, no. 7, 2004, pp. 3333-3335, https://doi.org/10.1128/jcm.42.7.3333-3335.2004.
Vilar, et al. “The Management of Pneumocystis Carinii Pneumonia.” British Journal of Clinical Pharmacology, vol. 47, no. 6, 1999, pp. 605–609, https://doi.org/10.1046/j.1365-2125.1999.00966.x.
-Alice Ann Lever is a fourth-year medical student at the Medical College of Georgia. She is interested in hematopathology and surgical pathology.
-Hasan Samra, MD, is the Director of Clinical Microbiology at Augusta University and an Assistant Professor at the Medical College of Georgia.
Against the backdrop of COVID-19, the world experienced a multicounty outbreak of Mpox (formally monkeypox) beginning in May of 2022. Prior to that time, the virus was primarily known to circulate within central and west African nations causing zoonotic disease. Clinical presentations of Mpox comprise signs and symptoms including rash on the hands, feet, face or mucous membranes and patients may experience fever or an influenza-like illness.1 Historically, transmission was associated with travel to an endemic region and contact with an infected animal. Importantly, the outbreak in 2022 was associated with broad changes in Mpox epidemiology, as most infections were acquired via sexual transmission.
Pox viruses and Mpox
Pox viruses are members of the family Poxviridae, which are double stranded DNA viruses that replicate entirely in the cytoplasm of host cells. They have worldwide distribution and cause disease in humans and other animals. Infection typically manifests as the formation of lesions, skin nodules or rash. Mpox belongs to the genus Orthopoxvirus which also includes other clinically important viruses including variola virus (smallpox), vaccinia virus, and cowpox. In the context of diagnosis, differentiation between the members of the Orthopox family becomes important.
The duration of illness with Mpox is usually between 2-4 weeks, with a variable incubation time most often between 6-13 days. The Mpox rash has historically been more focused on the face and extremities,2 and will cycle through stages including encrustation, scabbing, and eventually resolution. During the 2022 outbreak, an increasing number of presentations involved the anogenital and oral regions, further highlighting the change in epidemiology. The window for transmission is currently an area of active research as new data suggests transmission can begin prior to the appearance of symptomology.3
Diagnosis – Molecular
Mpox is generally diagnosed using PCR testing from a swabbed lesion. At the onset of this emerging infectious disease, the CDC shared its algorithm and testing for Mpox with public health laboratories. The first-generation algorithm largely reflected its potential use as a tool for screening for bioterrorism agents, which included using two-tiered testing. The first test was designed to demonstrate that Orthopox DNA was present and rule out variola virus by targeting the Orthopox DNA polymerase gene found not present in Variola (E9L-NVAR). The second step was to target an Mpox-specific gene encoding the envelope protein (B6R).4 It soon was readily apparent that the only Orthopox virus in circulation was Mpox, so the CDC updated its guidance in late June 2022 to confirming diagnosis of Mpox with the single Orthopox DNA-polymerase PCR assay.
However, despite this modification to improve expediency and like the situation faced at the onset of the COVID-19 pandemic, the need for testing greatly exceeded what public health infrastructure could support. Thus, laboratories designed and validated laboratory developed tests (LDTs) to expand access to testing, thus enabling physicians to interrogate the causes of a patient’s rash more thoroughly. This flexibility was essential given rising cases numbers and relatively non-specific symptomology of Mpox. By May 2023, over 80 laboratories registered Mpox LDTs with the Food and Drug Administration,5 and commercial device manufacturers are now including it in new and forthcoming assays still in development.
Diagnosis – Histopathology
Although PCR testing is the mainstay of diagnosis, histopathologic evaluation of biopsy material from a lesion can also provide insight into the viral etiology. Mpox infected skin biopsies demonstrate similar histopathologic features of infections caused by other pox viruses. As the rash continues to evolve over time, representative histopathological changes can also be observed. Early lesions may demonstrate ballooning degeneration, acanthosis and spongiosis. More mature lesions progress to near total keratinocyte necrosis with exocytosis comprised of mixed cellular inflammatory infiltrate.6 Eosinophilic bodies may be identifiable in the cytoplasm of infected cells, commonly known as Guarnieri bodies, represent the mature virions produced in the cytoplasm of infected cells.
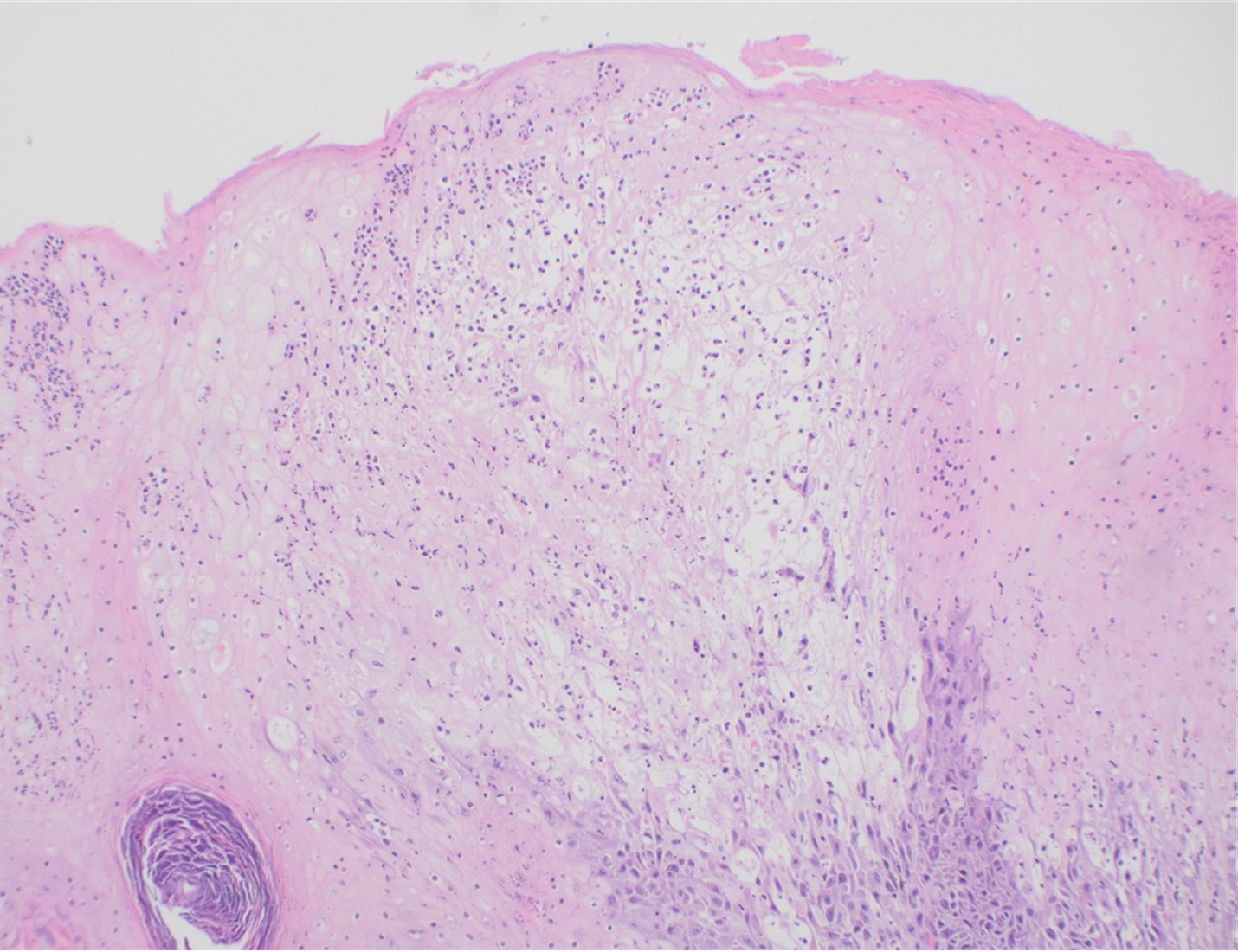
Recently, the histopathological description of 20 outbreak-associated clinical cases of Mpox from Spain was reported. Epidermal necrosis and keratinocytic ballooning were commonly encountered microscopic features associated with Mpox lesions.7 Figure 1 is a skin biopsy from a patient who presented with a vesicular eruption in September with a history of mpox, syphilis and herpes simplex infection whose lesions were worsening. It similarly shows ballooning degeneration, epidermal necrosis, exocytosis of neutrophils into the epidermis, and intracytoplasmic eosinophilic inclusions (Guarnieri bodies) (Figures 2-3).
Figure 1. Histopathology of MPOX from a biopsied skin lesion (4x magnification, H&E). Intact epidermis with evidence of ballooning keratinocyte degeneration and infiltration of neutrophils.Figure 2. Histopathology of Mpox (10x magnification, H&E). Epidermis with a cross-section of follicular infundibulum (hair follicle) is in the bottom left. The keratinocytes to the right demonstrate marked vacuolar change and small eosinophilic bodies can be observed in a background of neutrophils and necrotic keratinocytes.Figure 3. Histopathologic findings of MPOX in a biopsy of a skin lesion (40x magnification, H&E). High power magnification of viral inclusions, guarnieri bodies, (arrowheads) in a background of necrotic keratinocytes and neutrophilic infiltrate.
Treatment
Mpox is much milder than smallpox despite similar rash manifestations. In cases of severe Mpox infection, therapies used for smallpox have been compassionately utilized, but supportive measures are the mainstay of management of uncomplicated cases. Vaccination is now available as both a pre-exposure prophylaxis and post-exposure prophylaxis. It is important to note that the clinical effectiveness of the currently used vaccine in the United States is not known; however, early data across 32 US jurisdictions showed that among males 18-49, those who were unvaccinated had an Mpox incidence 14 times higher than similarly aged males who received at least one dose of vaccine at least 2 weeks prior.8
Conclusion
The Mpox outbreak, declared a global health emergency in July of 2022, has reinforced the need for flexibility within laboratories and industry to respond to emerging infectious diseases. The global health emergency for Mpox was declared over on May 11, 2023, but cases are still going to sporadically occur and minor outbreaks will result. The rapid development of numerous LDTs was essential to support the overwhelmed public health infrastructure, and this continued flexibility is needed to appropriately respond to future public health emergencies.
Rodríguez-Cuadrado FJ, Nájera L, Suárez D, Silvestre G, García-Fresnadillo D, Roustan G, Sánchez-Vázquez L, Jo M, Santonja C, Garrido-Ruiz MC, Vicente-Montaña AM, Rodríguez-Peralto JL, Requena L. Clinical, histopathologic, immunohistochemical, and electron microscopic findings in cutaneous monkeypox: A multicenter retrospective case series in Spain. J Am Acad Dermatol. 2023 Apr;88(4):856-863. doi: 10.1016/j.jaad.2022.12.027. Epub 2022 Dec 26. PMID: 36581043; PMCID: PMC9794029.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
-Travis Vandergriff, MD is an Associate Professor and Board-Certified Dermatopathologist and practicing Dermatologist at UT Southwestern Medical Center.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
A 35 year old male presented to the emergency department with left-sided chest pain, a new cough and pain that gets worse with inspiration. The past medical history was significant for HIV, recurrent syphilis, rectal high-grade dysplasia, proctitis with possible rectal abscess with concomitant Herpes Simplex Viral infection and Cytomegalovirus colitis. This patient was not compliant with antiretroviral therapy (ART) and his CD4 count was <100 at admission. In the ED, a chest X-ray was performed which revealed bilateral patchy, peripheral mass-like opacities with ground glass halos (Figure 1). Routine respiratory cultures of sputum and bronchoalveolar lavage (BAL) revealed no significant observations; mainly respiratory flora was reported. However, hematology staining of BAL revealed multiple fungal elements consistent with Pneumocystis jirovecii organisms (Figure 2).
Bilateral patchy airspace opacities with a loculated left pleural effusion (Figure 1, top). Wright Giemsa staining of Pneumocystis jirovecii cysts (with intracystic bodies, dots in the cysts) in a bronchoalveolar lavage specimen (Figure 2, bottom).
Discussion
Previously classified as a protozoa, Pneumocystis jirovecii (formerly known as Pneumocystis carinii) is currently considered a fungus based on nucleic acid and biochemical analysis. Stringer et al. proposed the change in nomenclature in early 2002, in honor of the Otto Jirovec, who was credited by some, as the original descriptor of the organism in human hosts.1 A few Pneumocystis species have been described in a wide variety of mammalian hosts but P. jirovecii is only capable of infecting humans and is not capable of infecting other animals.4P. jirovecii infection mostly affects the immunocompromised patients and can lead to severe, life-threatening disease. HIV is one of the most commonly encountered underlying diseases, but individuals with cancer, transplant recipients and hosts receiving immunosuppressive medication can be at risk. The route of transmission is thought to be person to person through air transmission. Immunocompetent hosts can act as reservoirs of the organisms and spread it to the immunocompromised. The use of antiretroviral therapy and prophylactic medication on HIV patients has substantially decreased the incidence of PJ infection in this population.2, 3 Defects in cellular immunity, specifically CD4+ T-cell-mediated immunity is a predisposing factor for the development of severe Pneumocystis infection. The disease is usually a pneumonia that can have a slow progression or progress rapidly. Fever, nonproductive cough, tachypnea, and severe dyspnea with hypoxia are the most common symptoms.
Induced sputum, bronchoalveolar lavage fluid, or lung tissue are the commonly accepted specimens received in clinical laboratories for direct diagnosis of P. jirovecii. Microscopically, the life cycle of Pneumocystis consists of at least two different life cycle forms of Pneumocystis organisms: the trophic form and the cyst form. The trophic form generally measures ∼2 µm in greatest diameter and in contrast, the cyst is significantly larger, measuring ∼8–10 µm in greatest diameter. The rigid Pneumocystis cyst wall is formed of β-glucan, which warrants detection of systemic Pneumocystis infections using Fungitell testing.4 Trophic and cyst forms can be detected with Papanicolaou, Gram-Weigert, or Wright Giemsa, Gomori methenamine silver (GMS), or calcofluor white. The sensitivity of the interpretation of these stains depends upon the expertise of the observed to differentiate Pneumocystis from artifacts and other fungi such asand Histoplasma capsulatum. The use of monoclonal antibodies with Immunofluorescent antibody stains directed against human Pneumocystis epitopes, can enhance direct detection of this organism in clinical specimens.5
Because the sensitivity of special stains and the microscopy depends, in part at least, on the experience and skill of the microscopist, polymerase chain reaction (PCR) has become a newer and promising testing method for P.jirovecii DNA detection. It is recommended that PCR should be done in cases with only mild to moderate immunosuppression because these individuals may have a lower burden of the fungus and clinical and radiologic findings are less developed compared to severely immunosuppressed patients.6 Another advantage of PCR is the ability to quantify the amount of P. jirovecii in the specimen, which has been suggested to help distinguish individuals who may be colonized versus those with true P. jirovecii associated pneumonia.7
The drug of choice for prophylaxis against or treatment of P. jirovecii is trimethoprim-sulfamethoxazole. Prophylaxis may generally be started on HIV positive patients once the CD4+ is <200cells/microL, CD4% is <14%, and/or patients have a detectable viral load.8
–Ilianne Vega Prado is a PGY-3 pathology resident at George Washington University. She has worked as a Microbiology technologist for a few years before completing her medical degree. Her academic and research interest include antibiotic stewardship, cytopathology, and breast pathology.
-Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.
A 25 year old male with severe right lower quadrant abdominal pain, fever and history of congenital neutropenia and thrombocytopenia presented to the emergency department. The patient reported experiencing similar episodes over the previous six months, sometimes requiring hospitalization. His symptoms would typically improve following several days of antibiotic therapy and were thought to be secondary to typhlitis. He reported that his current symptomology was more severe than any of the previous episodes. In the emergency department, the patient was found to be tachycardic and severely hypotensive, prompting admission for sepsis and empiric antimicrobial therapy with piperacillin/tazobactam and vancomycin. Imaging at the time revealed severe terminal ileitis with mild pancolitis, markedly worsened from a study obtained months prior during a previous episode. After failing to improve with conservative management, an exploratory laparotomy with total abdominal colectomy and end ileostomy was completed to achieve source control.
Laboratory workup
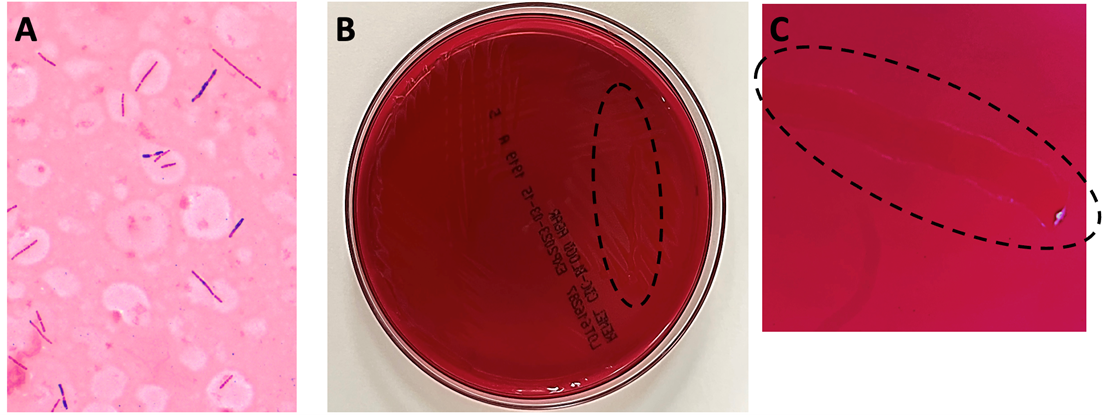
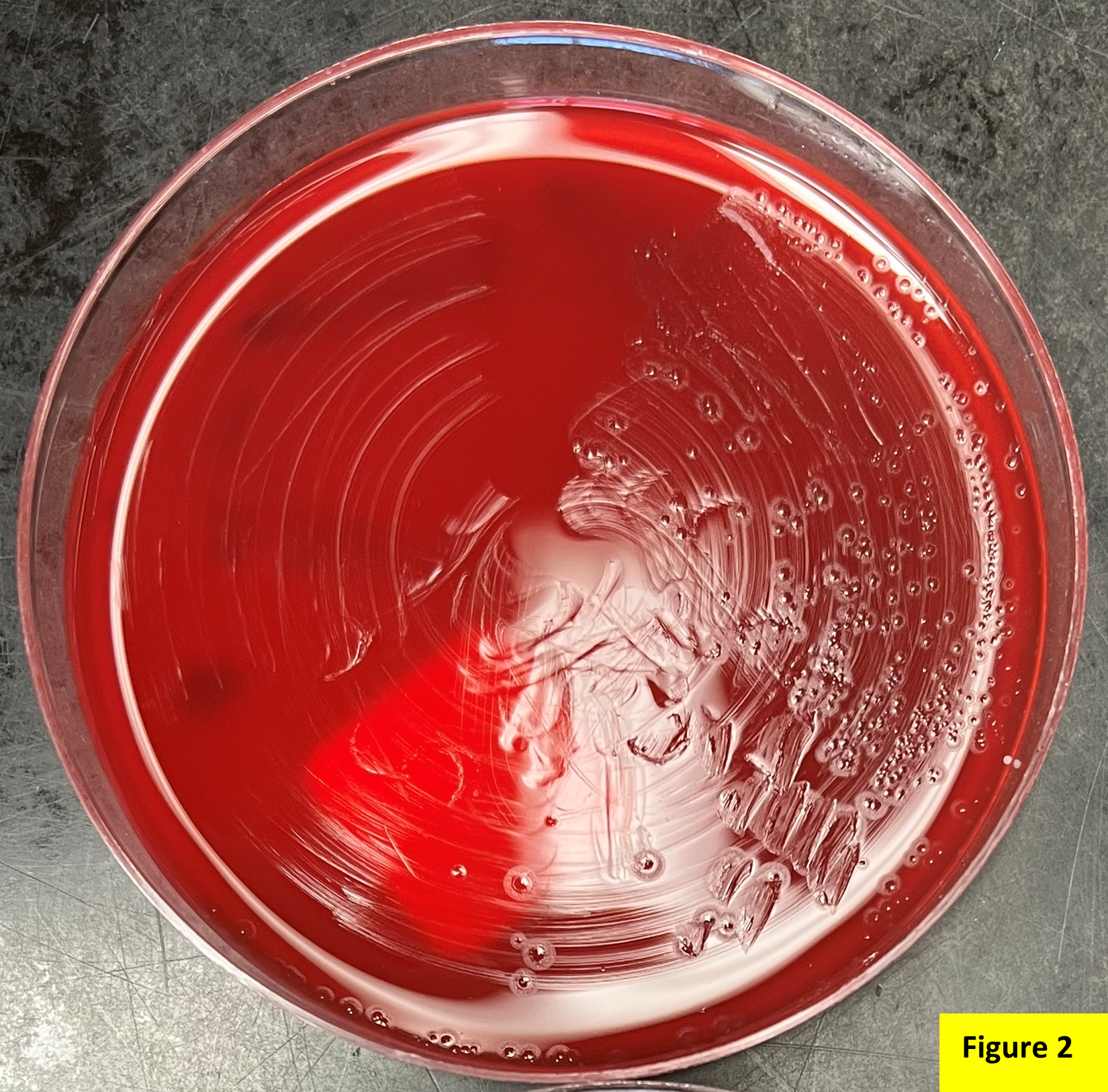
Anaerobic bottles from blood cultures collected at the time of hospital admission flagged positive in under 24 hours. Gram staining from the positive bottle broth revealed large, gram variable bacilli (Image 1A). Multiplex PCR performed on the positive blood culture broth failed to reveal the identity of the organism. After 24 hours, close observation was required to visualize bacterial growth on anaerobic blood culture media, which appeared as a thin, translucent film (Image 1B). To provide better visualization for this case, a loop was utilized to scrape the growth so a path could be observed within the biomass (Images 1B and 1C, dotted lines). The bacterium recovered was definitively identified as Clostridium septicum by MALDI-TOF MS, prompting continued coverage with piperacillin/tazobactam until discharge.
Image 1. A) Representative Gram stain from the positive anaerobic blood culture bottle. Staining reveals large, gram variable rods. Given the size and morphology of the cells, a gram positive organism was suspected. B) Growth of the organism on CDC anaerobic blood agar after 72 hours. A lack of distinct colonies was noted, and the organism grew as a thin film across the surface of the plate which was difficult to visualize. The hatched oval denotes where a loop was pulled across the plate surface to help visualize the bacterial growth. A closer, enhanced image is presented in C.
Discussion
Clostridium septicum is an anaerobic, Gram-positive spore-forming bacillus.1,2 Colony morphology on solid media evolves over time, with a characteristic “medusa head” morphology at under 8 hours, a “sand grain” appearance at approximately 24 hours, and visible swarming after 48 hours (Image 1B and 1C).2 The organism is found in the soil and the gastrointestinal tracts of both humans and animals with the potential to cause a variety of diseases. It is especially problematic as an infectious agent of livestock and other ruminants, poultry, and horses.1 Clinical manifestations of infection with C. septicum in humans includes necrotizing enterocolitis, bacteremia, and clostridial myonecrosis.2 Prompt identification of infection with Clostridium septicum is essential due to the rapidly fatal nature of untreated bacteremia with this organism. The mainstay of treatment is early initiation of antibiotic therapy and aggressive surgical debridement of affected tissue. The drug of choice for medical management is penicillin, although metronidazole and carbapenems may be used in patients with penicillin allergies.
C. perfringens and C. septicum are the two clostridial species most associated with bacteremia in neutropenic patients.5Clostridium septicum bacteremia can allow for the hematogenous dissemination of infection and can be rapidly fatal.3 Infection of the bowels of a susceptible host and compromise to the bowel wall integrity leads to entry of bacteria into the circulation. In severe cases, this in turn can lead to seeding of distal sites with progression to sequelae including clostridial myonecrosis (gas gangrene). While classical traumatic myonecrosis associated with an infected wound becomes contaminated with clostridial spores from the external environment (most commonly C. perfringens), atraumatic (or spontaneous) myonecrosis is associated with C. septicum (among other clostridial species) and results from hematogenous seeding of distal sites during bacteremia. Virulence and tissue necrosis are mediated by a variety of exotoxins produced by the organism,1 with alpha-toxin being the primary virulence determinant.4
Importantly, Clostridium septicum bacteremia is strongly associated with both hematogenous and gastrointestinal cancers. For this reason, detection of this pathogen in the blood may warrant further patient evaluation for potential sources of underlying pathology.2 In this patient’s case, typhlitis and neutropenic enterocolitis were precipitating factors leading to his C. septicum bacteremia as this patient presented without evidence of gastrointestinal malignancy. Following the procedure, the patient stabilized, and his condition continued to improve through recovery. His antibiotics were eventually discontinued, and he was discharged.
References
Alves MLF, Ferreira MRA, Donassolo RA, Rodrigues RR, Conceição FR. Clostridium septicum: A review in the light of alpha-toxin and development of vaccines. Vaccine. 2021;39(35):4949-4956. doi:10.1016/j.vaccine.2021.07.019
Mallozzi MJG, Clark AE. Trusting your gut: Diagnosis and management of clostridium septicum infections. Clinical Microbiology Newsletter. 2016;38(23):187-191. doi:10.1016/j.clinmicnews.2016.11.001
Koransky JR, Stargel MD, Dowell VR Jr. Clostridium septicum bacteremia. Its clinical significance. Am J Med. 1979;66(1):63-66. doi:10.1016/0002-9343(79)90483-2
Kennedy CL, Krejany EO, Young LF, et al. The alpha-toxin of Clostridium septicum is essential for virulence. Mol Microbiol. 2005;57(5):1357-1366. doi:10.1111/j.1365-2958.2005.04774.x
Bennet JE, Dolin R, Blaser MJ, Onderdonk AB, Garrett WS. Diseases Caused by Clostridium. In Mandell, Douglas, and Bennett’s principles and practice of infectious diseases (2nd ed., pp. 2960-2968). Elsevier.
-Amanda Means is a PGY-1 resident in Anatomic and Clinical Pathology at the University of Texas Southwestern Medical Center in Dallas, Texas. Dr. Means did her undergraduate studies at Sam Houston St University in Huntsville, TX and received her medical degree from the University of Texas Health Sciences Center in San Antonio.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
A 13 year old female presented to the emergency department with a painful left thumb swelling. Eight days ago, she picked out a hangnail from the medial side of her left thumb, resulting in a worsening pain and swelling. She went to urgent care five days ago and was prescribed Augmentin with no improvement. Physical examination showed a tender circumferential swelling of the right thumb past the flexion joint, with paronychia extending 1 cm in length with fluctuance extending an additional 0.5 cm. The wound was incised, and the drainage was sent to the microbiology laboratory for culture.
The culture grew Gram negative bacilli after 24 hours of incubation (Figure 1). The culture grew a moderate quantity of small nonhemolytic colonies that showed “pitting” appearance on blood (Figure 2) and chocolate (Figure 3) agar plates. The colonies notably smelled musty/bleachy. There was no growth on MacConkey agar.
Identification by Matrix-Assisted Laser Desorption Ionization – Time of Flight (MALDI-ToF) revealed Eikenella corrodens.
Discussion
Eikenella corrodens is a facultatively anaerobic, gram negative, oxidase positive, catalase negative, nonmotile, non-spore-forming, rod. It belongs to the HACEK group and is in the family Neisseriaceae. It is a part of the normal flora of the mouth and upper respiratory tract.
E. corrodens is an opportunistic pathogen that can lead to various infections including a variety of head and neck infections (ocular, mastoid, submandibular, thyroid), pleuropulmonary infections, skin and soft tissue infections, etc.). It can cause subcutaneous abscesses, cellulitis of soft tissues, and bacteremia in intravenous drugs users. E. corrodens also causes infections of the hand (i.e., ostomyelitis, cellulitis) because of chronic nail biting, human bite, or clenched-fist injury. The bacterium can gain access to the central nervous system by way of periodontal, middle ear, or sinus infections and cause meningitis, brain or spinal abscesses, subdural empyema, and osteomyelitis. In some predisposed individuals, endocarditis and bacteremia can also occur.
Under aerobic conditions, it grows slowly in blood and chocolate agar at 35–37℃ and does not grow on MacConkey Agar. It forms small, convex, round or irregular, gray, and non-hemolytic colonies. Most isolates may “pit” the agar although both pitting and non-pitting strains have similar biochemical characteristics. Most strains produce a musty or bleach-like odor.
E. corrodens is generally sensitive to ampicillin, amoxicillin, second- and third generation cephalosporins, tetracyclines, azithromycin, sulfamethoxazole, and fluoroquinolones. They are resistant to clindamycin, vancomycin, erythromycin, metronidazole, aminoglycosides, and penicillinase-resistant penicillins, with penicillin susceptibility varying from strain to strain. In clinical microbiology laboratories, the routine antimicrobial susceptibility testing for E. corrodens is not usually performed since it is generally responsive to beta-lactams. If necessary, susceptibility testing can be performed following the CLSI guidelines for fastidious organisms.
The disease spectrum of E. corrodens is increasing in complexity, and it is important to study its clinical characteristics for timely diagnosis, and effective treatment.
References
Chapter 9, Color Atlas and Textbook of Diagnostic Microbiology, Seventh Edition.
Li, L, Shi, Y-B, Weng, X-B. Eikenella corrodens infections in human: Reports of six cases and review of literatures. J Clin Lab Anal. 2022; 36:e24230. doi:10.1002/jcla.24230
-Fahad Sheikh is a 2nd year AP/CP pathology resident in the Department of Pathology at Montefiore Medical Center in Bronx, NY.
-Phyu Thwe, Ph.D, D(ABMM), MLS(ASCP)CM is Associate Director of Infectious Disease Testing Laboratory at Montefiore Medical Center, Bronx, NY. She completed her medical and public health microbiology fellowship in University of Texas Medical Branch (UTMB), Galveston, TX. Her interests includes appropriate test utilization, diagnostic stewardship, development of molecular infectious disease testing, and extrapulmonary tuberculosis.
A 47 year old male presented to the emergency department with a two-week history of progressively worsening left-sided flank and abdominal pain with radiation to his back. He also endorsed associated nausea, vomiting, dizziness, lack of appetite, and a 1-month history of intermittent fever, chills, night sweats, cough, and chest pain. Patient history was also notable for travel throughout the Amazon basin in Peru and Colombia, then to Panama where he felt ill while hiking in the rainforest. He also had sustained injuries to his left flank and head while traveling.
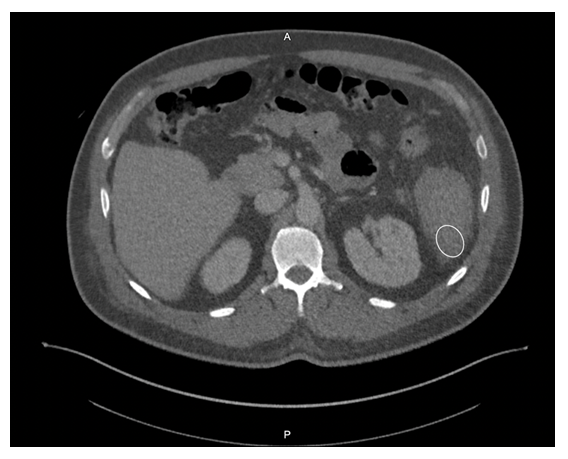
Given his symptomology, further evaluation and management were undertaken. CBC showed a drop in hemoglobin from 10.3 g/dL to 8.5 g/dL, and imaging revealed splenomegaly with a caudally located subcapsular hematoma (Figure 1). Small hemoperitoneum on the pelvis with small non-loculated fluid along the bilateral paracolic gutters was also observed. The patient received two units of packed red blood cells to stabilize his hemoglobin levels.
Laboratory Diagnosis
Malaria smears were ordered given his history travel and evidence of anemia. Plasmodium vivax was identified on thin smear at a parasitemia of 0.1%. The Infectious Disease service was consulted and the patient received IV artesunate followed by oral artemether/lumefantrine and was also started on primaquine for hypnozoite eradication as he was not G6PD deficient. The malaria-associated splenic rupture was well managed with conservative treatment, and no surgical intervention was needed.
Figure 1. Computer Tomography scan of the abdomen reveals a caudally located subcapsular hematoma (white circle).Figure 2. Peripheral blood smears (Giemsa stain, 1000x magnification, oil immersion) from the presented patient. A) An enlarged red blood cell with an irregular membrane containing a ring form (black arrowhead) and a mature trophozoite (white arrowhead) of P. vivax. B) An enlarged red blood cell with dot-like staining and a ring form, consistent with P. vivax (black arrowhead). C) P. vivax gametocyte (black arrowhead) and mature trophozoite (white arrowhead). Infected cells are enlarged and the mature trophozoite expands to nearly fill the red blood cell.
Discussion
Malaria is a severe and sometimes fatal tropical disease caused by Plasmodium sp.The World Health Organization (WHO) estimates 300-500 million humans suffer from malaria each year, of whom >1 million die.1 Five species of Plasmodium cause human malaria: P. falciparum, P. malariae, P. vivax, P. ovale, and P. knowlesi. Patients with malaria initially present with a combination of non-specific symptoms such as fever, chills, headache, and general malaise. Moreover, it can cause various complications, including severe anemia, neurologic defects, nephrotic syndrome, hepatosplenomegaly, and even splenic rupture.
Splenic rupture is an infrequent but life-threatening complication of malaria. Due to a paucity of reported cases, the incidence of pathological splenic rupture in natural vector-transmitted malaria is poorly defined. Additionally, cases of splenic rupture in the setting of malaria are likely to be underreported due to a lack of diagnostic methods, especially in endemic regions.2 One case series determined splenic rupture during malaria was fatal 22% of the collected cases, and it was likely to be the most frequent life-threatening issue of Plasmodium vivax infection reported worldwide.3 Similarly, P. vivax tends to cause more pronounced splenomegaly and a higher incidence of splenic rupture when compared to other Plasmodium species as noted in experimental and clinical studies.2.4 However, the underlying mechanism is incompletely established.
The cause of splenic rupture in malaria infections is thought to be a complication of the macroscopic consequences of different microscopic infiltrative phenomena. Specificities of clotting regulation in the spleen red pulp and acute spleen-specific pooling/unpooling of platelets may lead to increase in intrasplenic tension, making the spleen prone to rupture.3 Although malaria-related splenic rupture is essentially a ‘pathological rupture’ in the absence of overt trauma, minor trauma can also be a triggering event, which possibly contributed to the splenic rupture in this case.
Malaria patients with splenic rupture may present with abdominal pain, hypotension, tachycardia, nausea, and vomiting, which can be difficult to distinguish from signs and symptoms of malaria. Referred left shoulder pain (Kehr sign) caused by diaphragmatic irritation from peri-splenic effusion may also occur. The physical examination can show left upper quadrant or diffuse abdominal tenderness, abdominal rigidity or guarding, and splenomegaly. Radiological studies (i.e., ultrasound or CT scan) play a critical role in diagnosing malaria-associated splenic rupture, and the main findings may include splenic enlargement, splenic tear, subcapsular/intrasplenic hematoma, peri-splenic effusion, and hemoperitoneum. Non-radiological workup by contrast (e.g., decreased hemoglobin/hematocrit level) is generally non-specific.
Management of malaria-associated splenic rupture generally follows the same principles as traumatic injuries. Early diagnosis and appropriate management are essential for a favorable prognosis. It is suggested that conservative treatment can be considered in patients with stable hemodynamics. However, the risk of delayed hemorrhage still exists, which makes strict monitoring crucial. Some data suggest surgical intervention should be considered a first-line treatment if tears involve the splenic hilum.5 Although it may be challenging to decide on surgery versus conservative strategy in clinical practice, there are several definitive surgical indications including signs of peritonitis and unstable hemodynamic status despite aggressive resuscitation. Of note, splenectomy may increase the risk of severe infection caused by encapsulated bacteria and complicatedmalaria; therefore, spleen-preserving procedures should be attempted in selected patients, such as frequent travelers to malarious regions.6
References
Guerra, C.A., et al., The limits and intensity of Plasmodium falciparum transmission: implications for malaria control and elimination worldwide. PLoS Med, 2008. 5(2): p. e38.
Zingman, B.S. and B.L. Viner, Splenic complications in malaria: case report and review. Clin Infect Dis, 1993. 16(2): p. 223-32.
Imbert, P., C. Rapp, and PA Buffet, Pathological rupture of the spleen in malaria: analysis of 55 cases (1958-2008). Travel Med Infect Dis, 2009. 7(3): p. 147-59.
Schmidt, L.H., Plasmodium falciparum and Plasmodium vivax infections in the owl monkey (Aotus trivirgatus). I. The courses of untreated infections. Am J Trop Med Hyg, 1978. 27(4): p. 671-702.
Fuks, D., et al., Spontaneous splenic rupture during a febrile crisis of Plasmodium falciparum malaria. J Chir (Paris), 2005. 142(6): p. 403-5.
Jimenez, B.C., et al., Spontaneous splenic rupture due to Plasmodium vivax in a traveler: case report and review. J Travel Med, 2007. 14(3): p. 188-91.
-Bo Zhang, MD is an AP/CP resident at UT Southwestern Medical Center in Dallas, Texas. He is a first year resident interested in different aspects of surgical pathology.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
A middle-aged patient with a complex past medical history presented to the Emergency Department with the primary complaints of shortness of breath and cough. The patient had recently been admitted for community-acquired pneumonia and discharged with antibiotics 10 days ago. However, the patient continued to have a dry cough, a fever of 102 degrees F, and shortness of breath. On the new admission, they were noted to be hypotensive and labs showed elevated WBC (14.7), lactate of 7.3, proBNP of 852, and procalcitonin of 4.62. Bacterial blood cultures showed no growth. A chest x-ray showed worsening left lower lobe consolidation with extension to the left upper lobe, compared to the x-ray at the previous admission. A bronchoscopy was done and bronchoalveolar lavage (BAL) was submitted for Gram stain, aerobic bacterial culture, and fungal culture. The Gram stain and bacterial culture were negative. However, the fluorochrome stain showed many large budding yeast forms, most suggestive of Blastomyces dermatitidis. Lung tissue sample culture (Image 1), Gram stain (Image 2) and histopathology (Image 3) confirmed the identification as Blastomyces dermatitidis. The patient was expired before the results were released. Gross images of lungs are shown in image 4.
Image 1. Fungal growth on the Sabouraud dextrose plate observed after 2 days. Image 2. Gram stain of left lower lobe of lung tissue sample demonstrating budding yeast. Image 3. GMS and H&E stains of left lower lobe of lung sections demonstrating budding yeast. Image 4. Gross pictures of lungs showing left lower lobe hepatization and miliary pattern consolidation in the right lung.
Discussion
Blastomyces dermatitidis is a dimorphic fungus found in soil and decaying wood. Often found in areas close to a water source such as a lake, river, or stream.1 The fungus is endemic to parts of the United States, including parts of the Appalachian Mountains, the Great Lakes, and the Ohio and Mississippi River Valley.1 Human infection occurs when airborne conidia are inhaled. Blastomycosis (aka Gilchrist’s disease) may cause a broad range of clinical presentations. The most affected organs are the lungs and the skin.2 Osseous, genitourinary, central nervous system (CNS), and disseminated blastomycosis can also be seen, but at a lower frequency.2 Unlike opportunistic fungal pathogens such as H. capsulatum, C. immitis, and C. neoformans, B. dermatitidis no more likely to cause disease in immunocompromised population compared to the non-immunocompromised populatin.3 However, the disease is more severe, with higher morbidity and mortality, and more likely to be disseminated in immunocompromised patients.3
Although growth of fungi took 2 days in our case, Blastomyces is a slow growing fungi in that mycelial forms mature in 14-21 days. In suspicious cases, cultures should be hold up to 8 weeks. Furthermore, Blastomyces should be cultured as soon as possible since it does not survive well in samples. Morphologically, Blastomyces colony appears as a mold, which is white, prickly, and cottony at 25-30 °C However, at 35-37 °C, the colony appears as a yeast, which is tan, wrinkled, and waxy. Microscopically, at 37 °C, Blastomyces appear as round to oval cells with refractile and thick cell walls and measure 8 – 15 uM in diameter. Each yeast cell produces only one, broad-based (4-5 uM), bud. At 25-30 °C, septate hyphae form with short or long conidiophores. Round to pear-shaped conidia attach to the apex, resembling lollipops (Image 5).4
Image 5. Spherical, oval, or pyriform conidia rising from aerial hyphae, mold phase.
History of recent travel to the endemic areas or already living in there usually triggers the suspicion with clinical findings. There are different auxiliary diagnostic modalities for B. dermatitidis including culture, cytology smear, histopathology, urine antigen test, serum antigen test, serum antibody test, and molecular techniques. Serum antibody test exhibits high degree of cross-reactivity with other endemic mycoses.5 Serum and urine antigen testing has a sensitivity of 89 % and specificity of 79 % and it is useful in diagnosis, monitoring treatment, and detecting recurrence.5,6,7 Direct visualization of the distinctive yeast form with broad-based budding on a cytology smear of respiratory secretions or tissue samples using fluorochrome stain is considered as presumptive diagnosis and enough for initiation of antifungal therapy. However, a negative result in smear cannot exclude the diagnosis due to lack of sensitivity. Polymerase chain reaction (PCR) based assays have been developed to detect B. dermatitidis.8 However, although they are promising, utility has not been confirmed and there are no FDA approved assays.8
Only histopathology and culture can provide a definitive diagnosis. Although H&E may be enough in selected cases, periodic acid-Schiff (PAS) and Grocott’s methenamine silver (GMS) stains are useful to highlight the yeast form in tissue sections. In culture, seeing the characteristic morphologic and microscopic appearance is very useful for diagnosis. However, confirmatory testing with chemiluminescent DNA probe may still be necessary.9
Depending on the severity and site of the infection fluconazole, itraconazole, voriconazole, or amphotericin B can be used in treatment.10
References
Castillo CG, Kauffman CA, Miceli MH. Blastomycosis. Infect Dis Clin North Am. 2016;30(1):247-264.
Mazi PB, Rauseo AM, Spec A. Blastomycosis. Infect Dis Clin North Am. 2021;35(2):515-530.
McBride JA, Gauthier GM, Klein BS. Clinical Manifestations and Treatment of Blastomycosis. Clin Chest Med. 2017;38(3):435-449.
Maresca B, Kobayashi GS. Dimorphism in Histoplasma capsulatum and Blastomyces dermatitidis. Contrib Microbiol. 2000;5:201-216.
Wheat LJ. Antigen detection, serology, and molecular diagnosis of invasive mycoses in the immunocompromised host. Transpl Infect Dis. 2006;8(3):128-139.
Mongkolrattanothai K, Peev M, Wheat LJ, Marcinak J. Urine antigen detection of blastomycosis in pediatric patients. Pediatr Infect Dis J. 2006;25(11):1076-1078.
Tarr M, Marcinak J, Mongkolrattanothai K, et al. Blastomyces antigen detection for monitoring progression of blastomycosis in a pregnant adolescent. Infect Dis Obstet Gynecol. 2007;2007:89059.
Bariola JR, Hage CA, Durkin M, et al. Detection of Blastomyces dermatitidis antigen in patients with newly diagnosed blastomycosis. Diagn Microbiol Infect Dis. 2011;69(2):187-191.
Saccente M, Woods GL. Clinical and laboratory update on blastomycosis. Clin Microbiol Rev. 2010;23(2):367-381.
Chapman SW, Dismukes WE, Proia LA, et al. Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(12):1801-1812.
-Kadir Isidan, MS, MD is a pathology resident at University of Chicago (NorthShore). His academic interests include gastrointestinal pathology and cytopathology.
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
A 40-year-old woman with past medical history of polysubstance use disorder (cocaine, IVDU-heroin) presented with shortness of breath on exertion, weight loss, and weakness. Cardiac ultrasound showed aortic valve endocarditis with mild thickening of the aortic valve, vegetation and severe aortic regurgitation without stenosis. The patient was taken to the operating room for aortic valve replacement. A tissue biopsy was sent for surgical pathology workup and microbiology cultures. H&E staining of the right and left coronary cusp and noncoronary cusp and showed focal giant cell reaction, and acute inflamed granulation tissue consistent with vegetation/infective endocarditis. The Gram stain of the tissue specimen revealed gram positive cocci but no bacterial growth was seen. Fungal and mycobacterial cultures were also negative. Broad Range Bacterial PCR and Sequencing (BRBPS) of the heart valve detected Streptococcus mutans.
H&E staining of the heart valve revealed focal giant cell reaction (black arrow), and acute inflamed granulation tissue consistent with vegetation/infective endocarditis (left image). The Gram stain of the tissue specimen revealed gram positive cocci (right image). (H&E diagnosis credits: Dr. Irena Manukyan from George Washington University.)
Discussion
The first step of BRBPS is performing polymerase chain reaction (PCR) targeting the 16S ribosomal RNA (rRNA), a conserved gene across many bacterial species including mycobacteria. If PCR is negative, then sequencing is not performed but if PCR is positive, sequencing such as Sanger sequencing or Next generation sequencing will be followed. Subsequent bioinformatics analysis of the sequencing results will allow identification of the specific bacteria.1,2 In the patient here, the PCR for 16S rRNA was positive and sequencing revealed S. mutans.
S. mutans is part of the viridans-group of Streptococcus and can be identified as a gram positive cocci with growth that is alpha-hemolytic, optochin resistant, and bile insoluble. Viridans group Streptococcus invade the bloodstream following dental treatment or dental procedures and can be associated with high risk for infectious endocarditis in patients with underlying heart disorders. S. mutans first gained medical attention due to its role in dental caries.3S. mutans is considered part of the normal flora of the oropharynx, more specifically the dental plaque, and can form biofilms on the hard surface of the tooth. Bacterial strains that cause endocarditis have been shown to be able to bind to type I, III, and IV collagen, which are major components of the host cardiovascular tissues.4 The bacteria also have virulence factors that can cause strong adhesion to human endothelial cells. Additionally, aggregation and interaction with fibrinogen, platelets, and completement allow this bacteria to successfully cause cardiovascular diseases.5
In infective endocarditis, 20% of the cases are negative by conventional methods such microbiology cultures.6 Several studies have shown that in specimens from patients with endocarditis, 16s rRNA sequencing can correctly detect the organism that was grown in culture but also successfully detect organisms in specimens where there was no growth, allowing clinical teams to accurately treat patients, similar to our case here.7,8 For prosthetic heart valve tissue, the sensitivity of sequencing versus culture is 93% and 35%, respectively. A study describing periprosthetic joint infections using elbow joint fluids showed that sequencing was positive in 47 specimens but 8% of those were negative by culture.10 Additionally, 16s rRNA sequencing has been useful in identifying bacterial tick-borne organisms not typically grown in culture such as Borrelia, Anaplasmsa, Ehrlichia, and Rickettsia].11
The BRBPS test is validated for and ideally be tested on specimens from sterile sources (joint fluid, blood, heart valves, CSF) and ideal specimens are those where bacterial organisms can be visualized using microscopy. Limitations of BRBPS is that this test only detects bacterial organisms and will not detect viruses, fungi, and parasites. False-positive results are possible if the specimen is contaminated with patient flora. False-negative results may occur due to sequence variability affecting how the primers bind, presence of PCR inhibitors, or the quantity of nucleic acid material below the limit of detection. Clinical tests utilizing sequencing approaches may be costly at the moment in time; those who order sequencing tests need to understand the purpose of different sequencing tests so the most appropriate test is ordered. For example, if fungal pathogens are suspected, a sequencing test based on amplifying 28S rRNA or ribosomal ITS genes for the conserved genes found in fungal pathogens is appropriate.12 Such tests where you selectively enrich for specific targets such as 16s or ITS are ‘targeted NGS tests’ which have higher sensitivity for detection of microorganisms in sample types with large amounts of DNA. In comparison, metagenomics is a more agnostic approach and allows for detection of all nucleic acid in the specimen (including both host and microbial reads). While metagenomics can successfully detect pathogens involved in an infection, it can also detect the microbiome present in the same specimen. Hence, the one limitation is the background noise from human nucleic acid and the microflora [13-14. Another type of sequencing is whole genome sequencing where the microbial genome of a particular organism is sequenced and assembled. WGS aids in identification, typing, and determining the microbial susceptibility. WGS is helpful in identifying outbreaks or for epidemiological purposes, but the limitation is that a pure culture is needed. WGS requires a pure culture so this is a limitation for organisms that are non-viable in culture [13-14].
References
Rosey AL, Abachin E, Quesnes G, Cadilhac C, Pejin Z, Glorion C, Berche P, Ferroni A. Development of a broad range 16S rDNA real-time PCR for the diagnosis of septic arthritis in children. J Microbiol Methods. 2007 Jan;68(1):88-93. doi: 10.1016/j.mimet.2006.06.010. Epub 2006 Aug 14. PMID: 16904782.
Loesche WJ. 1986. Role of Streptococcus mutans in human dental decay. Microbiol Rev 50:353–380.
Nomura R, Naka S, Nemoto H, Inagaki S, Taniguchi K, Ooshima T, Nakano K. 2013. Potential involvement of collagen-binding proteins of Streptococcus mutans in infective endocarditis. Oral Dis 19:387–393. doi: 10.1111/odi.12016.
Otsugu, M., Nomoura R., Matayoshi, S., Teramoto, N., Nakanoa, K. Contribution of Streptococcus mutans Strains with Collagen-Binding Proteins in the Presence of Serum to the Pathogenesis of Infective Endocarditis. Infect Immun. 2017 Dec; 85(12): e00401-17.
Baddour LM at al; American Heart Association Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and Stroke Council. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals from the American Heart Association. Circulation. 2015 Oct 13;132(15)
Peeters, B., Herijgers, P., Beuselinck, K., Verhaegen, J., Peetermans, W.E., Herregods, M.-C., Desmet, S., Lagrou, K. Addd diagnostic value and impact on antimicrobial therapy of 16s rRNA PCR and amplicon sequencing on resected heart valves in infective endocarditis: a prospective cohort study. Clinical Microbiology and Infection. 2017 Nov; 23(11): 888.e1-888.e5
Premru, M.M, Zupanc, T.L., Klokocovnik, T., Sabljic, E.R., Cerar, T. Broad-Range 16s rRNA PCR on Heart Valves in Infective Endocarditis. J Heart Valve Dis. 2016 Mar; 25(2):221-22
Miller, R. J.H., Chow, B., Pillai, D., Church, D. Development and evaluation of a novel fast broad-range 16S ribosomal DNA PCR and sequencing assay for diagnosis of bacterial infective endocarditis: multi-year experience in a large Canadian healthcare zone and a literature review. BMC Infect Dis. 2016 April 12:16:146
Flurin, L.; Wolf, M.J.; Greenwood-Quaintance, K.E.; Sanchez-Sotelo, J.; Patel, R. Targeted next generation sequencing for elbow periprosthetic joint infection diagnosis. Diagn. Microbiol. Infect. Dis. 2021, 101, 115448.
Kingry, L.; Sheldon, S.; Oatman, S.; Pritt, B.; Anacker, M.; Bjork, J.; Neitzel, D.; Strain, A.; Berry, J.; Sloan, L.; et al. Targeted Metagenomics for Clinical Detection and Discovery of Bacterial Tick-Borne Pathogens. J. Clin. Microbiol. 2020, 58, e00147-20.
Yeo, S.F.; Wong, B. Current status of nonculture methods for diagnosis of invasive fungal infections. Clin. Microbiol. Rev. 2002, 15, 465–484.
Mitchell SL, Simner PJ. Next-Generation Sequencing in Clinical Microbiology: Are We There Yet? Clin Lab Med. 2019 Sep;39(3):405-418
Hilt, E.E., Ferrieri, P. Next Generation and Other Sequencing Technologies in Diagnostic Microbiology and Infectious Diseases. Genes (Basel). 2022 Aug 31;13(9):1566. doi: 10.3390/genes13091566.
–Rami Abdulbaki, MD is a Pathology Resident (PGY-4) at The George Washington University Hospital. His academic interest includes hematopathology and molecular pathology.
-Maikel Benitez Barzaga, MD is a Pathology Resident (PGY-2) at The George Washington University Hospital. His academic interest include hematology, microbiology, molecular and surgical pathology.
–Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.