Case History:
A 76 year old female presents with a two year history of worsening upper back pain. Imaging revealed compression fractures of the first three thoracic vertebrae (T1-T3). Fine needle aspiration and a core biopsy of the T3 vertebral body were examined in surgical pathology. There was acute and chronic granulomatous inflammation with fungal organisms observed on histologic examination. Surgery for decompression and fusion of C5-T6 vertebrae was performed and tissue was sent for fungal culture.
Potato flake agar shows a tan-brown fungus.Mycosel agar shows beige-white fungal growth.Scotch tape prep shows septate hyphae with unbranched conidiophores and single, terminal, “lollipop” conidia.Silver stain of involved bone with fungal organisms exhibiting broad-based budding.
Laboratory Identification:
The workup revealed a thermally dimorphic fungus with a mold form growing in the laboratory at 25°C and a yeast form present in the surgical pathology specimen. The mold form is moderately slow growing and has septate hyphae with small, round, terminal conidia often described as “lollipops.” The yeast form is large (8-15 microns) with broad based buds and double contoured cell walls. The immune system reacts to the presence of the fungus by forming granulomas and leads to acute and chronic inflammation within the involved tissue. The organisms can occasionally be seen within giant cells in histologic sections. The silver stain, as seen above, highlights the organisms.
Discussion:
The fungus described above exhibits the features of Blastomyces dermatitidis. This organism resides in soil and decaying plant matter and is endemic to eastern North America including the Mississippi and Ohio River Valleys as well as areas surrounding the Great Lakes and St. Lawrence River. The most common primary sites of involvement for Blastomyces are cutaneous and pulmonary. Following a primary infection, the disease can progress to disseminated blastomycosis which involves other sites such as bone.
The primary site of infection in this case is unknown. There was no history of cutaneous ulcers and chest imaging was unremarkable. The patient did have a remote history of bloody sputum production which she had attributed to “dental difficulties” that she was experiencing and has since resolved. This may have been evidence of a primary pulmonary infection preceding the vertebral involvement; however it is difficult to say with certainty.
The classic double contoured cell walls are not evident on the silver stain of the surgical pathology specimen in this case. This may be due to the fact that the bone required decalcification before histologic sections could be taken. The decalcification process may have caused an artifactual loss of the double contour. Despite the fact that this classic finding was not seen, the macroscopic and microscopic morphology is most consistent with Blastomyces.
The patient is being treated with long-term itraconazole and is currently doing well.
-Britni Bryant, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
You know that old adage “you can’t teach an old dog new tricks”? Well, laboratory professionals know that’s wrong—not only do we need to learn new tricks, sometimes we need to learn them in order to help diagnose a patient. In that regard, continuing education sessions—like those at ASCP’s Annual Meeting—can be so helpful to bench technologists. Today, I attended “Team Approach to Diagnosis of Fungal Infections” presented by Dr. Jeannette Guarner, MD, FASCP from Emory University in Atlanta, Georgia. Here are some of the tidbits I learned.
An easy reminder for dimorphic fungus: “mold in the cold, yeast in the beast.”
In direct stains of tissue samples, not all broad-based budding yeast 8 to 15 microns are Blastomyces. It could be Candida or even Aspergillus.
If you’re able, tell the clinician to send to biopsy samples for micro AND pathology—shared specimens tend to introduce error.
Paracoccidioidomycosis is much more common in males (20:1); current thinking is that estrogen is protective.
Chrysosporium (previously Emmonsia): dimorphic yeast currently only seen in South Africa.
Fusarium can grow in blood cultures. (In the tissue, it almost looked like Aspergillus with hyaline septated hyphae.)
Fusarium is generally resistant to antifungals
When seen in tissue samples, hyaline septated hyphae DOES NOT ALWAYS equal Aspergillus.
Black molds are black because of melanin, which protects them from UV rays, heavy metals, free radicals, and high temperatures.
Cryptococcus is the only fungus that has mucin in its cell wall; mucin stain will be positive.
Crypto can sometimes do a broad-based budding.
-Kelly Swails, MT(ASCP), is a laboratory professional, recovering microbiologist, and web editor for Lab Medicine.
Just in time for Halloween: a recently-published study in mBio discusses the 2014 outbreak of Listeria monocytogenes tied to caramel apples. There’s not enough water in caramel and an apple is too acidic to support this bacterium, so how did this outbreak occur? From the study: “Our findings suggest that the 2014 listeriosis outbreak associated with caramel-coated apples can be explained by growth of L. monocytogenes occurring at the interface between two foods which, by themselves, are inhibitory to pathogen growth.”
Case history:
An 18 year old pregnant woman at 16 weeks gestation presented at the emergency department with nausea and vomiting for 3 days. Three days ago she and some of her friends ate chicken at a party. None of her friends experience her symptoms. Laboratory tests revealed urinary tract infection and a stool sample was sent to the microbiology laboratory for culture.
She was prescribed an antibiotic and was released from the ED.
Laboratory identification:
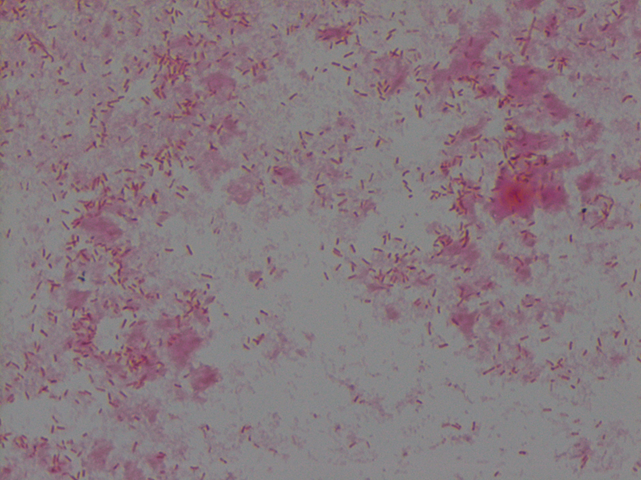
The organism grew well on MacConkey agar, and formed small colorless lactose-negative colonies. Gram stain revealed short gram-negative bacilli and MALDI-ToF confirmed the bacteria as Yersinia enterocolitica.
Non-lactose fermenting, flat colonies on MacConkey agarGram stain of Yersinia enterocolitica reveals Gram-negative bacilli
Discussion: Yersinia enterocolitica is a gram negative, short, non-spore-forming bacillus in the family Enterobacteriaceae. They can exhibit bipolar staining, especially from the primary sample. It is a facultative anaerobe can grow at temperatures ranging from 4-43oC that is motile at room temperature but non-motile at 37oC. The organism grows well on MacConkey agar, and forms small colorless lactose-negative colonies but if the clinical team is suspicious for Yersinia, a selective growth medium is recommended. The most widely used is cefsulodin-irgasin-novobiocin (CIN) agar, which inhibits the growth of competing flora and produces characteristic colony morphology (red color with “bull’s eye” appearance).
The major route of Y. enterocolitica infection is through contaminated foods or water. The primary pathogenic event is colonization of the intestinal tract where most of the pathologic effects and clinical manifestations occur. Temperature and calcium concentration regulate expression of virulence factors that guide the invading Yersinia and allow them to survive and disseminate.
The most common form of disease caused by Y. enterocolitica is gastroenteritis associated with consumption of contaminated food or water, especially raw or undercooked pork such as chitterlings. Disease can range from self-limited gastroenteritis to terminal ileitis and mesenteric lymphadenitis that can be misdiagnosed as appendicitis. Gastrointestinal infections are usually self-limiting and do not merit antimicrobial therapy. However, in immunocompromised hosts and in patients with septicemia or invasive infection, the mortality can be high (approximately 50%).
Kossivi Dantey, M.D. is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
–Christi Wojewoda, MD, is certified by the American Board of Pathology in AP/CP and Medical Microbiology. She is currently the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Antibiotic resistance is a huge concern for microbiologists. In addition to stewardship programs and regulating agricultural use of antibiotics, is it time to re-examine clinical testing paradigms?
A recent study suggests that the typical way microbiologists test for antibiotic susceptibility–meuller-hinton plates and antibiotic disks–might be fallible. When his team tested Salmonella against polymyxin using typical methods, the organism tested sensitive; when the tested the same organism against the same antibiotic using medium that more closely resembled human cells, the organism tested resistant.
Bloomberg Business discusses the paper here. The article is worth your time, even if the info-graphic gives erroneous information (it mentions meuller-hinton broth instead of meuller-hinton agar plates).
An 8 week old female was brought to an outside hospital due to pallor, decreased eating over several days, vomiting, fever, and blue color in the feet. The patient had received her two month vaccinations the day prior to presentation. Her past medical history was significant for being born at 32 weeks gestation, followed by an uneventful 4 week NICU stay. At the outside hospital the patient was in respiratory distress, tachycardic, with pallor. She was intubated and transferred to our institution due to concern for an ALTE (apparent life-threatening event). Blood and CSF specimens were drawn. Upon presentation, the patient had a white blood cell count of 19,600/mm3. Her CSF had 63 nucleated cells/mm3 (30% neutrophils, 49% lymphocytes, 11% monocytes), glucose of 23 mg/dL and protein of 212 mg/dL. Blood and CSF cultures were performed with the following results:
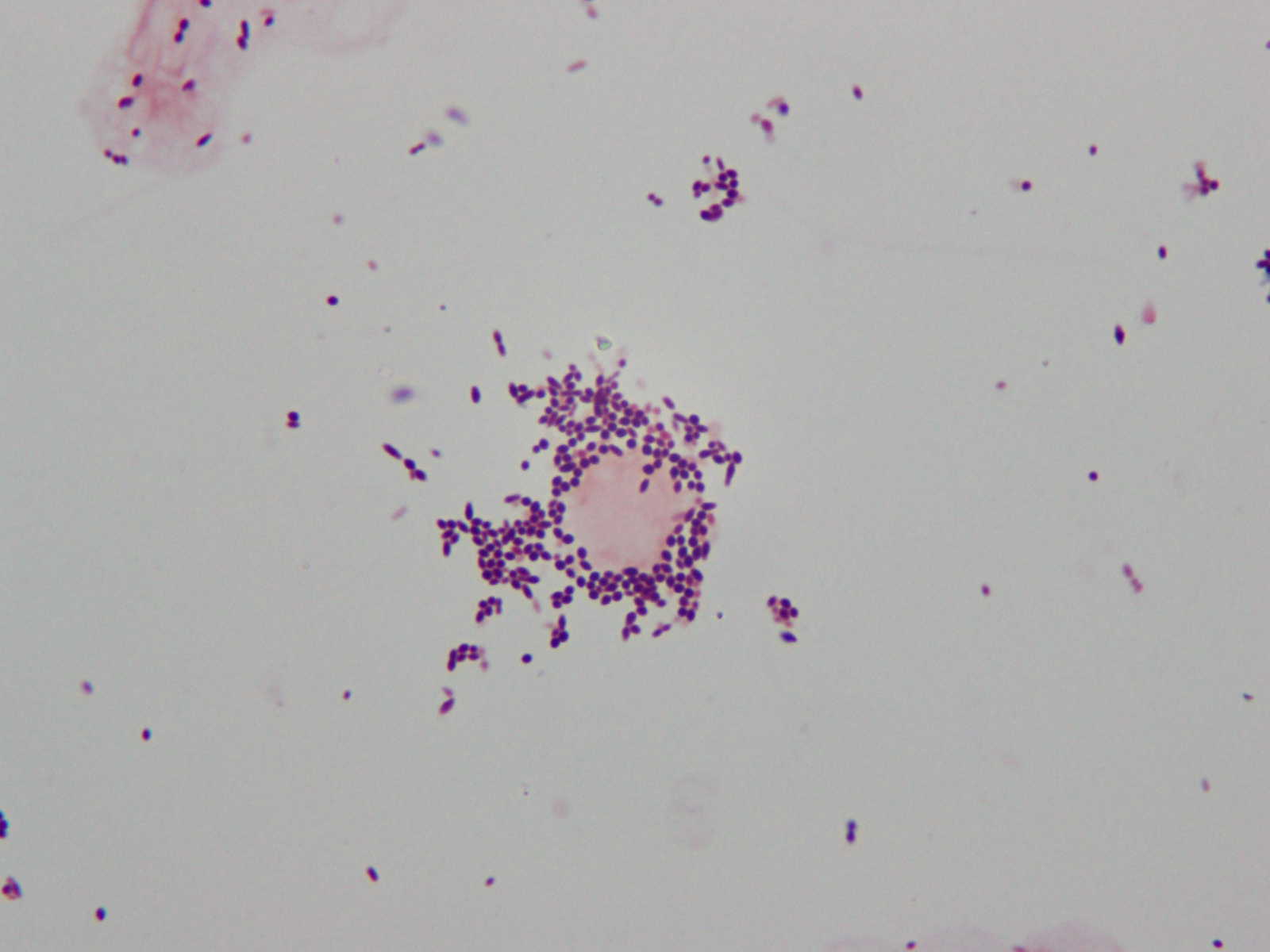
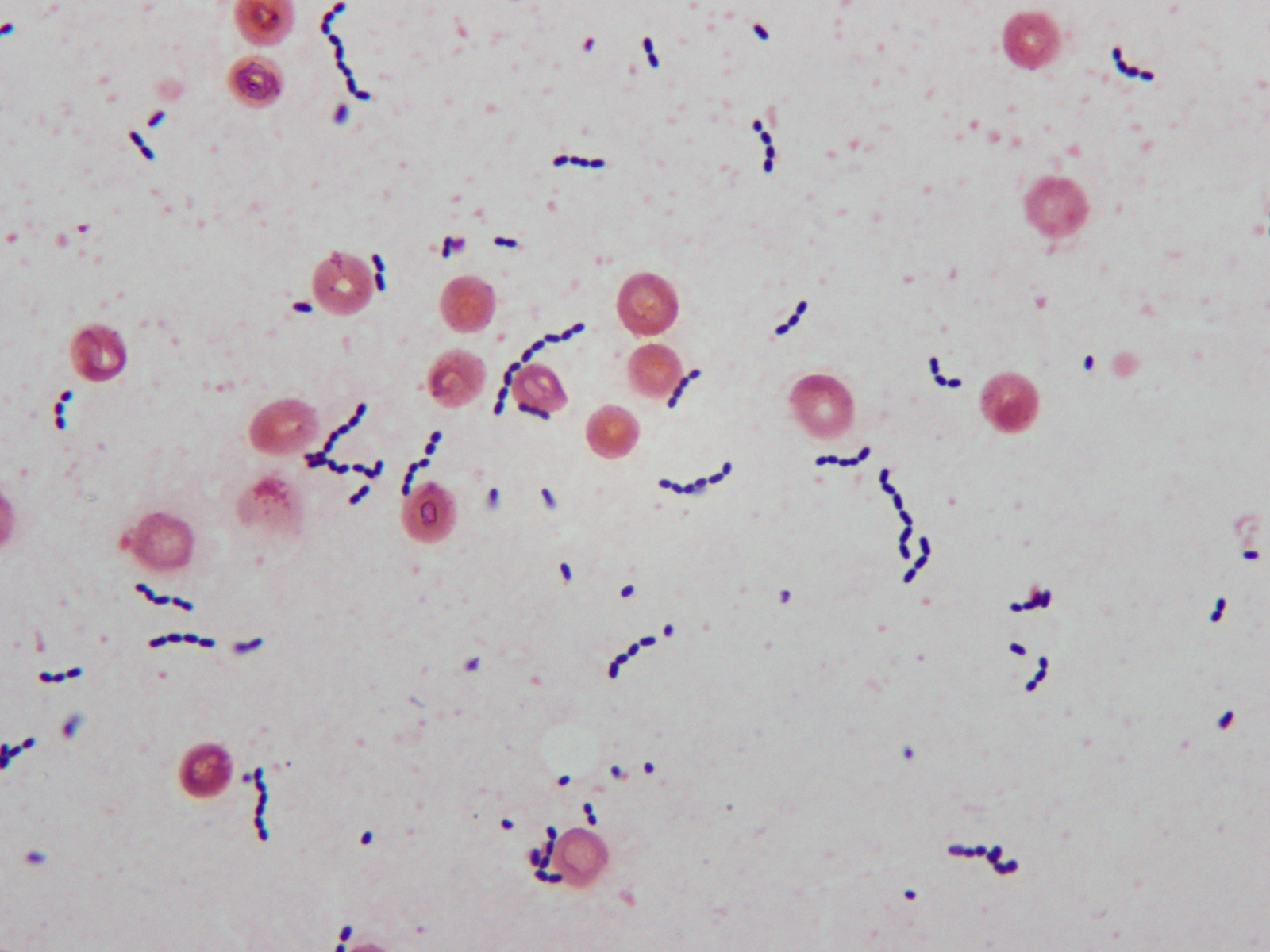
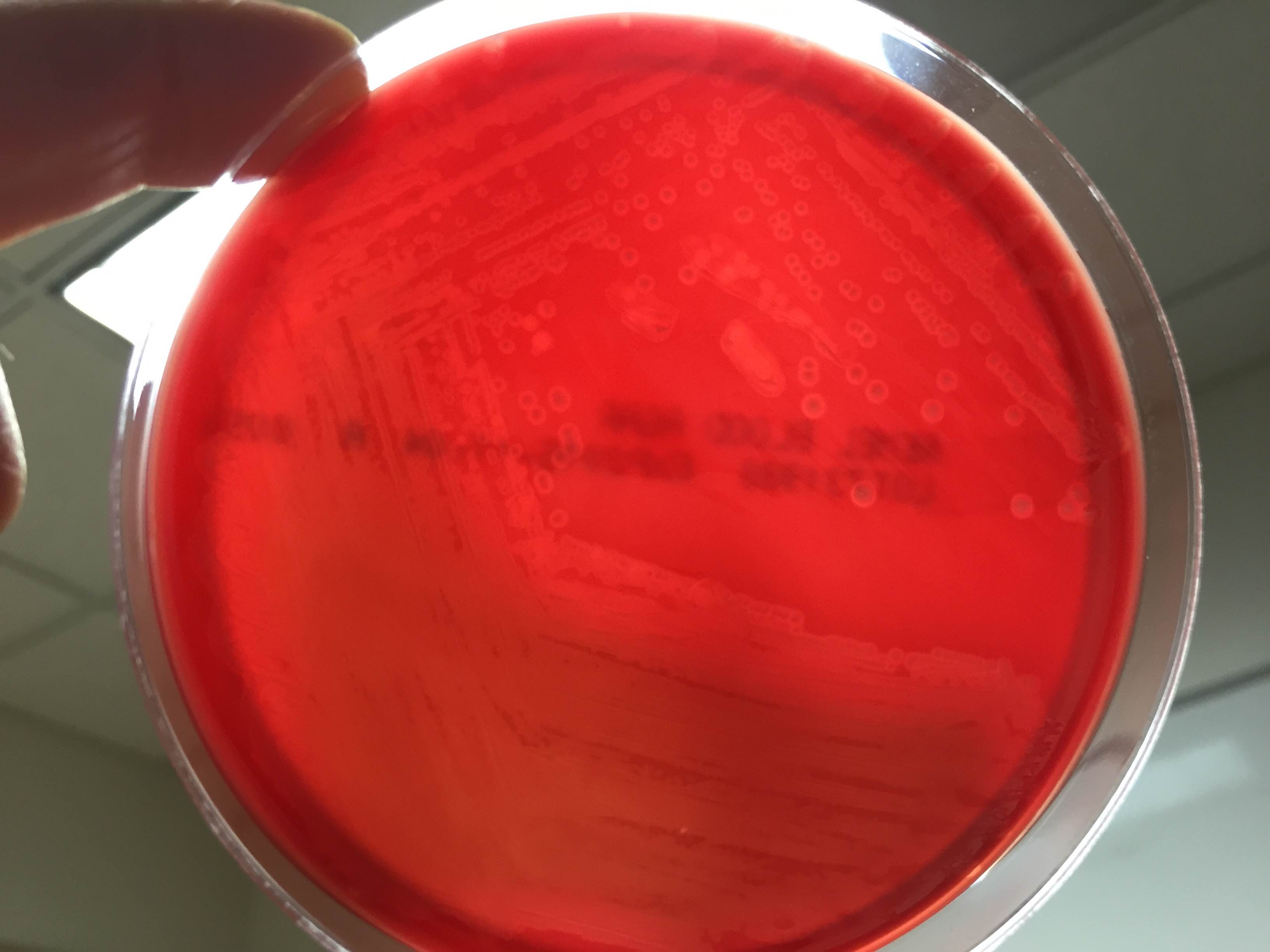
Gram stain of cerebral spinal fluid (CSF) specimen showing Gram positive cocci in singles and pairsGram stain of positive blood culture broth showing Gram positive cocci in chainsSmall zones of beta hemolysis around colonies growing on 5% sheep blood agar
Laboratory Identification
CSF Gram stain was read as many Gram-variable coccobacilli (Image 1) and blood culture Gram stain was resulted as Gram-positive cocci in pairs and chains (Image 2). The Nanosphere Verigene Gram-positive blood culture molecular assay was performed on the positive blood culture broth immediately following Gram staining. CSF and positive blood culture specimens were plated to 5% sheep blood, chocolate, MacConkey, and CNA agars. In >24 hours colonies from both specimens grew a single organism on sheep blood, chocolate, and CNA agars. On blood agar, colonies exhibited a soft zone of b-heomlysis (Image 3). Colony Gram stains showed Gram-positive cocci in chains, catalase testing was negative, and the organism typed in Lancefield antigen group B. Verigene identified the organism directly from the positive blood culture broth as Streptococcus agalactiae (aka Group B Streptococcus or GBS) and MALDI-TOF mass spectrometry confirmed the identification of S. agalactiae.
Discussion
Laboratory Considerations
As our CSF specimen demonstrated, streptococci can be difficult to interpret from specimen Gram stains. Organisms are often are pleomorphic in size and shape and they have a tendency to stain Gram-variable. This lead to the report of Gram-variable coccobacilli on our patient’s CSF culture.
S. agalactiae produces a soft zone of b-heomlysis on sheep blood agar. Unlike Streptococcus pyogenes (aka Group A Streptococcus) which produces a wide zone of b-hemolysis, soft b-hemolysis can often be very subtle, especially with young growth. Soft zones b-hemolysis can best be seen by holding plates up to a light source or my moving a colony out of the way to observe if hemolysis is present underneath. The pattern of S. agalactiae b-hemolysis is very similar to that produced by Listeria monocytogenes. Streptococcal isolates that type as Lancefield Group B, but produce large zones of b-hemolysis can create confusion and are most likely not S. agalactiae, but S. porcinus or S. pseudoporcinus.
Clinical Significance
S. agalactiae is the cause of significant neonatal disease. Early-onset infection presents as systemic infection, respiratory distress, apnea, shock, and pneumonia within the first 24 hours of life (range, 0–6 days). Meningitis is less common in early-onsetS. agalactiae infections, found in just 5-10% of cases. Late-onset disease presents at 3 to 4 weeks of age (range, 7–89 days) as meningitis and/or sepsis with other focal infection. Approximately 50% of survivors of early- or late-onset meningitis have long-term neurologic sequelae.
S. agalactiae colonizes the urogenital or gastrointestinal track of 10-30% of pregnant women. Being born to a S. agalactiae colonized mother is the most significant risk factor for development of disease in neonates. For this reason, women are screened for “Group B Strep” colonization between 35 and 37 weeks of pregnancy. Women found to be colonized receive prophylactic antibiotics immediately prior to delivery to prevent transmission to the child. Since implementation of these practices in 1996, there has been a substantial decline in early-onset S. agalactiae infections. Interestingly, these measures have not affected the incidence of late-onset disease.
Treatment
Until recently S. agalactiae was considered universally susceptible to penicillin. There have now been a few reports of S. agalactiae isolates with increased penicillin MICs due to mutations in the penicillin binding protein Pbp2x. The detection of these isolates is still extremely rare, so much so that S. agalactiae susceptibility testing for penicillin and other b-lactams is not considered necessary at this time. Penicillin and its derivatives are the preferred treatment option.
Patient follow-up
Our patient had a complicated course of late-onset Group B Streptococcal meningitis including multifocal cerebral infarctions and seizures. She was treated with a 28 day course of ampicillin. Blood cultures taken 24 hours after the start of antibiotics were negative and her CSF culture was negative when rechecked 5 days after her presentation. Due to her complicated course, the patient was hospitalized for 4 weeks. Follow-up appointments have shown the patient’s MRI is nearly normal 8 weeks post infection and the patient is doing well, although she is still followed by neurology to assess for long term sequelae.
Our patient’s mother had an unknown Group B Strep carrier status at the time of her birth, as she was born at 32 weeks, which is before routine screening occurs for pregnant women. Either way, the mother’s status would not have affected the patient’s risk for late-onset Group B Streptococcal infection.
References:
Red Book 2015
Journal of Clinical Microbiology, 10th edition
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
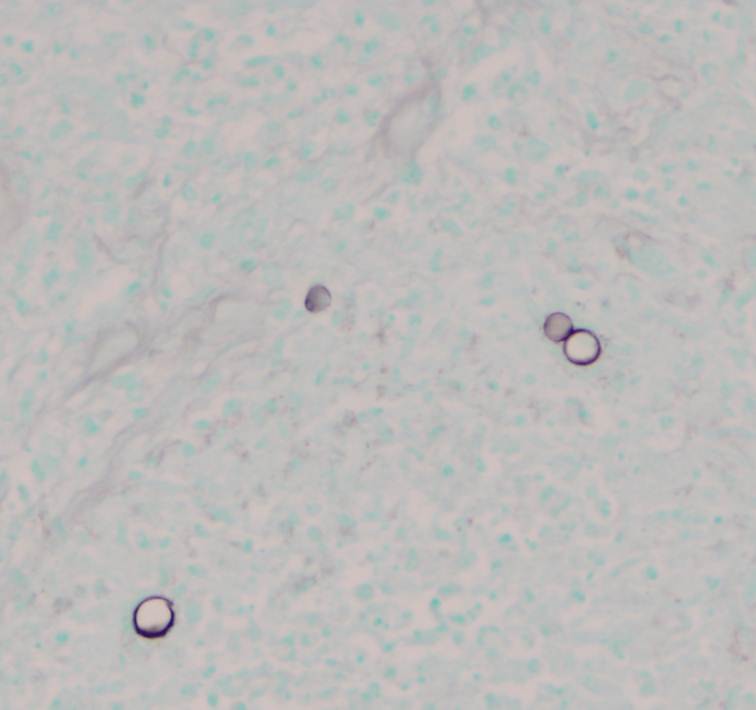
A 32 year old male with a history of HIV presented with a non-productive cough, pleuritic chest pain, and subjective fevers and chills. The patient’s CD4 count was 23 cells/mL; he was not on highly active anti-retroviral therapy (HAART) or prophylaxis for opportunistic infections. A bronchoscopy was performed out of concern for opportunistic infection; a silver stain of bronchoalveolar lavage fluid from the right middle lobe revealed the following.
Laboratory identification:
Pneumocystis jiroveci (P. carinii) was identified based on morphologic examination of the silver stained fluid. The spherical, slightly dented or concave firm-walled cystic form (4-7 mm in diameter) was identified within the foamy alveolar fluid. Flexible-walled trophozoite forms may also be present in pulmonary fluid but are difficult to recognize. The organism may also be identified by a monoclonal antibody microscopic method of detection (highly sensitive but expensive and may have nonspecific staining) or nucleic acid amplification methods. The organism does not grow in routine culture.
Discussion:
Pneumocystis is an opportunistic pathogen with worldwide distribution that has closer homology to fungi than protozoa, which is why the name was changed from P. carinii to P. jiroveci. Its life cycle is not entirely understood, but there are cyst forms, sporozoite forms, and trophozoite forms.
Infection is acquired by inhalation. It is believed that most people are sub-clinically infected during childhood and that the infection is usually well contained by the immune system. During times of immunocompromise, the organism adheres to type I pneumocytes and replicates extracellularly while bathing in alveolar lining fluid causing the alveolar spaces to fill with foamy material. The organism is not susceptible to common antifungal agents and is treated with trimethoprim-sulfamethoxazole.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 51 year old woman with a significant smoking history presented with 8-9 weeks of fever and cough. Shortly after the beginning of her illness, she developed pleuritic left-sided chest pain and hemoptysis. She was treated with amoxicillin and then prednisone without improvement. She had progressively worse pain and hemoptysis as well as fevers and night sweats, with weight loss. A chest x-ray and CT scan showed a left upper lobe mass- like infiltrate suspicious for a carcinoma. She underwent transbronchial fine needle aspiration biopsy of the lesion which showed the following morphology.
Bronchoalveolar lavage fluid (Pap stain).
The specimen was also sent for fungal culture.
Colony morphology on fungal media.Organism morphology with lactophenol cotton blue scotch tape prep.
Laboratory diagnosis:
Blastomyces dermatidis was identified by microscopy and colony morphology. Septate, delicate hyphae with single, circular-to-pyriform condia on short conidiophores (lollipops) were seen on a scotch tape prep. The colonies appeared waxy and wrinkled, with a cream-tan color. Large, thick-walled yeast with buds attached by a broad base, 8-15 um with double-contoured walls, were demonstrated in tissue. Additionally, this patient had a positive urine antigen test for Blastomyces.
Discussion:
Blastomyces’ natural habitat is unknown but the organism is thought to reside in soil or wood, particularly in the Ohio, Mississippi, and Missouri River valley regions. It takes 2-30 days to grow in the lab. The infectious form is the conidia which are transmitted by inhalation. Common sites of infection include skin, lungs, and bone. The typical presentation in an immunocompetent individual is a pulmonary infection with associated acute or chronic suppurative and granulomatous lesions. Blastomyces infection may also cause osteomyelitis, prostatitis, urethritis, CNS infection, and disseminated infection. Immunocompromised patients may present with disseminated infection with involvement of skin, bone, and multiple organs. Infection may be confirmed by exoantigen testing or by nucleic acid probe testing.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
Is $12 million enough to jump start innovation in the fight against antimicrobial resistance? The folks at the British initiative The Longitude Prize hope so. The challenge: create a cheap, fast, and accurate point-of-care analyzer or test kit to rapidly diagnose bacterial infections.
A major hurdle to curbing antimicrobial resistance is diagnostic in nature. Because identification and susceptibility testing can anywhere from two days to several weeks (depending on the causative agent), healthcare providers often need to prescribe antibiotics without knowing this critical information.
The challenge is a daunting one–the test kit would need to identify a broad number of bacterial species and resistance factors. It also needs to be functional all over the world (read: low resource settings).
CLSI has released a new fall webinar schedule. Starting this month, the organization will focus on helping laboratory professionals develop their own individualized quality control plans (IQCPs) and provide them with new ways to deal with antimicrobial susceptibility testing (AST) challenges.
On September 15, 2015, CLSI will host a webinar entitled, Developing Your Laboratory’s IQCP for Antimicrobial Susceptibility Testing. Presented by Susan E. Sharp, PhD, ABMM, FAAM, Director, Regional Microbiology and Molecular Infectious Diseases Laboratories at Kaiser Permanente in Portland, Oregon, USA, and Linda C. Bruno, MA, MT(ASCP), Director, Microbiology and Molecular Pathology Labs at ACL Laboratories in Rosemont, Illinois, USA, this webinar will focus on requirements for IQCP as mandated by the Centers for Medicare & Medicaid Services. It will also focus on the new College of American Pathologists (CAP) requirements for IQCP and how to develop an IQCP for AST.
On October 6, 2015, CLSI will partner with CAP to present Antimicrobial Susceptibility Challenges in regards to the CLSI AST documents and other AST resources that are currently available. Led by Janet A. Hindler, MCLS, MT(ASCP), Sr. Specialist, Clinical Microbiology at UCLA Health System in Los Angeles, California, USA, and Audrey N. Schuetz, MD, MPH, D(ABMM), FCAP, Interim Director, Clinical Microbiology Laboratory; Associate Professor of Pathology and Laboratory Medicine; and Associate Professor of Medicine, Weill Cornell Medical College/NewYork-Presbyterian Hospital from New York, New York, USA, this webinar will cover appropriate agents to report on individual species when isolated from select body sites. There will also be information presented about practical strategies for identifying, confirming, and reporting results for multidrug-resistant bacteria.
Lastly, on November 19, 2015, CLSI will host a webinar called Finding Value in Your AST IQCP: Improving Accuracy and Timeliness of AST Reports. This webinar will focus on what AST results should be confirmed before reporting and will cover processes that can be implemented to identify the most common AST reporting errors. Join A. Beth Prouse, MS, MT(ASCP), Clinical Microbiologist, at Peninsula Regional Medical Center in Salisbury, Maryland, USA, and Janet Hindler as they present on these topics as well as describe ways to improve AST report turnaround time.
Register for these webinars on the CLSI website at www.clsi.org/webinars. Member discounts apply to all CLSI-hosted webinars (September 15 and November 19).