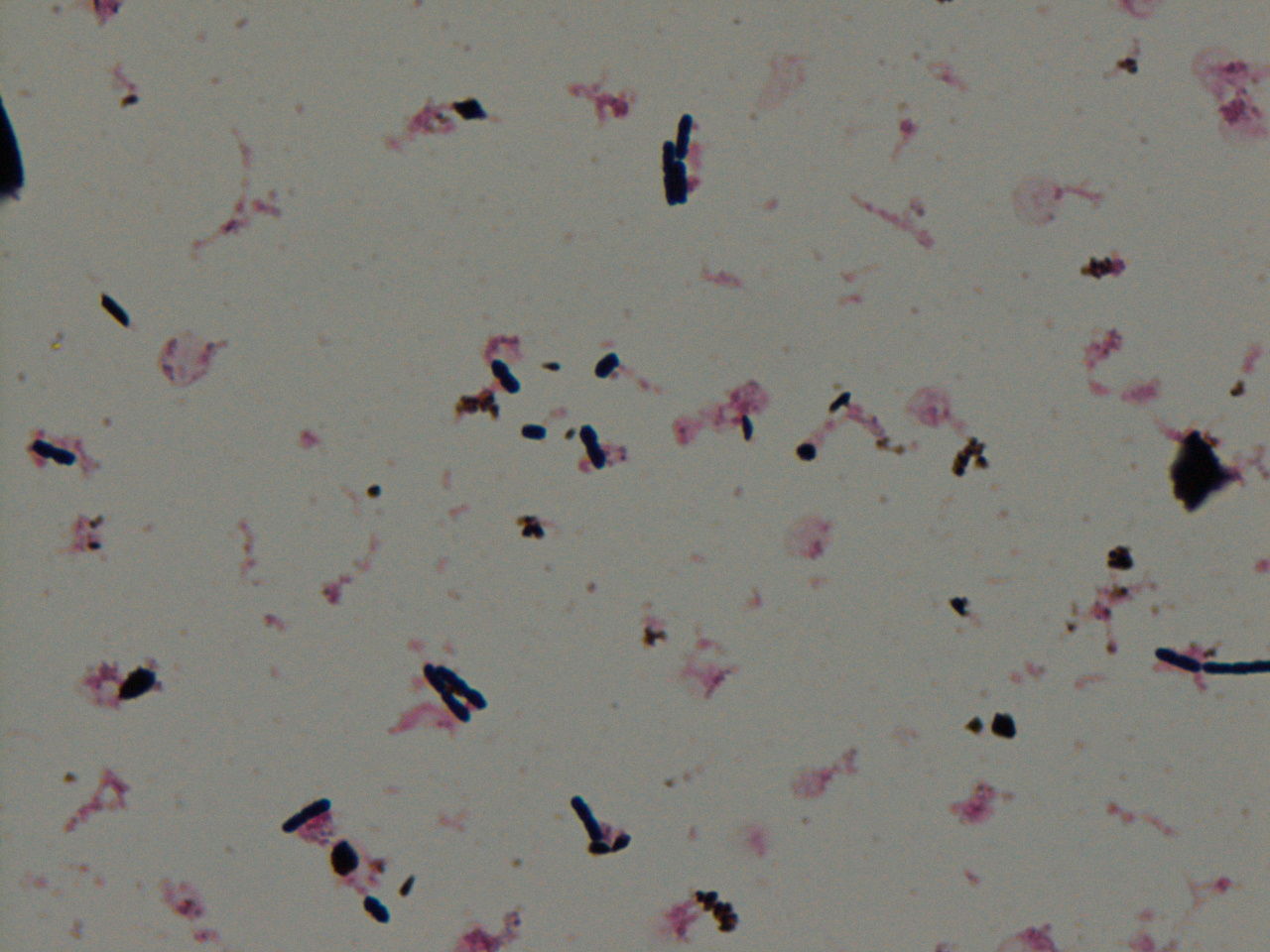
An 80 year old female presented to the emergency department complaining of a productive cough, three episodes of bright red blood stained sputum, persistent night sweats, fever, chills, and weight loss. Chest imaging revealed extensive centrilobular ground glass opacities, multiple pleural based nodules, and a cavitary lesion. The patient was exposed to Mycobacterium tuberculosis as a child when her father was treated for an active infection. Direct smears were negative; respiratory cultures were performed and an AFB culture bottle flagged positive with the following gram stain and culture morphology.
Poor-staining, beaded Gram positive bacilli in clumps and cords.
Laboratory identification:
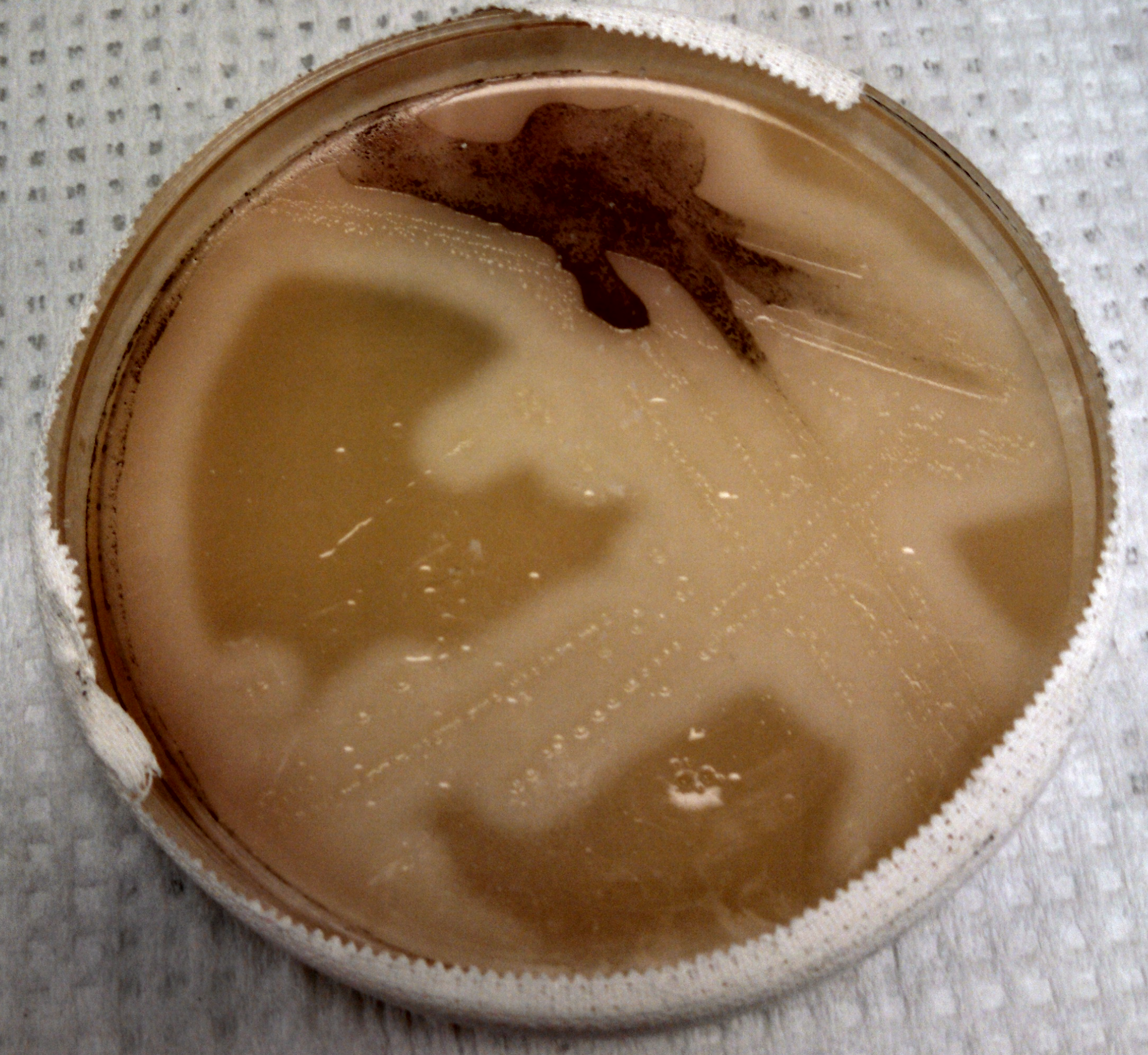
The organism was auramine fluorescent stain positive from the broth. The AFB culture bottle was sub-cultured to agar based medium in addition to Lowenstein-Jensen medium, which yielded buff colored colonies with a dry bread-crumb like appearance, raising concern for Mycobacterium tuberculosis. Species identification was confirmed by DNA probe.
Discussion:
Definitive diagnosis of Mycobacterium tuberculosis is based on microscopy, culture, and/or PCR. The organisms are typically acid fast, straight or slightly curved rods that occur singly or in small clumps in clinical specimens. They may grow as twisted rope-like colonies called serpentine cords in liquid medium and take up to 2-4 weeks to grow in culture. They are obligate aerobes.
TB is transmitted by inhalation of bacilli in contaminated respiratory droplets. In an immunocompetent host, primary, latent, or reactivation pulmonary infection may occur. Reactivation disease and disseminated (military) disease is possible in immunocompromised patients including those with HIV, transplant recipients, and the elderly. TB also causes meningitis, pleurisy, and spinal infections.
The virulence of the organism is likely multifactorial and is believed to be related to its ability to survive within macrophages. It is treated with multi-drug antimicrobial therapy.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
An 11 month old female with no significant past medical history was admitted with a fever of 104 degrees Fahrenheit, nausea and vomiting for 3 days (now resolved), watery diarrhea 4-5 times/day (resolved), and a new onset of acute pharyngitis/bilateral cervical adenitis. ER staff was concerned for a bacterial superinfection. She appeared sick with pale skin, but vital signs were stable, and labs were unremarkable except for an elevated CRP (15.7) and an absolute monocytosis (though no elevation in total WBCs). Exam showed a hyperemic pharynx without exudates, and no lymph nodes larger than 1 cm. A CT neck shows bilateral cervical adenitis, left greater than right, with some suggestion of necrotic nodes, as well as a likely left 3rd or 4th branchial cleft cyst. Blood cultures were drawn, and they turned up positive in a matter of hours, with the gram stain and plate morphology seen below:
Gram stain of positive blood culture broth showing Gram positive cocci in chainsLarge zones of beta-hemolysis around colonies growing on 5% sheep blood agar
Laboratory Identification:
Gram positive cocci in chains were seen, with small, glossy, gray-white, translucent colonies on blood agar having a wide zone of surrounding beta hemolysis. Catalase testing was negative, PYR testing was positive, and latex agglutination testing for Lancefield antigens was positive for Group A. MALDI-TOF confirmed the presumptive identification of Streptococcus pyogenes.
Discussion:
S. pyogenes (aka Group A Streptococcus [GAS]) is a ubiquitous gram positive cocci that causes a wide range of disease in humans. It is the leading cause of acute pharyngitis, particularly in children aged 5-15, although 15-25% of school aged children are asymptomatically colonized. S. pyogenes can also cause cellulitis, impetigo, necrotizing fasciitis, scarlet fever, toxic shock syndrome, otitis media, osteomyelitis, pneumonia, or even rarely meningitis/brain abscess. It additionally causes several serious post-infectious sequelae, particularly in untreated cases, including acute rheumatic fever with potential rheumatic heart disease, and poststreptococcal glomerulonephritis.
S. pyogenes has numerous virulence factors, most importantly the M protein, of which there are nearly 80 variants. M protein binds fibrinogen, inhibits complement binding, and prevents phagocytosis. As it is the major antigenic target of antibodies formed following infection, immunity is conferred only to the infecting strain, and none of the others, which complicates vaccine development efforts. Streptolysin O is responsible for the organism’s b-hemolysis on blood agar, and is also immunogenic, causing elevated Anti-Streptolysin O antibodies (ASO), which can be useful in diagnosing a recent infection, rheumatic fever, or poststreptococcal glomerulonephritis.
GAS pharyngitis is uncommon in children less than 3 years old, as is the bacteremia seen in the patient, which was presumably secondary to the severity of the throat infection. A later CT scan showed an enlarging abscess in the left lateral neck, corresponding to the earlier supposed branchial cleft cyst, despite IV clindamycin which was begun in the ER. Ceftriaxone was added, and later changed to Piperacillin/Tazobactam to complete a seven day course, though future blood cultures were negative. The additional antimicrobial coverage was due to the concern for other infectious microorganisms, as S. pyogenes is universally susceptible to penicillin.
Interestingly, this patient also developed a severe absolute neutropenia, with her ANC dropping from 7,100 at admission to 300 two days later, and then to 60 after two further days. The hematology/oncology service was consulted, and they determined that this likely represented a reaction to the infection rather than a more sinister bone marrow pathology. Several more days into therapy her ANC did begin to recover.
References:
Henningham A, Barnett TC, Maamary PG, Walker MJ. 2012. Pathogenesis of group A streptococcal infections. Discovery medicine 13:329-342.
Cunningham MW. 2000. Pathogenesis of group A streptococcal infections. Clinical microbiology reviews 13:470-511.
Red Book 2015
Journal of Clinical Microbiology, 10th editionCunningham MW. 2000. Pathogenesis of group A streptococcal infections. Clinical microbiology reviews 13:470-511.
-Paul Yell, M.D. is a 2nd year anatomic and clinical pathology resident at the University of Texas Southwestern Medical Center.
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
Do you need to know the percentage of Salmonella Typhi resistant to nalidixic acid in California in 2001? A resource now exists that can give you that answer.
The Centers for Disease Control (CDC) has released a tool called National Antimicrobial Resistance Monitoring System (NARMS) Now: Human Data, and it allows users to access antimicrobial resistance data based on year and geographical region. The interactive site tracks resistance for four bacteria that cause foodborne illness: Salmonella, Shigella, Campylobacter, and E. coli O157.
A 58 year old male with a history of pica presented to the emergency room complaining of bilious, non-bloody emesis associated with right upper quadrant pain, fatigue, decreased oral intake, and fevers. Initial labs revealed a lactate of 7.4, a white blood cell count of 22K, alkaline phosphatase 456, AST 373, ALT 444, total bilirubin 5.8, and a troponin of 3.4. Imaging showed a distended, gangrenous gallbladder with compression of the biliary system. Aerobic and anaerobic blood cultures were drawn and the anaerobic culture flagged positive at 20 hours with the following gram stain and colony morphology.
Large Gram-positive boxcar shaped bacilli.Schaedler plate showing double zone of beta hemolysis.Opacification of egg yolk agar around bacterial colonies.
Laboratory identification:
Clostridium perfringens was suspected due to the presence of large gram-positive boxcar shaped bacteria on the gram stain and obligate anaerobic growth with a double zone of hemolysis on the Schaedler plate. Opacification of the egg yolk agar demonstrated that the organism was lecithinase positive which is another characteristic of C. perfringens. Identification of the organism was confirmed by mass spectrometry.
Discussion:
Clostridium perfringens grows on the anaerobic blood agar plate as small gray to gray-yellow colonies with a glossy, dome- shaped appearance with a double zone of beta hemolysis. The organism is an obligate anaerobe and therefore the aerotolerance test is negative. Its biochemical characteristics including the following: lecithinase positive, lipase negative, and catalase negative.
C. perfringens is encountered in a number of clinical settings including wound infections, gas gangrene, bacteremia, septicemia, and food borne illness. The organism has a number of virulence factors including exotoxins and an enterotoxin. Although there are reports of resistance, penicillin is still recommended therapy in many cases.
C. perfringens is found in the biliary system and is associated with gangrenous cholecystitis.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 51 year old man with a medical history of liver abnormalities and long standing alcohol abuse presented with generalized weakness, hypoxemic respiratory failure, sputum production, significant hyperbilirubinemia, macrocytic anemia, and laboratory tests consistent with DIC. Chest X ray revealed a bronchopneumonia pattern. Sputum samples were sent for culture and blood cultures were obtained. Urine antigen legionella test was positive for Legionella pneumophila serogroup 1. The sputum was then plated on buffered charcoal yeast extract (BCYE) agar.
Laboratory identification:
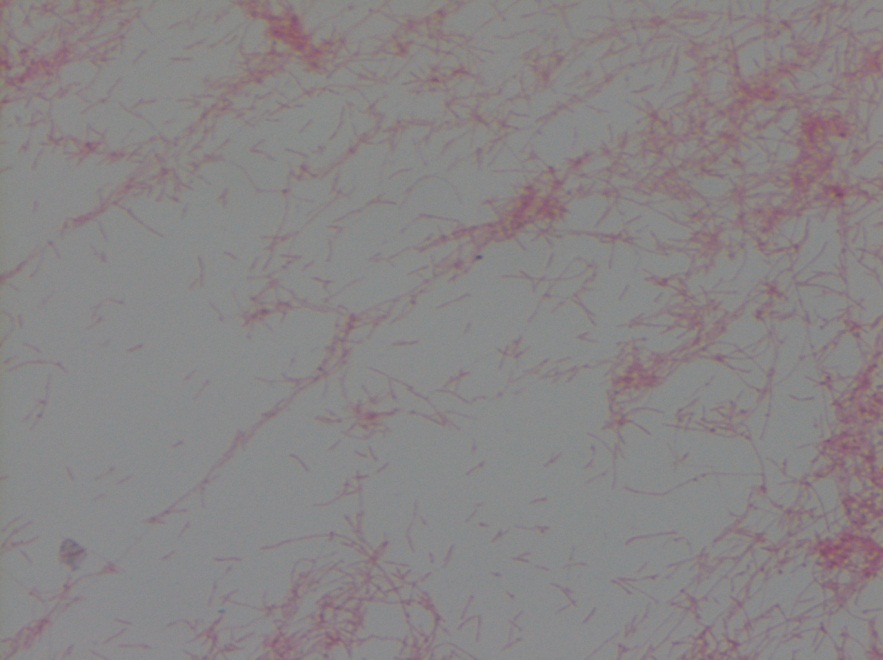
Gram stain of colonies growing on BCYE revealed thin short to filamentous rod shaped organisms. The definitive diagnosis of Legionella pneumophila was made by isolating the organism on BCYE with confirmation on the MALDI-ToF. Colonies were speckled blue and
Legionella on BCYE agar plateGram negative, thin, short-to-filamentous rod shaped organisms
Discussion:
Legionella pneumophila was first identified and recognized during the outbreak that occurred during the American Legion Convention in Philadelphia in 1976. There are over 40 species of Legionella and 18 of those are human pathogens. Among those, L. pneumophila is an important cause of nosocomial and community-acquired pneumonia (CAP) and should be considered in the differential diagnosis in any patient who presents with pneumonia. Two clinical syndromes caused by this microorganism are: Legionnaires’ disease and Pontiac fever (acute, febrile, self-limited illness).
L. pneumophila is a thin faintly staining short to filamentous gram negative rod. Legionella is a fastidious organism and does not grow on standard media. Buffered charcoal yeast extract (BCYE) agar is the primary medium used for its isolation and it is the gold standard for its diagnosis although testing for the antigen in urine is more commonly performed. The urinary antigen assay only detects L. pneumophila serogroup 1 which cause 95-98% of community acquired Legionnaires’ disease.
The microorganism is found in natural water supplies and soil. It is also found in recirculating and water supply systems, where it breeds rapidly in favorable conditions (temperature of 35°C, range 25-45, stagnant water and water containing organic debris which can provide nutrients for growth). Macrolides (azithromycin or clarithromycin) or fluoroquinolones (levofloxacin or moxifloxacin) are the standard antibiotic drugs used to treat Legionnaires’ disease in humans.
Kossivi Dantey, M.D. is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.
–Christi Wojewoda, MD, is certified by the American Board of Pathology in AP/CP and Medical Microbiology. She is currently the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
In this podcast, Dr. Lori Racsa discusses the laboratory identification of this amoeba. While most microbiology techs are unlikely to encounter a case, it’s best to be prepared.
A 5 year old boy who recently immigrated to the United States from Africa presented to his primary care physician with several rough, hypopigmented skin lesions and some hair loss on the scalp. The rash was treated with topical antifungal medication. The patient was treated with griseofulvin for tinea capitis and initially responded well. Six months later he developed pruritic macules on his body, for which clotrimazole was prescribed. The patient’s scalp at that time showed few lesions concerning for recalcitrant tinea capitis. He was prescribed weekly fluconazole and topical clotrimazole. Fungal cultures grew an organism with the following scotch tape prep and colony morphology.
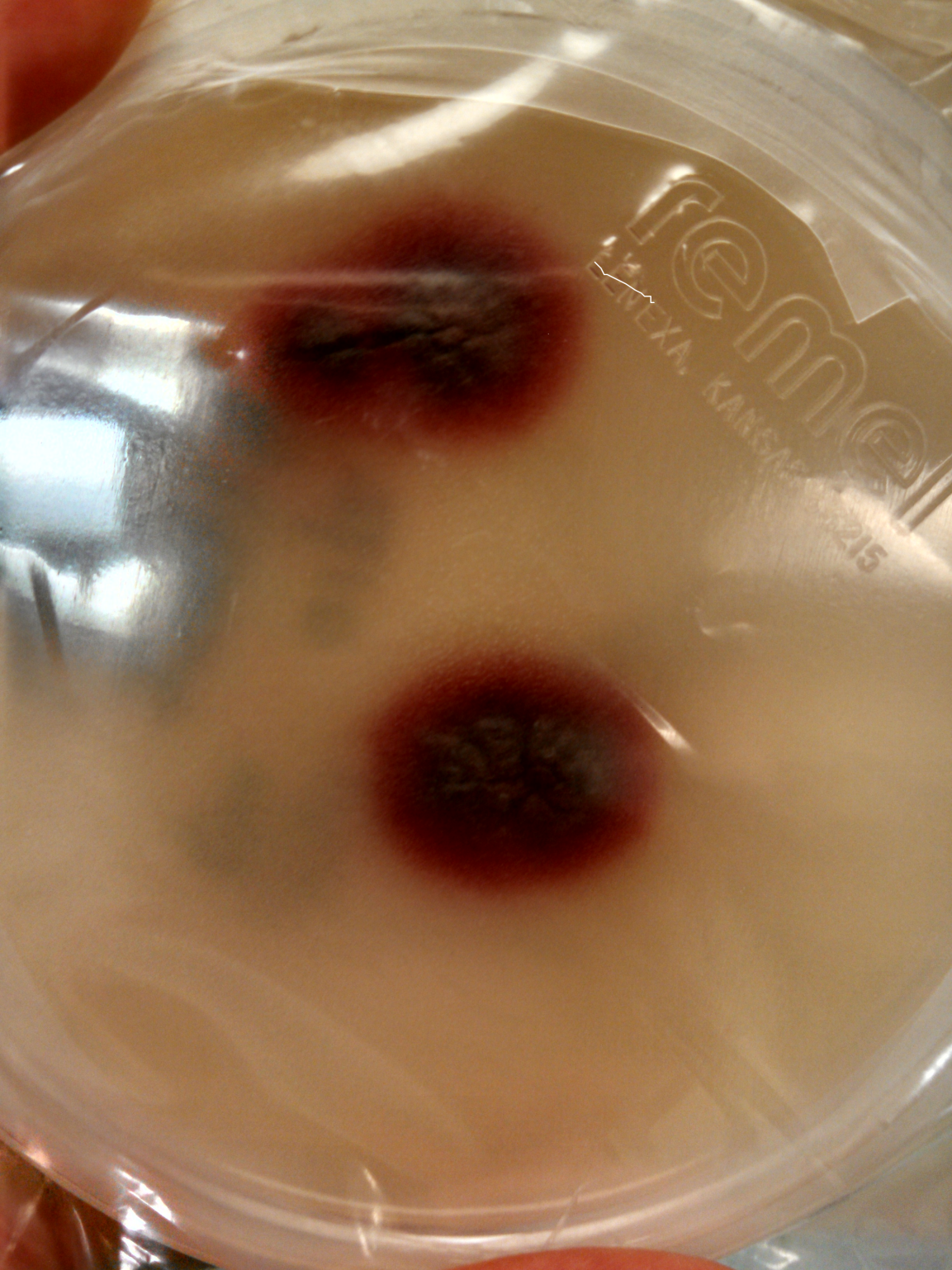
Lactophenol analine blue tape preparation.Colony morphology with deep purple red pigmentation.
Laboratory identification:
The scotch tape prep showed branched, tortuous hyphae and chlamydoconidia in chains but no microconidia or macroconidia were present. The colonies took over two weeks to grow and were initially cream-colored but later developed a port wine to deep violet color. Based on this information Trichophyton violaceum, Trichophyton rubrum, and Trichophyton soudanense were on the differential diagnosis. The specimen was sent to a referral lab for definitive speciation. The referral lab identified the organism as Trichophyton violaceum by MALDI-ToF. The organism was also sequenced for confirmation.
Discussion:
Trichophyton violaceum is a dermatophyte that can be recovered from hair, skin, and nails. The organism requires 14-18 days to grow. Its growth is enhanced by media containing thiamine, which helps differentiate it from other species within the Trichophyton genus. Infection typically causes “black dot” tinea capitis, tinea corporis, and onychomycosis. Infections with this particular Trichophyton species are seen primarily in persons living in Mediterranean region, the Middle East, and Africa. It is treated with oral griseofulvin.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
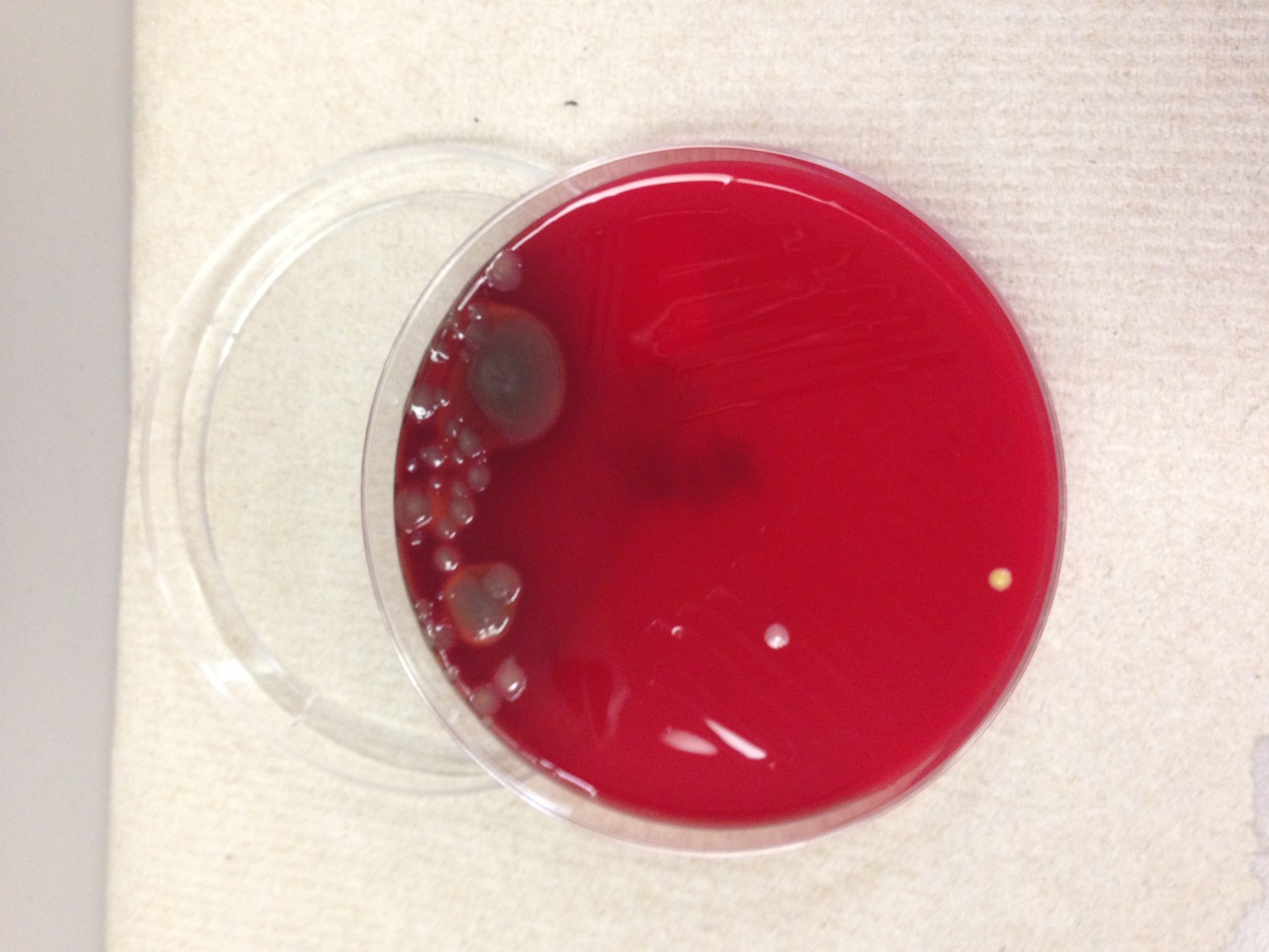
A 22 year old female with no significant past medical history presented with a fever, joint pain and a petechial rash. She endorsed having cold/flu symptoms for two weeks prior. The patient was admitted to the hospital where blood cultures were drawn and antibiotics were initiated. One set of blood cultures from the patient flagged positive at 14 hours of incubation with the following gram stain and colony morphology.
Gram stain showing Gram negative diplococci.Chocolate agar plate with small gray, slightly mucoid colonies. Photo courtesy of pixgood.com
Laboratory identification:
The patient’s blood was cultured on aerobic blood agar and chocolate agar plates. The gram stain revealed gram negative diplococci. Medium sized, round, gray to white, slightly mucoid colonies grew on blood and chocolate agars. The organism was definitively identified as Neisseria meningitidis by VITEK-MS. Prior to adoption of mass spectrometry, biochemical tests were performed for further characterization of the organism. Neisseria meningitidis is catalase positive, ferments glucose and maltose but not lactose, is oxidase positive, and does not reduce nitrate.
Discussion:
Neisseria meningitidis asymptomatically colonizes the oropharynx and nasopharynx of humans. It is transmitted by person-to-person spread of contaminated respiratory droplets. Infection causes a spectrum of disease including life-threatening meningitis. Bacteremia causes the characteristic petechial rash, thrombocytopenia, DIC, and shock. The organism may also cause conjunctivitis, pneumonia, and sinusitis. Its virulence factors include surface structures to facilitate attachment to and invasion of epithelial cells. Once the organism gains access to the vascular system, its survival is mediated by the polysaccharide capsule. Endotoxin release mediates many of the systemic manifestations of infection such as shock.
The differential diagnosis for this organism based on the gram stain and colony morphology includes Neisseria gonorrhoeae and Moraxella species. Different Neisseria species can be identified by the sugars they are able to ferment. For example, N. gonorrhoeae ferments only glucose, but N. meningitidis ferments both glucose and maltose.
There is a vaccine that is available for N. meningitidis that includes serogroups A, C, W-135, and Y. There are 12 different serogroups that can be distinguished based on the polysaccharide capsule. Our patient had been fully vaccinated. The isolate was sent to the state public health lab and it was reported back as non-typable and was sent to the CDC.
Treatment of N. meningitidis consists of supportive therapy for shock plus antimicrobial therapy with penicillin, ceftriaxone, or cefotaxime.
***Rare, fatal cases of meningococcal disease have been reported in laboratory staff. Any potential N. meningitidis should be worked with under a class II biological safety cabinet.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 51 year old male with a history of recent left knee arthroscopy presented with increasing joint pain, swelling, and reduced range of motion accompanied by subjective fevers. He was receiving physical therapy and admitted to soaking the knee in a hot tub on two occasions after the therapy sessions. An aspirate of synovial fluid obtained at the clinic showed the following colony morphology and Gram stain:
Spready, rough, bluish-green colonies on blood agar.Gram stain of the predominant colonies showing gram negative bacilli
Laboratory identification:
Pseudomonas aeruginosa is a non-spore forming, non-encapsulate, motile gram-negative bacillus. The bacteria typically form characteristic colonies with a metallic sheen and have a green-blue appearance due to production of soluble blue phenazine pigment (pyocyanin) and yellow-green pigment fluorescein (or pyoverdin). The organisms classically emit a grape-like odor in culture. They are oxidase positive. Lab diagnosis is based on colony morphology and the organism’s biochemical characteristics. P. aeruginosa is also the only clinically significant fluorescent pseudomonad that grows at 42oC. In our laboratory, the isolate was identified on the MALDI-TOF.
Discussion:
P. aeruginosa has been documented to infect any external site or organ. Community acquired infections are associated with otitis media, skin ulcers, corneal infection, and rashes secondary to contaminated hot tub water which is consistent with our patient’s history. Hospital acquired infections are typically related to catheters, bedsores, burns, and eye infections. People with cystic fibrosis are particularly susceptible to infection with this organism although asymptomatic colonization in these patients is also possible. Patients with extensive burns are also at risk for infection with Pseudomonas. Rarely, a septicemic infection characterized by black necrotic skin lesions known as ecthyma gangrenosum may happen.
The organism has two important virulence factors for pathogenesis- exotoxin A and exoenzyme S. It also produces various cytotoxic substances, all of which contribute to the local tissue destruction.
Pseudomonas infections can be treated with aminoglycosides, beta lactam, and fluoroquinolone antibiotics.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
A 92 year old female nursing home resident presented to her primary care physician with an itchy rash between her fingers and at her waist. A skin scrape revealed the following:
Sarcoptes scabiei (the itch mite) from skin scraping.
Laboratory identification:
It is critical that an appropriate specimen is collected for identification of the organism. A fresh unopened papule on the skin should be selected for skin scraping. A scalpel coated in mineral oil should be used to vigorously scrape the papule and transfer the scrapings to a glass slide. A well collected skin scraping draws blood.
Female mites are 330-450 microns long; males are slightly smaller at 200-240. The eggs are thin shelled and approximately 150 x 100 microns in size. It is also possible to see fecal pellets in scrape specimens.
Discussion:
Sarcoptes scabiei is transmitted by direct contact. The gravid female mite burrows into the epidermis leaving behind a trail of up to 40 eggs. The burrowing process is enhanced by the presence of suckers and specialized cutting surfaces on the organism. The larvae hatch in 3-4 days, leave the burrow, and reach adulthood in hair follicles. The typical patient presentation is intense pruritis, often in folds of skin, with possible secondary bacterial infection due to itching and excoriation.
Scabies is treated with aqueous solutions of malathion or permethrin.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.