Author: Lablogatory
The Aftermath of Ebola
The Ebola outbreak may no longer make front page news in the United States and Liberia may have been declared Ebola free in May, but the consequences of the outbreak are still ever present, and will be for years to come.
The first reported Ebola case was in December 2013 in Guinea. By June of 2014 the outbreak had rapidly spread and the rest of the world was taking note. In May 2015 Liberia was declared Ebola free. Currently, the situation in Guinea and Sierra Leone is improving and each country is now able (from a health care standpoint) to isolate and treat current patients. However, new cases are still being reported in both countries so continued vigilance is paramount.
As the disease itself abates and it is possible to see the light at the end of the tunnel, it is clear that Ebola may be (nearly) gone, but its effects will linger for decades and it has left devastation in its wake.
The CDC estimates that, in the hardest hit countries of Guinea, Liberia, and Sierra Leone, the death toll from Ebola cases is: Guinea: 2,509, Liberia: 4,806, Sierra Leone: 3,947. The total number of cases is hard to track but estimates of total cases, including those that are suspected, probable, and confirmed are as high as 3,784 in Guinea, 10,666 in Liberia, and 13,241 in Sierra Leone (numbers are as of July 17, 2015).
The socio economic consequences of the outbreak are numerous. Much of the day-to-day workings of the economy ground to a halt as people stayed home or fled jobs in factories, mines, and fields. Panicked investors fled as the disease began to spread. Disruption during the agricultural season caused diminished agricultural yields which had both economic consequences and resulted in severe food insecurity across the region. Internal and regional trade were dramatically affected due to boarder closures and movement restrictions to help staunch the transmission of the disease. Those who survived the outbreak are now left to pick of the pieces of their daily lives and learn to live without loved ones. Parents were left without children, children were left without parents. The courage it would take to find jobs, housing, a support system after watching loved ones die (and possibly being sick oneself) is hard to fathom.
A portion of the damage left in Ebola’s wake includes health care systems and infrastructure. Already weak to begin with, Ebola wreaked havoc on the human and infrastructural health care resources in all three countries. The Economist reports that an estimated 509 health care workers died in Guinea, Liberia, and Sierra Leone. This is an enormous loss of human resources in countries where, before the outbreak, the average doctor to patient ratio was less than 10 doctors per 100,000 people. Looking to the future, one of the biggest health care concerns is the number of children who went unvaccinated during the height of the outbreak. Because of this, vaccine-preventable diseases, such as measles and polio, will contribute, indirectly, to Ebola’s death toll.
To end on a positive note, however, the local and international communities are now left with an opportunity: to remake the systems better than they were before. In many places physical infrastructure, human resources, and other necessary systems will be starting anew. With the right expertise and resources, using best practices and with cooperation among international agencies, private donors, and local governments, among others, health care can be built stronger than before with an eye toward preventing such devastating outbreaks in the future and caring for the day-to-day health needs of the local populations.
For further reading:
- http://www.washingtonpost.com/sf/world/2015/03/23/ebola-aftermath/
- http://www.doctorswithoutborders.org/article/%E2%80%9Cmy-life-torn-apart%E2%80%9D-living-aftermath-ebola
- https://publichealthwatch.wordpress.com/2015/03/12/ebolas-aftermath-a-devastating-measles-outbreak-threatens-west-africa/
- http://foreignpolicy.com/2015/04/27/the-next-victims-of-ebola-measles-polio/
- http://www.wsj.com/articles/africa-struggles-to-rebuild-its-ravaged-health-care-system-1433457230

-Marie Levy spent over five years working at American Society for Clinical Pathology in the Global Outreach department.
Markers of Inflammation
I thought today I’d do a little discussion related to two of the more non-specific, questionably useful tests that we have in the laboratory test arsenal, C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), and their use as markers of inflammation. I’ve left out procalcitonin on purpose since I’ve posted about that inflammatory marker previously. And I won’t discuss hs-CRP and its use in cardiovascular disease risk assessment.
CRP and ESR are referred to as inflammatory markers because both rise when inflammation is present. However neither marker provides much more information other than the presence of inflammation. That leads to the questions: how are these tests useful, and why do we need both?
Good questions! First though, what exactly are these markers? Both of these markers will increase in inflammation, infection and tissue destruction, but at different speeds and to different degrees. CRP is a protein and an acute phase reactant. It is produced by the liver and released in response to inflammatory cytokines, usually within hours of a tissue injury, an infection, or any other cause of inflammation. ESR on the other hand isn’t any kind of analyte at all, but rather a measure of the ability of the red cells to settle out in a blood sample. This settling is affected by the fibrinogen and globulin concentration in the blood as well as by the red cell concentration and how normal the red cells are. Thus besides inflammation, things like anemia, polycythemia and sickle cell disease also will affect an ESR. ESR also increases in malignancies, especially paraproteinemias and other states with abnormal serum proteins, and in autoimmune diseases. ESR elevations are used to support the diagnosis of specific inflammatory diseases, like systemic vasculitis and polymyalgia rheumatic. CRP is useful for monitoring patients after surgery and since it rises rapidly in response to bacterial sepsis, it is often used to monitor response to antimicrobial therapy. Considering the differences in these two “markers” it’s perhaps not surprising that they do not correlate well when compared against each other. Nor is it surprising that the lab has been unable to retire either test.
The pattern of usage for these tests in my lab has shifted in the last several years. In 2007 we ran almost equal numbers of both tests, about 500 per month of each. Eighty percent of the time, both tests were ordered simultaneously. Of those, 20 percent had one normal result and one abnormal result, 50 percent were both abnormal and 30 percent were both normal. Surprisingly, 50 percent of the time, only one single CRP and ESR was ordered, even though these tests are probably more useful when used to trend response and the majority of the time, one or both results were abnormal. This year in 2015 we are running about 1400 CRP per month and 900 ESR per month, and still 70 percent of those ESRs that we do run, are run simultaneously with CRP samples. The same services tend to order both tests, with many of the orders coming from GI, the ED, Orthopedics, Rheumatology, Oncology or Infectious Diseases. CRP tends to be ordered more frequently by general hospitalists, intensivists and Cardiology. ESR orders are STAT 30 percent of the time, while CRP orders are STAT about 22 percent of the time.
Both of these analytes are markers for the presence of an inflammatory process. CRP seems to reflect bacterial or septic processes and response to therapy to a better degree than ESR does, probably because CRP is one of the liver’s acute phase proteins and reflects liver response to injury. CRP also tends to respond more quickly than ESR, rising faster and then falling more rapidly. ESR on the other hand tends to reflect a more systemic response. With either analyte, a one-time order is a snap-shot in time. Thus often one of these markers is normal while the other is abnormal, which may explain why physicians tend to order both. Ordering either analyte as a one-time order will only tell you that inflammation is present, and the results of the tests must always be used in conjunction with other tests and clinical signs and symptoms in order to have any diagnostic efficacy. Sequential CRP or ESR samples allow for trending and helping to determine response to therapy, thus providing more useful information.

-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.
CLSI Publishes New and Revised Standards on POC Testing
From the press release:
“CLSI recently released new and revised standards on point-of-care testing in relation to glucose measuring and monitoring. Effects of Different Sample Types on Glucose Measurements, 1st Edition (POCT06-Ed1), provides information to assist the clinical and point-of-care staff in result and measurement procedure comparisons of glucose tests. Glucose Monitoring in Settings Without Laboratory Support, 3rd Edition (POCT13-Ed3), focuses on performance of point-of-care glucose monitoring systems, with an emphasis on safety practices, quality control, training, and administrative responsibility.“
These documents, including their sample pages, can be found on the CLSI Shop.
Microbiology Case Study: 22 Year Old Female with Joint Pain
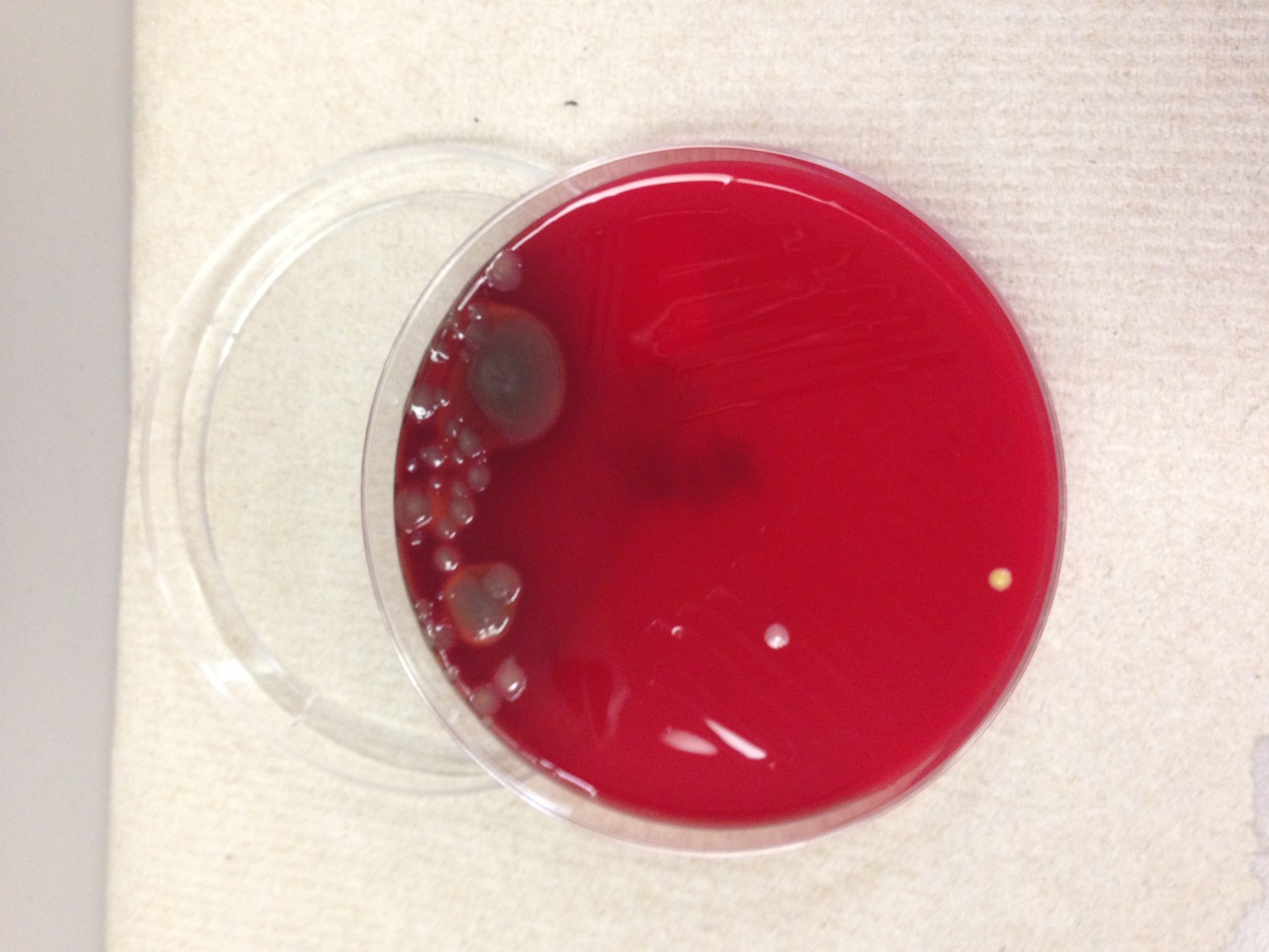
A 22 year old female with no significant past medical history presented with a fever, joint pain and a petechial rash. She endorsed having cold/flu symptoms for two weeks prior. The patient was admitted to the hospital where blood cultures were drawn and antibiotics were initiated. One set of blood cultures from the patient flagged positive at 14 hours of incubation with the following gram stain and colony morphology.


Photo courtesy of pixgood.com
Laboratory identification:
The patient’s blood was cultured on aerobic blood agar and chocolate agar plates. The gram stain revealed gram negative diplococci. Medium sized, round, gray to white, slightly mucoid colonies grew on blood and chocolate agars. The organism was definitively identified as Neisseria meningitidis by VITEK-MS. Prior to adoption of mass spectrometry, biochemical tests were performed for further characterization of the organism. Neisseria meningitidis is catalase positive, ferments glucose and maltose but not lactose, is oxidase positive, and does not reduce nitrate.
Discussion:
Neisseria meningitidis asymptomatically colonizes the oropharynx and nasopharynx of humans. It is transmitted by person-to-person spread of contaminated respiratory droplets. Infection causes a spectrum of disease including life-threatening meningitis. Bacteremia causes the characteristic petechial rash, thrombocytopenia, DIC, and shock. The organism may also cause conjunctivitis, pneumonia, and sinusitis. Its virulence factors include surface structures to facilitate attachment to and invasion of epithelial cells. Once the organism gains access to the vascular system, its survival is mediated by the polysaccharide capsule. Endotoxin release mediates many of the systemic manifestations of infection such as shock.
The differential diagnosis for this organism based on the gram stain and colony morphology includes Neisseria gonorrhoeae and Moraxella species. Different Neisseria species can be identified by the sugars they are able to ferment. For example, N. gonorrhoeae ferments only glucose, but N. meningitidis ferments both glucose and maltose.
There is a vaccine that is available for N. meningitidis that includes serogroups A, C, W-135, and Y. There are 12 different serogroups that can be distinguished based on the polysaccharide capsule. Our patient had been fully vaccinated. The isolate was sent to the state public health lab and it was reported back as non-typable and was sent to the CDC.
Treatment of N. meningitidis consists of supportive therapy for shock plus antimicrobial therapy with penicillin, ceftriaxone, or cefotaxime.
***Rare, fatal cases of meningococcal disease have been reported in laboratory staff. Any potential N. meningitidis should be worked with under a class II biological safety cabinet.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
New Technology for Transfusion Medicine
Late last year, the FDA approved Cerus’s INTERCEPT blood system for platelets and plasma. This system reduces the risk of transmitting blood-borne pathogens through platelets and plasma. INTERCEPT accomplishes this by inserting molecules into the DNA of pathogens that makes them incapable of replicating. While the pathogen still exists, it can’t replicate, and therefore can’t cause disease in the recipient. This is useful for well-known agents such as HIV or hepatitis as well as emerging diseases such as Chikungunya. Since it targets DNA, it would also neutralize undiscovered pathogens.
One potential downside of using this system is potentially increasing the cost of blood products for hospitals. Also, there is a bit of risk involved with being the so-called “first kid on the block” when using any new technology. While the FDA approval process is rigorous, unforeseen complications can arise with widespread use. Since the FDA approval, several blood centers—Delmarva, SunCoast, and Bonfils—have signed agreements to use this this system to ensure the functional sterility of their blood products. It will be interesting to see how widely this new technology is adopted and if blood products are made safer than with current methodologies.
If you’d like to read papers about this technology, you can find them here.
Reconsidering Mass Transfusion Protocols
In a new article exclusive to the Lab Medicine website, Gregory et al discuss mass transfusion protocols and argue against the 1:1:1 (1 unit each of platelets, plasma, and packed red blood cells) dogma. You can follow this link to read the paper.
What do you think? Is it time to reevaluate mass transfusion protocols?
What’s That Interference?
I’ve heard it said that there is no such thing as a lab test with no interferences, and I have to admit, I believe that to be true. For every method devised to measure a specific analyte, something else can interfere with that measurement. For example, photometric measurements using absorbance assume that only the analyte of interest absorbs light at the wavelength being used. Quite often, many other compounds absorb light at that wavelength as well. In chromatography methods, we assume only the compound of interest elutes from the column at a specific time point, and again, many other compounds often do. Various types of mass spectrometry are touted as specific for the compounds being measured, however, even using mass spectrometry, compounds may fragment in similar patterns when looking at mass spectra, or fragment into the same size precursor and/or product fragments using tandem MS.
Thus, we routinely report test results knowing that most often what we are reporting is accurate. However, we must always be aware that the result we’re reporting may not be accurate due to interferences.
I recently had an occurrence related to test interference. Like all such cases, the tech responding to the clinician’s call used our standard response. He located the original sample and repeated the test. The assay gave the same results on the repeat and the result was reported back to the clinician as real and accurate, even when questions were raised by the healthcare staff about the result not fitting the clinical picture. And in fact, although the result was reproducible and in the realm of possibility, in this case the result was wrong.
The analyte in this case was plasma free hemoglobin which is performed in our lab by an assay which measures absorbance at one of the wavelengths at which hemoglobin absorbs light and subtracts a background wavelength reading. The test was persistently giving very high plasma free hemoglobin results even though the patient had no other evidence of hemolysis. When the healthcare staff became adamant about the discrepancy, the sample was sent to an outside lab which performs the assay using a full spectrophotometer, and the sample was found to have no hemoglobin present. An interferent in this patient’s sample was being measured as hemoglobin by our method.
Of course, once it’s been determined that a test is experiencing interference the next question from the healthcare provider is always, what is interfering? That’s a much more difficult question to answer, although occasionally it can be answered with some investigation. Looking into the patient’s drug regimen can help, as well as checking other health parameters to see what else is occurring. In the case of the elevated plasma free hemoglobin, the patient did have an elevated myoglobin which may have interfered.
The take home message here is that no matter how reproducible the results are, interferences are possible. As laboratory professionals, we should always be ready to look for ways to prove our results other than by repeating them, especially when the result does not fit the clinical picture and is being questioned by our healthcare colleagues. Sending the test to be run by a different method is one good way of determining interference. Another way is to check the patient’s chart for drugs or other substances that are known to interfere and are listed in the package insert. Finally, understanding the realities of assay interferences, and being willing to continue looking for answers is also important in the laboratory.
-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.
Mentoring Throughout Your Career: A Q&A With Jennifer Hunt, MD

At the 2014 ASCP Annual Meeting in Tampa, Fla., Jennifer Hunt, MD, MEd, FASCP, chair of the Department of Pathology at the University of Arkansas for Medical Sciences, had the opportunity to discuss with curious audience members the influence her mentor has had on her since she started her career. What made the experience even more special was that her mentor, Virginia LiVolsi, MD, MASCP, professor of pathology and laboratory medicine at Penn Medicine, sat right next to her and provided her own view of their mentoring relationship.
The session, which also featured an interview with special guest Barbara Pierce Bush, was out of the norm for a scientific meeting, but the topic is an engaging one, and crucial for pathology and laboratory professionals as they advance in their careers. Here, Dr. Hunt talks to Molly Strzelecki, senior editor for ASCP’s Critical Values, about her experience as both a mentor and a mentee, as well as how pathology and laboratory professionals can develop such relationships for themselves.
Molly Strzelecki (MS): When did you start mentoring others, and what are some characteristics a good mentor should have?
Jennifer Hunt (JH): As a mentor, I think it started rather early on, mentoring people who were junior to me—for example, when I was a chief resident and talking to first-year residents, or talking to junior faculty members and working with fellows. No matter where you are in your career, you’re probably a mentor to someone, whether you know it or not. Sometimes people don’t see the role as a mentor; they see the role as a friend. But if there are generational differences or differences in your status, then you’re probably mentoring as well as being a friend.
The mentor role varies based on the relationship, and what you’re mentoring the person for. I think it’s important to remember that no one mentor will be everything to you, as a mentee. You can’t have just one person and have them teach you everything. More than likely you’ll need multiple mentors at any given time in your career. And that mentor needs to recognize his or her limitations, and be able to send that mentee off to other people rather than trying to be everything to one person.
Great mentors share willingly—not just their opinions, but their opportunities, their professional interests, and the culture of their profession. They connect people. Dr. LiVolsi is the best person at that I have ever known—at meetings she would introduce me to everybody. And that becomes very important. Mentors are generous with their time, even though they are busy, and they’re wise in the areas you need them to be.
Good mentors don’t need credit for what they do. The credit is appreciated, and the mentee needs to recognize what mentors have done for them, but that’s not why mentors do what they do. There’s a lot that goes on behind the scenes. Often, my best mentors have done things that I never knew about, and I may still not know the extent. I am sure that so many of the opportunities that have come my way in life are because Dr. LiVolsi recommended me or suggested my name.
MS: Is it better to let mentorship evolve naturally, or seek it out specifically?
JH: It’s a combination of both. My relationship with Dr. LiVolsi was a very natural evolution, but I’ve had other mentors I approached about being my mentor for something specific. For example, in one of my jobs I wanted to learn lean process improvement, and to explore Six Sigma. So I went to someone in the institution who was pretty senior, and not a physician, and was in charge of those elements, and asked for his help. And he became a mentor not just for those subjects, but for many things.
I think seeking people out in situations like that is very practical and reasonable. And it’s not as awkward as it can sometimes be to seek out a general mentor—you’re approaching a person with a specific skill set and a specific goal in mind. It’s good for both people in the potential mentorship to understand what you’re looking for, or what the skill set is you’re trying to gain, or what the area is you need help with, and to start off with a narrow focus rather than a broad one. It’s easier for you to ask for that, and it’s easier for the other person to say yes when there are well understood limits to the relationship.
Getting to know each other is part of the process, too, whether the mentorship evolves naturally or is asked for specifically. It can be a little clunky, getting to know your mentee and vice versa. It is usually a little bit social, not all professional, and involves figuring out what makes people tick.
MS: Once you’ve found a mentor, how can you make sure you are getting the most out of the mentoring relationship?
JH: Good mentees ask the right questions. One of the things I often see as a problem for mentees is they ask “yes or no” questions, when what they really want is someone to think through an issue with them, and talk through the pros and cons. You don’t want a one-word answer or guidance, because you, as the mentee, may decide differently, which could put you at odds with your mentor. Ask questions that are more open-ended or opinion-based and thought provoking. Not, “Should I write this paper?” Rather, “What would be the benefit to my career if I write this paper?”
Good mentees don’t wait until it is too late for meaningful assistance—they reach out early and they don’t wait until decisions are made and paths are created, when things are harder to turn around. They ask early and touch base and connect while they’re going through things.
Good mentees don’t demand too much. There is a fine line between touching base frequently and bothering your mentor. And I think good mentees follow through and take advantage of opportunities that their mentors create for them. I’ve encountered people for whom you’d find an opportunity, and in response they’d tell me they were too busy. That’s not a good answer. I am “too busy,” too, most of the time but if I find time to present a career enhancing opportunity for a junior faculty member, let us say, the least that person can do is express some interest and enthusiasm even if that person does not feel that way.
MS: How does mentoring benefit pathology and laboratory medicine overall?
JH: If you’re talking about clinical mentoring, we transfer a lot of our knowledge and experience to others through mentoring relationships. We share cases—pathologists are never shy about sharing cases with each other, ever, and I don’t know a lot of surgeons who call each other into the operating room to ask a colleague for help. They tend to be more independent. But in pathology, we share cases; it’s part of the culture. And that’s mentoring. You share a case, you hear people’s opinions, you gather from them, and it’s in many ways mentoring, even though it’s also education.
And it never stops. I still show cases to people. Sharing is part of the process of working through it intellectually—we’re in an extremely collaborative profession. And it also makes for really excellent patient care that way, because we know we have many people to tap into for the best diagnosis.
-Ms. Strzelecki is Senior Editor of Critical Values.
–This interview originally appeared in the digital July issue of Critical Values.
Microbiology Case Study–Joint Pain After Left Knee Arthroscopy
Case history:
A 51 year old male with a history of recent left knee arthroscopy presented with increasing joint pain, swelling, and reduced range of motion accompanied by subjective fevers. He was receiving physical therapy and admitted to soaking the knee in a hot tub on two occasions after the therapy sessions. An aspirate of synovial fluid obtained at the clinic showed the following colony morphology and Gram stain:

Laboratory identification:
Pseudomonas aeruginosa is a non-spore forming, non-encapsulate, motile gram-negative bacillus. The bacteria typically form characteristic colonies with a metallic sheen and have a green-blue appearance due to production of soluble blue phenazine pigment (pyocyanin) and yellow-green pigment fluorescein (or pyoverdin). The organisms classically emit a grape-like odor in culture. They are oxidase positive. Lab diagnosis is based on colony morphology and the organism’s biochemical characteristics. P. aeruginosa is also the only clinically significant fluorescent pseudomonad that grows at 42oC. In our laboratory, the isolate was identified on the MALDI-TOF.
Discussion:
P. aeruginosa has been documented to infect any external site or organ. Community acquired infections are associated with otitis media, skin ulcers, corneal infection, and rashes secondary to contaminated hot tub water which is consistent with our patient’s history. Hospital acquired infections are typically related to catheters, bedsores, burns, and eye infections. People with cystic fibrosis are particularly susceptible to infection with this organism although asymptomatic colonization in these patients is also possible. Patients with extensive burns are also at risk for infection with Pseudomonas. Rarely, a septicemic infection characterized by black necrotic skin lesions known as ecthyma gangrenosum may happen.
The organism has two important virulence factors for pathogenesis- exotoxin A and exoenzyme S. It also produces various cytotoxic substances, all of which contribute to the local tissue destruction.
Pseudomonas infections can be treated with aminoglycosides, beta lactam, and fluoroquinolone antibiotics.
-Lauren Pearson, D.O. is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
