Radioactivity is no longer common in most clinical laboratories. At one point in my career, radioimmunoassays were commonly found in laboratories, and most labs had institutional radiation safety plans and carefully followed the CAP checklist for handling and dealing with radioactivity. With the advent of enzyme-linked immunoassays, sensitive nephelometers, various fluorescent and chemiluminescent technologies, and then mass spectrometry, radiation was quickly replaced in most clinical labs. The general prevailing thought was: Why deal with radiation if you don’t have to? Now days, radioimmunoassays are essentially only found in reference labs and utilized for esoteric analytes or those which cannot be measured any other way.
Despite that being true, it’s important for a lab to know what to do if radioactive materials should appear in the lab. How likely is that to happen? Perhaps more likely than you may think. Last week a sample shipped to us from an outside institution set off the radioactivity monitor on our hospital loading dock. The package was on a delivery cart with other packages so per protocol, the whole cart went to nuclear medicine where it was determined that the radioactive package was for the lab and it was brought to us. The radioactive sample turned out to be a urine sample for VMA/HVA analysis from a patient on a new cancer treatment protocol. The urine was indeed radioactive.
The shipping institution was contacted and the packaging personnel had no idea either that the sample was radioactive, although they were aware a new protocol was going into place. Working with our nuclear medicine department and the institutional radiation safety group, we have now once again put appropriate processes in place to handle and deal with radioactivity. And we’ve dusted off our old CAP checklist regulations as well.
This episode actually turned out to be a benefit to us, as we discovered that our own nuclear medicine department will be starting this new protocol soon, and had not thought ahead to possible radioactive samples sent to the lab. We are now working closely with them to ensure proper procedures and safeguards, and have a plan of action clearly in place. We also continue to work with the institution that sends us samples. The very next sample from them was properly labeled as potentially radioactive.
-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.
Just returning from the ASCP 2015 conference in Long Beach, California, I can’t help but reflect on what a wonderful experience I had. The weather was picturesque, attendees at an all time high, and a variety of educational offerings and speakers on point.
The highlight for myself (and I know I am not speaking out of line when I mention the four other amazing ladies) was being recognized as ASCP’s Top Five from the 40 Under Forty program this year. I cannot begin to tell you how refreshing and energizing it is to be a part of an amazing group of five women who are all dedicated to advancement in Pathology and Laboratory Science.
To be honest, I was a little nervous going into the meeting… What would the other honorees be like? What would they think of me? Am I going to be completely out of my league there? Well let me tell you, everyone that I met was wonderful! We discussed a variety of topics, and even tossed around an idea for future collaboration.
Yes, I could go on and on about my new friends, but I think what I want to point out is that it cannot, and should not go unnoticed that the Top 5 this year consisted of all women, all WELL deserving women at that. How were we chosen? Yes, we blogged, but don’t forget that we also submitted CVs and biographies. We wrote essays as well as recorded videos (some of us spending hours re-shooting and cringing at ourselves). Not to mention, votes were cast by a dedicated panel as well as online voters. Your 40 Under Forty, including the Top Five, came from all over the country and represent various specialties in our field.
Unfortunately, at some point I had to come down from the “girl power” high. I returned to Milwaukee and thought to myself, I wonder what the ratio of men to women is in our laboratory alone? A few short minutes later, I crunched the numbers and it was easy to see that women make up 85% of laboratory staff at our organization. The totals are inclusive of all laboratory departments and shifts as well as administrative support, Pathologists, and Directors at Children’s Hospital of Wisconsin.
It was during these thoughts on women in science and recognition, that I remembered an article I had read quite a while back. The article had discussed how historically, women occupied most of the laboratory jobs (the strange term, “lab gals” sticks out in my mind). This was thought to be the case because it was believed that women had more patience, were more detail oriented, and therefore were trained to perform the work that doctors did not want to do. At the same time, men typically occupied the higher-level decision making positions (those that required an advanced degree, PhD, and MD). I thought to myself that even today, it sure does seem that there are more women in the laboratory profession. However, we have come a long way and are seeing an increase in women being honored for their education, professional achievements, and advancements in the field. Every single lead technologist and laboratory manager at our institution as well as the CEO of our health system currently is female. Interestingly, more than HALF of the 40 Under Forty Honorees this year are highly educated women with advanced degrees!
We all know full well that more than 70% of critical medical decisions are based on laboratory results. Therefore, if the field of laboratory professionals is made up of mostly women, it appears that our attention to detail is instrumental in making some major decisions. Yes, there still may be gender gaps when comparing men to women in academia however, what once was a field dominated by the male PhDs and MDs, appears to be shifting majorly as more and more women are making their presence known in Pathology and Laboratory Science.
I applaud everyone who was honored this year as one of ASCPs 40 Under Forty. Women are the past, present, and the future of laboratory science and medicine and it brings a little extra smile to my face to know that so many well deserving women are being recognized by ASCP this year.
2015 ASCP 40 Under Forty Top Five: Amanda Wehler, Tiffany Channer, Jennifer Dawson, LeAnne Noll, and Kimberly Russell
-LeAnne Noll, BS, MB(ASCP)CM is a molecular technologist at Children’s Hospital of Wisconsin and was recognized as one of ASCP’s Top Five from the 40 Under Forty Program in 2015.
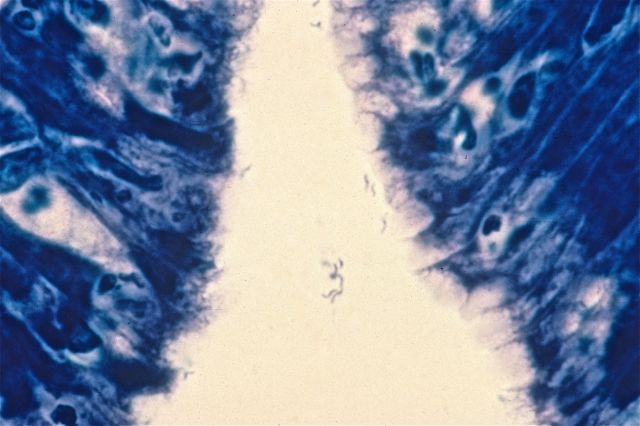
A 68 year old male presents with chronic, gnawing epigastric pain which has been getting worse over the past year. An endoscopy is performed and a representative gastric biopsy section, stained with Giemsa stain, is shown here. What organism is responsible for this patient’s symptoms?
A. Candida albicans
B. Helicobacter pylori
C. Bacillus cereus
D. Staphylococcus aureus
E. Campylobacter jejunum
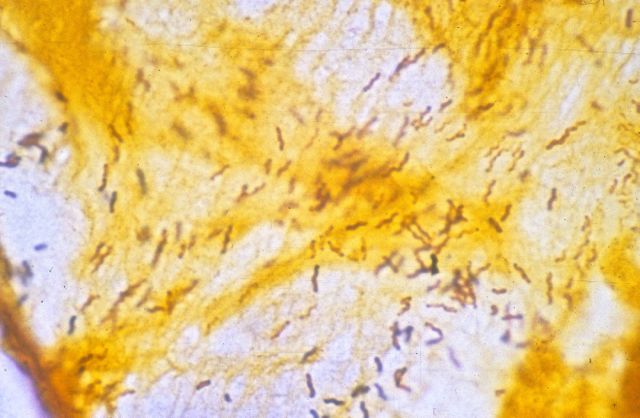
The diagnosis in this case is Helicobacter pylori. Described by Warren and Marshall in 1983, Helicobacter pylori is now known to be the cause of most cases of chronic gastritis and peptic ulcer. Helicobacter is a tiny, corkscrew-shaped bacillus, and is easily missed on routine H and E-stained histologic sections. Giemsa staining, as seen in the image above, can be helpful, as can silver staining, as seen in this image:
Helicobacter does not invade the gastric mucosa, but produces its symptoms through continual stimulation of the host immune response. Treatment involves triple therapy (e.g., omeprazole, amoxicillin and clarithromycin), and prognosis is excellent. A small number of patients, however, develop gastric adenocarcinoma or MALT lymphoma.
-Kristine Krafts, MD, is an Assistant Professor of Pathology at the University of Minnesota School of Medicine and School of Dentistry and the founder of the educational website Pathology Student.
An elementary school aged boy with a history of pre-B cell acute lymphocytic leukemia with a failed bone marrow transplant was transferred to a regional children’s hospital for leukodepletion and participation in an experimental clinical trial. At that time, his CBC was significant for 10% polymorphonuclear cells and 50% blasts. He was subsequently transferred to the ICU in respiratory failure and developed papulonecrotic lesions on his face, trunk, and bilateral legs. Prior to this, he was pancytopenic with no blasts present with cell counts of 100 WBC, hemoglobin 8.3 and 37,000 platelets. His Fungitell assay, which detects (1-3)-β-d-glucan, was positive.
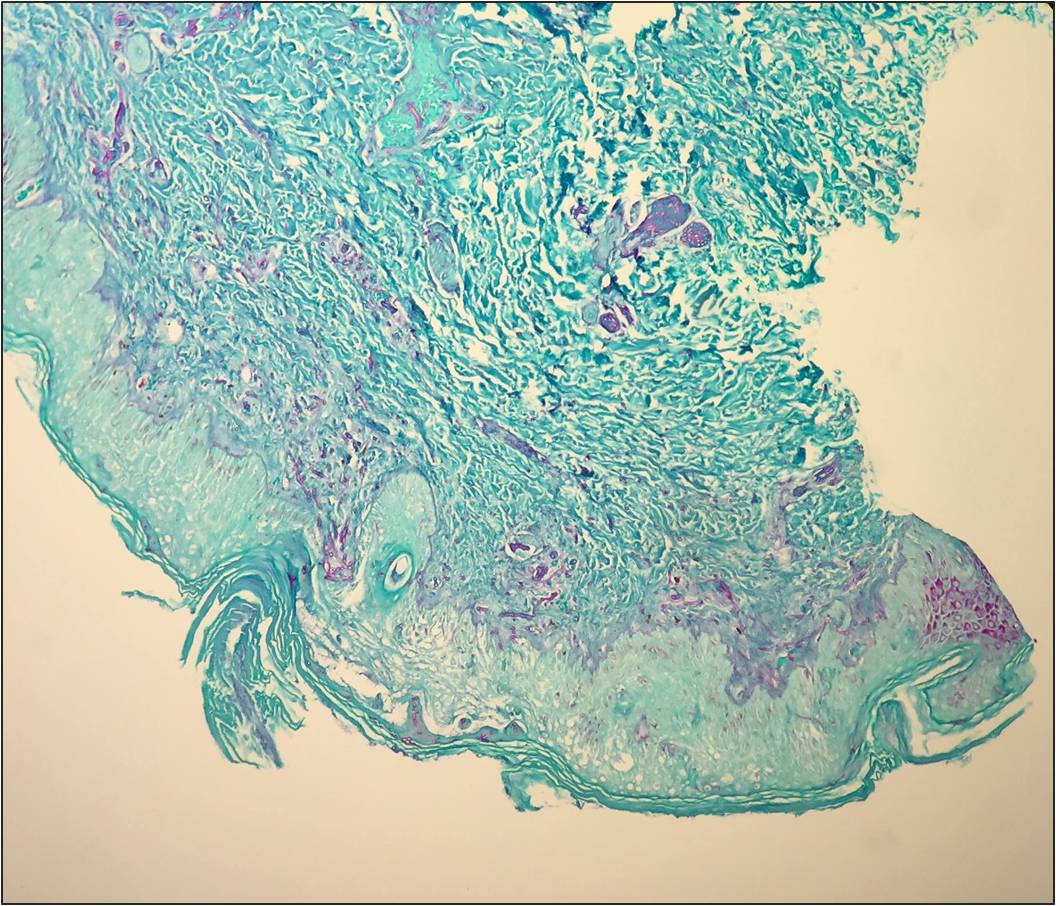
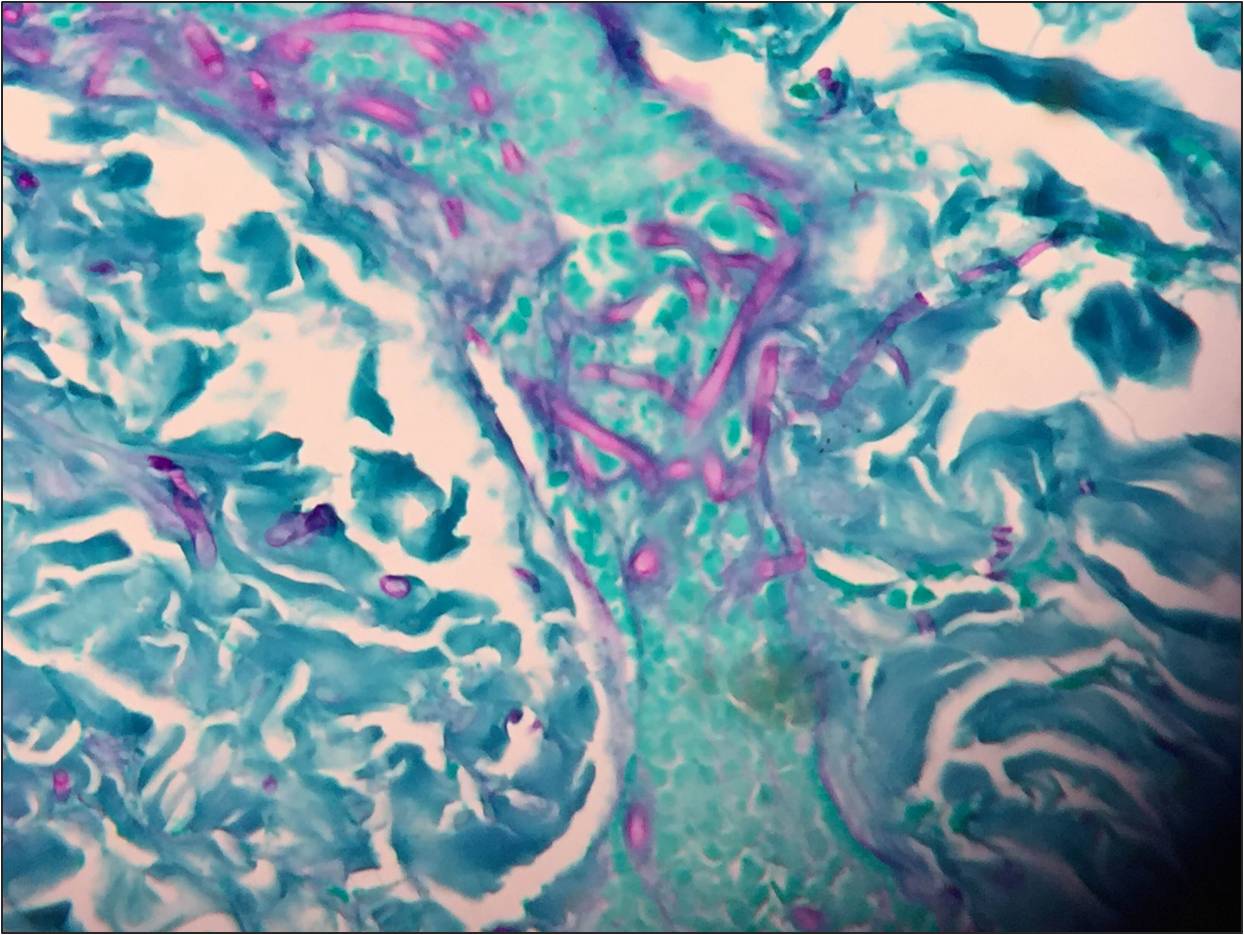
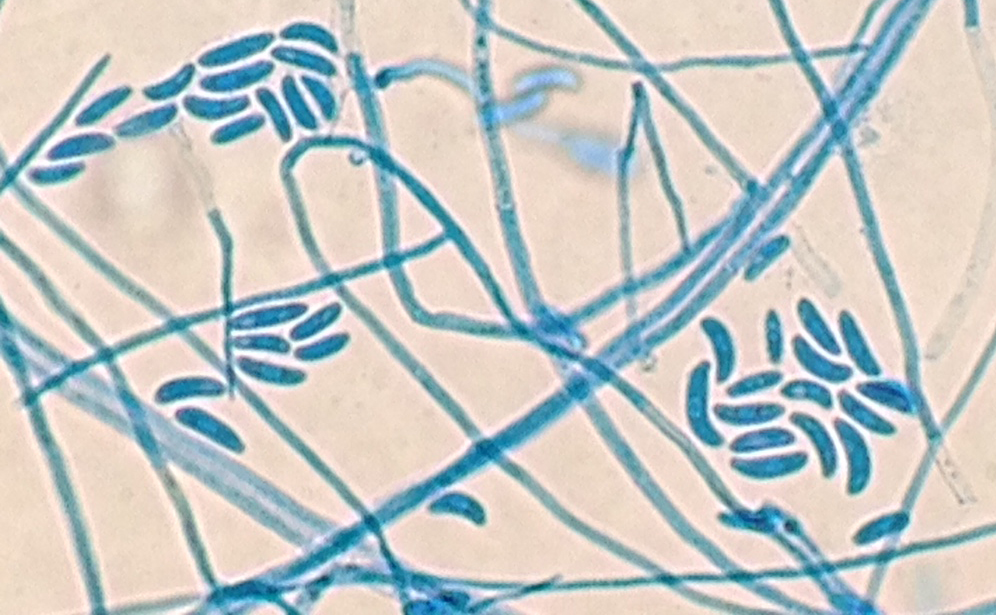
Routine blood culture, fungal culture from the endotracheal tube, and fungal culture from the skin lesion biopsy specimens all had fungal elements on KOH stain. Young growth of a whitish, fluffy mold was present on all cultures within two days. Histopathology on the punch biopsy of a skin lesion on the thigh showed septate hyphae within the dermis, epidermis, and invading the vasculature that was particularly apparent with GMS stain (Figure 1a and 1b). Within a few days, the fungal cultures showed septate hyphae with microconidia using lactophenol cotton blue tape preparation, and shortly thereafter the mold developed into macroconidia with multiple septations taking on canoe-like forms (Figure 2). The white, cotton-like colonies developed a pink tinge (Figure 3). These characteristics allowed for the identification of the growth as Fusarium sp.
Septate hyphae on GMS stained section of the skin punch biopsy.Septate hyphae on GMS stained section of the skin punch biopsy.Microscopic identification of Fusarium by lactophenol cotton blue stain.Colony of Fusarium growing on inhibitory mold agar (IMA).
Fusarium is an opportunistic hyaline mold with infection most commonly seen in immunocompromised hosts. It can cause keratitis through contamination of contact lenses, penetration due to trauma, or use of immunosuppressive steroid ophthalmic solution. It is increasingly becoming the cause of disseminated infection in neutropenic hosts with a broader spectrum of disease, which includes: skin lesions, fungemia, rhinocerebral involvement and pneumonia. In these cases, without an immune system to fight the infection, mortality is high. Inhalation of airborne conidia, ingestion from water sources or access through mucosal membranes are all potential points of entry.
The colony growth on plated fungal media is rapid, usually maturing within four days. On microscopic examination, Fusarium hyphae are septate, approximately 3-6 microns wide with acute angle branching. Microconidia are small, oval-shaped, and no larger than 4 x 8 microns in size. These can look like Acremonium sp. Macroconidia are canoe- or sickle-shaped with the largest dimension being about 80 microns in length, exhibiting 3-5 septatations.
–Jodi Music, MD, is an AP/CP resident at UT Southwestern Medical Center.
-Erin McElvania TeKippe, Ph.D., D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.
We can’t talk about Molecular Diagnostics without possibly talking about DNA, and with DNA, comes mutation. Much of the work I do revolves around searching for specific variants in a patient’s DNA sequence. We all have mutations in our DNA, but does that mean we all are affected negatively? Absolutely not. Spontaneous mutations occur during normal process such as DNA replication and repair within our cells. They also can arise from exposure to ionizing radiation, UV exposure, and chemical agents. Some mutations are passed down through reproductive cells. Mutations can be categorized as harmless or sometimes hurtful giving rise to gene defects, copy number variants, metabolic deficiencies, and cancer, while others result in positive effects.
Where do mutations occur?
Somatic mutations occur in cells that aren’t reproductive in nature. These mutations for the most part do not have a blatant effect on the organism because our normal body cells are able to counteract the mutated cells. However, sometimes mutations in somatic cells can affect division of cells, which has the potential to result in forms of cancer. On the contrary, germ-line mutations occur in reproductive cells and have the possibility of being passed down through generations, resulting in the presence of the mutation in all of the organism’s cells.
Understanding DNA
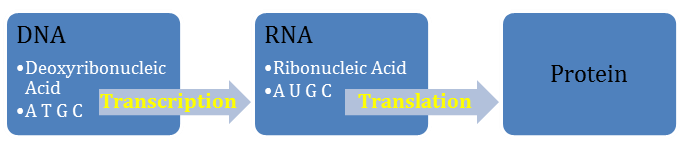
A T G C bases, along with a sugar, and a phosphate group combine to form a polymer of nucleotides. This polymer backbone of alternating sugar and phosphates is what we call DNA (Deoxyribonucleic Acid). DNA is transcribed to RNA (Ribonucleic Acid) which instead of Thymine (T) contains a Uracil (U). Finally, RNA is translated to protein.
Pyrimidines
Purines
Single-ringed organic bases
Double-ringed organic bases
Thymine (T)
Cytosine (C)
Uracil (U)
Adenine (A)
Guanine (G)
Hydrogen Bonds Between Complimentary Strands of DNA
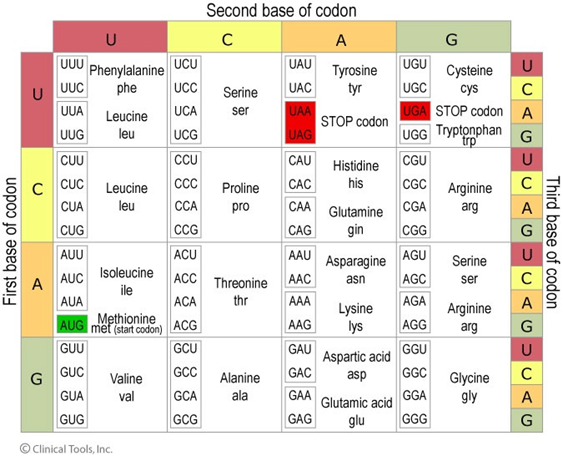
Amino acids are the triplet codons that make up proteins. It is extremely important to become familiar with the codon table. You don’t need to memorize it, however you should at a minimum know what triplets code for START and STOP codons. You will quickly see that there are multiple codes for a single amino acid. This becomes important when considering the effects of mutation:
Like I mentioned earlier, many of the tests I perform involve screening for variants in DNA sequence. I accomplish this through different methods, which I will touch on in future blog posts. We could easily discuss mutations for hours and hours, but for now, it’s probably most important to gain a quick (and simple) understanding of the types of mutations and what the resulting effects can be. For the sake of demonstration, let us consider the following normal (wild type) sequence pattern:
NOTE: Uracil replaces Thymine because of transcription from DNA to single stranded messenger RNA (mRNA)
Transition Mutations occur when mispairing results in a purine being replaced with a different purine, or a pyrimidine replaced with a different pyrimidine:
A→G
C→T
Transversion Mutations occur when a purine is replaced with a pyrimidine or vice versa:
A→T
C→G
Missense Mutations have the ability to result in a change in the amino acid. This happens when the codon triplet is altered, and the amino acid sequence of the encoded protein is changed:
Sometimes, Missense Mutations are silent:
Notice how the structure of the gene product is unchanged. This happens because all amino acids can be encoded by more than one triplet codon.
Frame shift mutations can result from either a single base insertion or a single base deletion.
Insertion.Deletion.
Nonsense mutations are exactly what they are called… Nonsense! Here, a base substitution changes an amino acid into a stop codon. Nonsense mutations result in abnormal termination of translation and the protein product is shortened:
Chromosomal Abnormalities
Sometimes changes in the actual chromosomal structure or number take place in the cells. These changes can result in deletions, duplications, inversions, and translocations of chromosomes. Chromosomal deletions and insertions are simply the loss or gain of chromosomal material. Inversions result from the removal, flipping, and then reconnection of the chromosomal material within the same chromosome.
Translocations are more complicated and involve switching of genetic material between two chromosomes. A reciprocal translocation occurs when parts from two different chromosomes exchange. We call a reciprocal translocation “balanced” when there isn’t a gain or loss of genetic material between the chromosomes (both chromosomes remain fully functional). An “unbalanced” reciprocal translocation affects an offspring’s phenotype due to extra or missing genes.
This information I have touched on is very general, however, it doesn’t mean it is not of importance. These basic concepts are the fundamentals needed to begin understanding mutation as they will provide us with the framework for recognizing the needs and importance of molecular diagnostic testing!
Test your Molecular Knowledge
What amino acids do the following codons code for:
GAU
AUG
UAG
CAG
UGA
Classify the following mutations:
T→A
T→C
AGA→UGA
AGA→AAA
AGA→CGA
Answers
1 a) Aspartic Acid b) Methionine (start) c) Stop codon d) Glutamine e) Stop codon. 2 a)Transversion b) Transition c) Nonsense d) Missense e) Silent
-LeAnne Noll, BS, MB(ASCP)CM is a molecular technologist at Children’s Hospital of Wisconsin and was recognized as one of ASCP’s Top Five from the 40 Under Forty Program in 2015.
Case History:
A 76 year old female presents with a two year history of worsening upper back pain. Imaging revealed compression fractures of the first three thoracic vertebrae (T1-T3). Fine needle aspiration and a core biopsy of the T3 vertebral body were examined in surgical pathology. There was acute and chronic granulomatous inflammation with fungal organisms observed on histologic examination. Surgery for decompression and fusion of C5-T6 vertebrae was performed and tissue was sent for fungal culture.
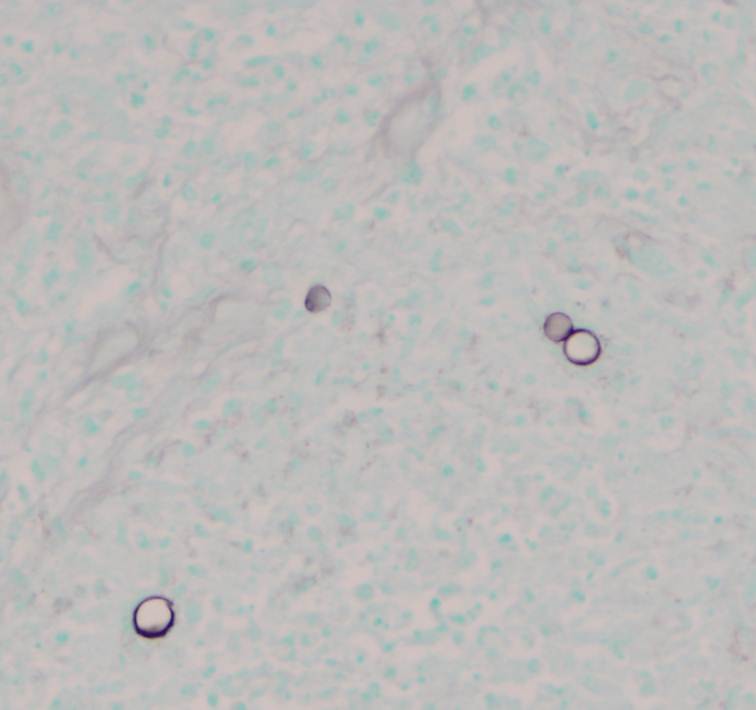
Potato flake agar shows a tan-brown fungus.Mycosel agar shows beige-white fungal growth.Scotch tape prep shows septate hyphae with unbranched conidiophores and single, terminal, “lollipop” conidia.Silver stain of involved bone with fungal organisms exhibiting broad-based budding.
Laboratory Identification:
The workup revealed a thermally dimorphic fungus with a mold form growing in the laboratory at 25°C and a yeast form present in the surgical pathology specimen. The mold form is moderately slow growing and has septate hyphae with small, round, terminal conidia often described as “lollipops.” The yeast form is large (8-15 microns) with broad based buds and double contoured cell walls. The immune system reacts to the presence of the fungus by forming granulomas and leads to acute and chronic inflammation within the involved tissue. The organisms can occasionally be seen within giant cells in histologic sections. The silver stain, as seen above, highlights the organisms.
Discussion:
The fungus described above exhibits the features of Blastomyces dermatitidis. This organism resides in soil and decaying plant matter and is endemic to eastern North America including the Mississippi and Ohio River Valleys as well as areas surrounding the Great Lakes and St. Lawrence River. The most common primary sites of involvement for Blastomyces are cutaneous and pulmonary. Following a primary infection, the disease can progress to disseminated blastomycosis which involves other sites such as bone.
The primary site of infection in this case is unknown. There was no history of cutaneous ulcers and chest imaging was unremarkable. The patient did have a remote history of bloody sputum production which she had attributed to “dental difficulties” that she was experiencing and has since resolved. This may have been evidence of a primary pulmonary infection preceding the vertebral involvement; however it is difficult to say with certainty.
The classic double contoured cell walls are not evident on the silver stain of the surgical pathology specimen in this case. This may be due to the fact that the bone required decalcification before histologic sections could be taken. The decalcification process may have caused an artifactual loss of the double contour. Despite the fact that this classic finding was not seen, the macroscopic and microscopic morphology is most consistent with Blastomyces.
The patient is being treated with long-term itraconazole and is currently doing well.
-Britni Bryant, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.
You know that old adage “you can’t teach an old dog new tricks”? Well, laboratory professionals know that’s wrong—not only do we need to learn new tricks, sometimes we need to learn them in order to help diagnose a patient. In that regard, continuing education sessions—like those at ASCP’s Annual Meeting—can be so helpful to bench technologists. Today, I attended “Team Approach to Diagnosis of Fungal Infections” presented by Dr. Jeannette Guarner, MD, FASCP from Emory University in Atlanta, Georgia. Here are some of the tidbits I learned.
An easy reminder for dimorphic fungus: “mold in the cold, yeast in the beast.”
In direct stains of tissue samples, not all broad-based budding yeast 8 to 15 microns are Blastomyces. It could be Candida or even Aspergillus.
If you’re able, tell the clinician to send to biopsy samples for micro AND pathology—shared specimens tend to introduce error.
Paracoccidioidomycosis is much more common in males (20:1); current thinking is that estrogen is protective.
Chrysosporium (previously Emmonsia): dimorphic yeast currently only seen in South Africa.
Fusarium can grow in blood cultures. (In the tissue, it almost looked like Aspergillus with hyaline septated hyphae.)
Fusarium is generally resistant to antifungals
When seen in tissue samples, hyaline septated hyphae DOES NOT ALWAYS equal Aspergillus.
Black molds are black because of melanin, which protects them from UV rays, heavy metals, free radicals, and high temperatures.
Cryptococcus is the only fungus that has mucin in its cell wall; mucin stain will be positive.
Crypto can sometimes do a broad-based budding.
-Kelly Swails, MT(ASCP), is a laboratory professional, recovering microbiologist, and web editor for Lab Medicine.
Hello again readers. It’s been a while as I took some time off from blogging. But I hope to update you every once in a while when I can. So, I’m currently in my final year of residency and have been serving as chief since April 1st. My chief term ends before the end of the year to provide time to focus on studying for the boards (we take our boards in mid-May).
When I reminisce about residency, I can’t believe that almost four years have flown by so quickly. I remember arriving in Chicago for a 2 week boot camp we had prior to our start date on July 1st just like it was yesterday. It was nice to be back in a familiar city (The University of Chicago is my alma mater), although many things had changed in the two decades since I had last been a college student in the Windy City.
Thinking about it now, I really appreciate all the thought and hard work that my director of surgical pathology, Dr. Elizabeth Wiley, had put into organizing this boot camp to ease us into the transition to residency (and surgical pathology). We learned Rokitansky method of autopsy dissection on 3 pig blocks that she personally picked up from the butcher’s for us and later had to complete a competency exam by ourselves on a 4th pig block. We learned to cut frozen sections on various tissues from our pig blocks (and of course, had a competency exam on that as well). We learned to gross uteri and prostates on ground turkey versions (complete with chickpea leiomyomas) that she and her fellows had made for us. We had weekly online exams on histology (we had a slide scanner which I now appreciate that not everyone has one) and special didactics on surgical pathology topics we don’t see much during general sign-out (dermatopathology, neuropathology, hepatopathology, and nephropathology) in addition to the usual goings-on during a surgical pathology rotation. We eventually had online modules on surgical pathology as well. And of course, we had three months straight (I hear its five months now) of learning to gross with our awesome fellows. I now appreciate more deeply just how innovative and dedicated Dr. Wiley was to our surgical pathology education. And even though I ultimately chose to pursue fellowships in hematopathology and molecular genetic pathology, the foundation in surgical pathology that was established during that boot camp still helps and influences me now.
During my first year, I was also fortunate to have hematopathology at Jesse Brown VA Medical Center with Dr. John Kennedy. He is a hematopathologist who was trained as a morphologist before the heavy reliance on flow cytometry and IHC. And he taught me to love the morphology of blood cells especially with respect to lymphomas. I had enjoyed my hematology sub-I at the NIH when I was a medical student but had originally entered residency thinking that I’d pursue molecular genetic pathology and clinical microbiology. But a great mentor can really open your mind to a different path and that is what Dr. Kennedy did for me. The second time I rotated with him, he was away for much of the rotation. But I loved the opportunity that I was given to take care of the hematopathology service in his absence. I looked at all the daily cases and performed path reviews and counts on peripheral blood smears and body fluids and the surgical pathology attending at the end of the day would review and sign-out my work. This experience of graduated responsibility helped me to decide to pursue hematopathology and it was nice to have someone believe in me and my abilities. I was also fortunate that I was in a city where the Lymphoma Foundation also held quarterly inter-program Lymphoma Rounds which I was able to attend.
So my advice is to identify mentors early on in your residency. You may not be able to see the ripple effect they have on your life until later on but I promise that they will touch your lives in an indelible manner that will help shape the pathologist you will become later on in life.
This week I’m at the ASCP Annual Meeting and will write about those experiences in a future blog, but for now, I’d like to take this opportunity to personally thank my mentors. I hope that I take your lessons and make you proud as a future physician-scientist with a public health (molecular epidemiology aka biomarker discovery which was one of my areas of specialization during my MPH) focus. You have touched my life in ways that I may not always be able to articulate but do acknowledge and appreciate.
-Betty Chung, DO, MPH, MAis a fourth year resident physician at Rutgers – Robert Wood Johnson University Hospital in New Brunswick, NJ.
One of the interesting things about working in the field of laboratory medicine is that there are always opportunities for learning new things. Almost every call I get from my colleagues outside the lab allows me and the lab team these opportunities. And sometimes we are reminded of the reason we do the things we do, basically re-learning them.
Case in point: An ICU physician contacted the lab, understandably concerned. He had been monitoring the pO2 in a patient using an I-Stat point of care analyzer. Values had been in the range of 50-70 mmHg, and he had been adjusting ventilation on the basis of those results. A blood gas sample was sent to the main lab, analyzed on an ABL analyzer and gave a result of 165 mmHg, repeated shortly thereafter on a new sample with a 169 mmHg. Understandably, the physician wanted to know which analyzer was wrong and how he should be adjusting his patient’s ventilation.
We quickly did an investigation and determined an interesting fact that we hadn’t paid much attention to previously. A blood gas sample that is sent through the tube system that has any amount of air in the sample, will give falsely elevated pO2 result. We investigated this by collecting blood gas samples, running them on both the I-Stat and the ABL, and then sending them through the tube system and rerunning them on both instruments after tubing. The pO2 values matched on both instruments, both before and after tubing. But interestingly, if there was any air in the collection device when the device was sent through the tube system, the pO2 after tubing still matched on the two instruments, but the values were more than double the original values. If no air was present, there was very little change before and after tubing. We tested this by expressing all air from one set of samples before tubing and leaving air in the syringe on the other set.
The collection process for blood gas samples in our institution has always specified that the collector should express any air in the sample before sending the sample to the lab through the tube system, and after this incident the reason for that step became clear. However, the staff collecting blood gases on the floors needs to be periodically retrained in the collection, and the lab staff needs to be reminded that air in a blood gas syringe arriving through the tube station is a reason to reject the sample. We were reminded that education needs to be a continuous process. We also learned that when we discover the reason for a process, it’s a good idea to document that reason in order to both understand the need and to help motivate people to follow it.
-Patti Jones PhD, DABCC, FACB, is the Clinical Director of the Chemistry and Metabolic Disease Laboratories at Children’s Medical Center in Dallas, TX and a Professor of Pathology at University of Texas Southwestern Medical Center in Dallas.
The American Society of Cytopathology is conducting a reproducibility study, and they need your help. They’d like for participants to evaluate images from the new Paris System for Reporting Urinary Cytology Atlas. If you’re able to participate, follow this link.