One of my favorite parts of being a cytotechnologist is the delight of having cytology students rotate through our institution as a practicum site. The pandemic caused a clinical rotation hiatus for the safety of both our staff and students, but thanks to widespread healthcare vaccination, we were able to bring in some fresh minds to experience the variety of interesting cases we enjoy every day. I think what I love most about having students here is reminiscing of when I was in their shoes seven years ago. I remember going into my rotations using nothing but morphologic criteria I memorized from lecture and labs. My clinicals served as a rude awakening that we rarely see any textbook perfect cases. Cancer is like a shape-shifter – one melanoma looks entirely different than another. Two lung squamous cell carcinomas from the right upper lobes from two different patients could look entirely different. The unique variation within and between cancer types is what makes this field so beautifully fascinating. The first time a cytotechnology student shows me a case, tells me their thoughts, works through the criteria, and lists the differentials, I look up and say, “nothing is quite by the book.” How often we fall into a routine of relying on criteria, closing our minds to certain diagnoses because it doesn’t quite look like the clinical impression. When the pathologic and clinical impressions divide, more diagnostic tests are performed, CPT codes fill our billing tab, and we start to panic. “It’s supposed to be adenocarcinoma, so why doesn’t it look like adenocarcinoma?!?
A few weeks ago, the lab received a left pleural fluid from a patient who presented with a history of small cell cervical cancer. I remember learning about this in my first semester of grad school – how rare a finding of small cell carcinoma is, accounting for less than 5% of cervical cancers. It essentially mimics small cell carcinoma of the lung and other neuroendocrine carcinomas, where you should be able to identify the telltale salt-and-pepper chromatin, nuclear molding, scant cytoplasm, loosely cohesive or isolated, necrosis, usually an absence of nucleoli, a high proliferation index with mitotic figures, etc. It’s an aggressive disease to say the least, just like its lung counterpart. When this cancer metastasizes, it takes its same characteristics with it, spreading rapidly without care.
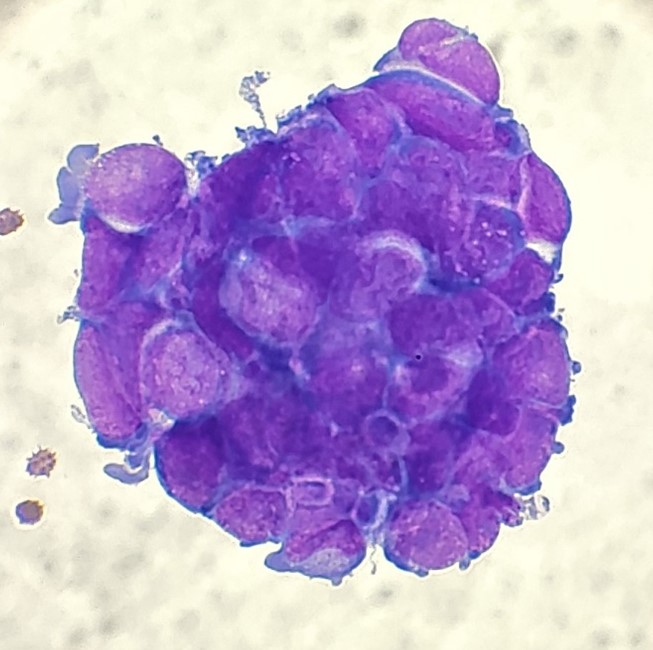
The first step in processing a fluid is to prepare a fresh, air-dried, Diff-Quik-stained cytospin to triage the specimen and decide whether the specimen should be processed routinely or hand-prepped and stained with overtly positive fluids to prevent cross-contamination. There was one cluster identified on the Diff-Quik preparation, but compared to the background of mesothelial and inflammatory cells, the tumor content was insufficient to push it up to hand-processing. The bluish cytoplasm caught my attention as a feature of neuroendocrine tumors AND lymphomas, but the nuclear molding had me favoring neuroendocrine.
That afternoon, I examined the pap-stained smears and SurePath liquid-based preparation, identifying similar cells of interest. However, despite the presence of nuclear molding and scant cytoplasm, the nuclei presented with prominent nucleoli. An interesting feature, to say the least.
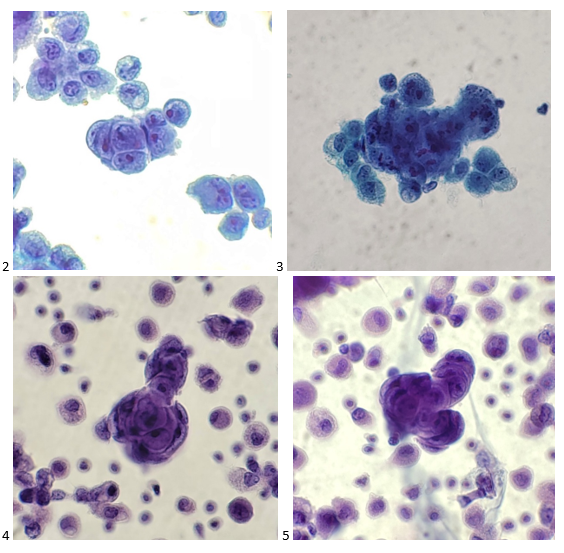
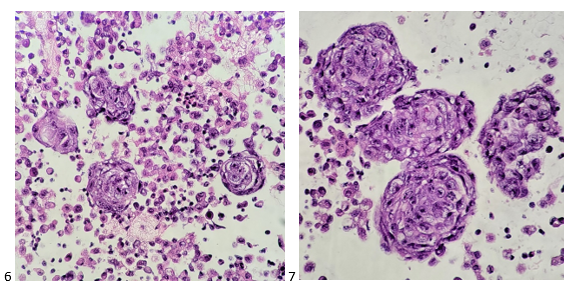
The following morning, I screened the cell block slides and came across molded groups of cells (appearing as a garden aerial view). Still the prominent nucleoli baffled me, and I thought, “Why doesn’t this look like a classic small cell carcinoma? They clinical history even included known lung mets from the patient’s small cell cervical cancer!”
When I sent the case for review by the pathologist, I wrote up a diagnosis of Positive for Malignant Cells; Carcinoma, small cell? Recommend correlation with IHC.” My attending was just as intrigued. She ordered a thorough panel of immunohistochemistry stains based on the morphologic findings.

The tumor cells are positive for synaptophysin, CD56, TTF-1, and BerEP4, focally positive for CK7 and chromogranin (not shown), and negative for calretinin, PAX-8, and p40 (also not shown). The findings support the diagnosis of metastatic high grade carcinoma with neuroendocrine differentiation.
While the stains support a diagnosis of small cell carcinoma, the morphologic diagnosis was mildly questionable. I went back to the patient’s record to see what we may have missed in the clinical history. It turns out the patient initially presented with Stage IB2 HPV+, moderately-differentiated cervical adenocarcinoma in 2020. After completing brachytherapy and one cycle of chemotherapy, but could not tolerate additional treatments due to leukopenia and elevated LFTs. Shortly thereafter the patient complained of abdominal pain and a liver mass and bulky lymphadenopathy were identified on imaging. An FNA of a supraclavicular lymph node confirmed not only metastasis of the patient’s cervical cancer, but discovered a small cell/neuroendocrine transformation. And this is why proper documentation of clinical history is so important to pathologists and laboratory professionals. In one of my earlier posts, I preached that cancer doesn’t discriminate; so why should we? Keeping an open mind is paramount to both succeeding in and enjoying the field of cytopathology. If it looks like a duck, and it walks like a duck, it might actually have transformed into a goose.

-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.