Working in a cancer center, our cytologists are well-versed in cancer morphology being able to diagnosis primary malignancies, distant metastases, and even combined metastatic disease in the same lymph node. What we don’t see as often as community hospitals are infectious diseases. However, we do have many immunocompromised patients at our institution, so the rare opportunistic infection does occur. And boy, do we get excited to pass the case around! Please find a series of infectious events embedded within this post. And unfortunately, we do not live in an area where coccidiomycosis is endemic, so beyond school, we haven’t had the pleasure of identifying those in our daily work.
Case 1. Lung, Bilateral, BAL (Bronchoalveolar Lavage)
A 73-year-old male patient was admitted to the ICU with pneumonia. The pulmonologist performed a bilateral bronchoalveolar lavage (BAL) to rule out pneumocystis pneumonia. We prepared a pap-stained smear, two cytospins, a SurePath liquid based prep, and a cell block. Two additional cytospins were sent to histology for GMS staining. While no malignant cells were identified, fragments of squamous epithelium with acute inflammation and necrosis were present. Multiple viral inclusions were identified, appearing as ground glass within the nuclei. (Image 1). These cells present with classic 3 M features: molding, multinucleation, & margination of chromatin. The cell block also highlights viral inclusions, but demonstrates pseudohyphae and spores associated with surrounding squamous cells as well (Image 2).
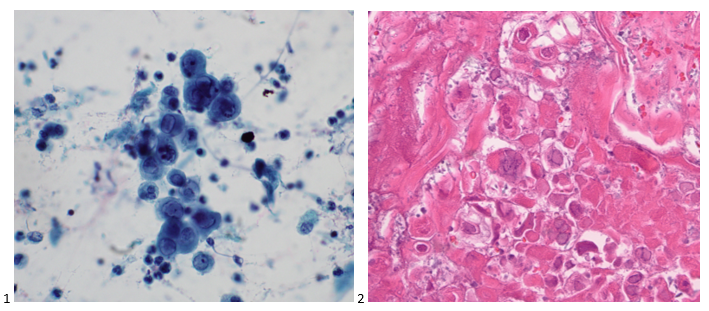
Diagnosis: Herpes Simplex Virus (HSV) and Candida.
Case 2. Lung, Left Lower Lobe, CT-guided FNA
A 72-year old male with stage IIA squamous cell carcinoma underwent a VATS right upper lobectomy and mediastinal lymph node dissection. He completed adjuvant carboplatin/gemcitabine therapy. On a surveillance CT scan, the treated area demonstrated progression as well as multiple bilateral lung nodules. To determine whether the new left lower lobe superior segment lung nodule was a metastasis or new primary, a CT-guided biopsy was performed. The smears and cell block sections were negative for malignancy but demonstrated inflammatory cells and necrotic debris, consistent with a necrotizing inflammatory process (Images 3-5). A separate pass was sent for microbiological cultures to correlate our findings. The following day, Kinyoun and GMS stains were performed on paraffin-embedded sections of the cell block. No fungal organisms were identified on GMS, but acid-fast bacilli were noted by the cytologist on the Kinyoun-stained section (Image 6).

Diagnosis: Acid-fast bacilli (AFB), consistent with Mycobacterium Avium Complex. Isolated and confirmed by microbiology.
Case 3. Lung, Right Upper Lobe, CT-guided FNA
A 58-year-old male presented with multiple lung nodules and a brain mass. We reviewed the brain mass excision from an outside institution and agreed with the original diagnosis of anaplastic oligodendroglioma, WHO grade III with a Ki-67 proliferation index that approached 20%. EGFR was not amplified (ratio 1.2), but 1p/q19 co-deletions were noted in greater than 75% of tumor cells. To rule out primary versus metastatic disease, the patient had a CT scan-guided biopsy of right upper lobe lung mass. No malignant cells were identified in the sample; however, necrotic debris and abundant fungal hyphae were noted (Images 7-9). A portion of the sample was sent to Microbiology for culture. The following day, a GMS and PAS stains were performed on paraffin-embedded sections of the cell block which demonstrated the same fungal hyphae seen in the smears and cell block preparations (Images 10 & 11).
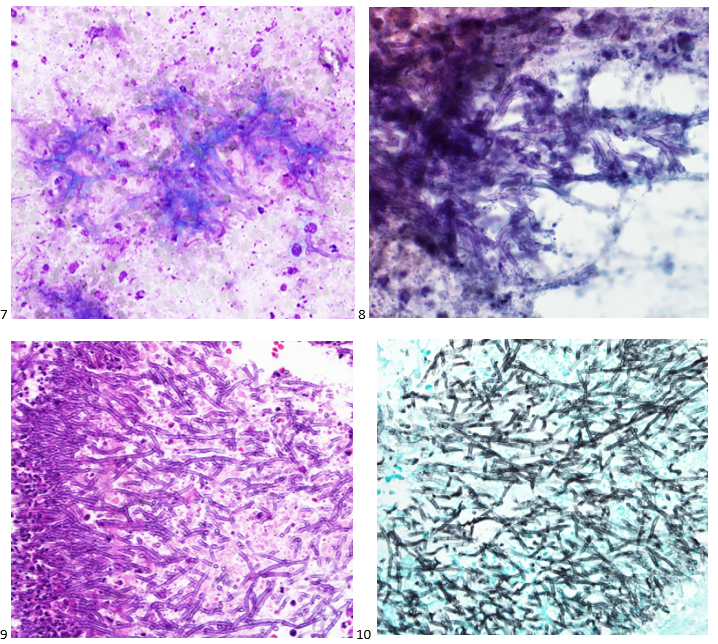
Diagnosis: Abundant fungal hyphae, consistent with Aspergillus
Case 4. Left Hilum, EBUS-FNA
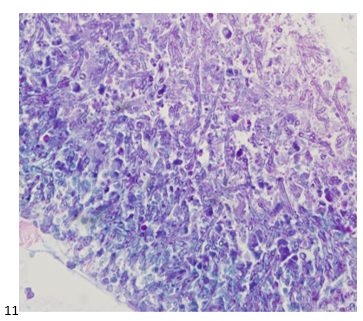
A 20-year-old female patient presented with patches, pain, and inflammation on her legs, and she was diagnosed with erythema nodosum. When her swelling and pain worsened, a chest X-ray demonstrated a left hilar mass, and a subsequent CT demonstrated the mass to be encircling the left superior pulmonary artery and obstructing the pulmonary vein along with multiple peribronchial ground-glass opacities and hilar lymphadenopathy. The concern from the referring physician was thymoma versus lymphoma given her age and clinical presentation. The patient underwent an endobronchial ultrasound to assess the hilar mass and lymphadenopathy. The lymph node aspirates appeared benign, with flow cytometry supporting the cytologic diagnosis. On the left hilum FNA, there were aggregates of lymphocytes, plasma cells, and epithelioid histiocytes with caseating necrosis and fibrosis (Image 12-14). Kinyoun, PAS, and GMS stains were performed on paraffin-embedded sections of the cell block. No acid-fast bacilli were identified. Fungal organisms in the form of budding yeast were noted on GMS (Image 15) and PAS stain. The patient was prescribed a 12-week course of antifungal medication.
Diagnosis: Necrotizing inflammation with fungal organisms, suggestive of Histoplasmosis.
Case 5. Lung, Right Middle Lobe, BAL (Bronchoalveolar Lavage)
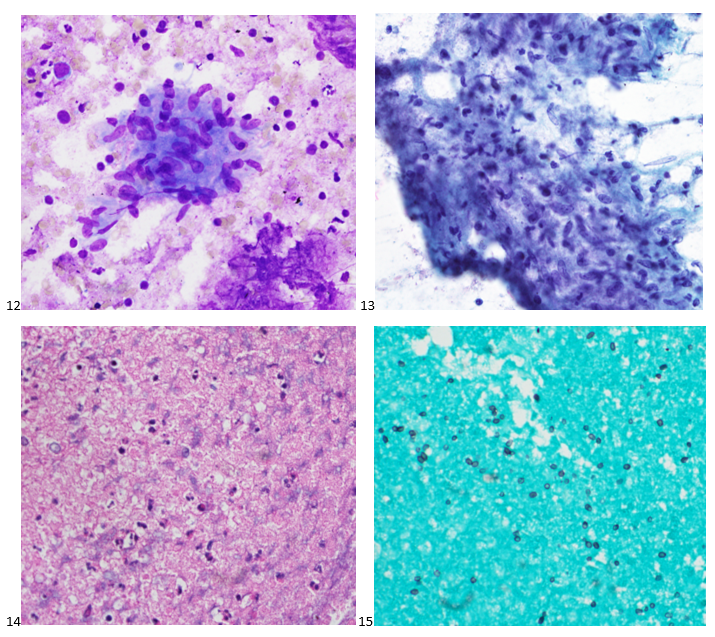
A 44-year-old male patient with uncontrolled Type II diabetes and hypertension presented to pulmonary after imaging demonstrated diffuse mediastinal and hilar lymphadenopathy. The differential diagnosis was sarcoidosis versus a lymphoproliferative process. An endobronchial ultrasound was performed to evaluate the lymph nodes, all of which came back as reactive. A BAL was performed and sent for cell count, cytology, flow cytometry, and microbiology. Flow cytometry analysis demonstrated a reversed CD4:CD8 ratio, and upon further testing, the patient was determined to have HIV. Eosinophilic froth or casts were identified on the cytopreparations of the BAL (Images 16). GMS and PAS stains were performed with adequate controls, and the PAS was negative for other fungal organisms while the GMS demonstrate positive staining for what we in cytology refer to as cups or crushed ping pong balls (Image 17). He was treated with Bactrim.
Diagnosis: No malignant cells identified. Positive for Pneumocystis jirovecii.
Case 6. Lung, Right Lower Lobe, CT-guided FNA
A 68-year-old male patient with a history of a renal transplant presented with an endobronchial mass in the left lower lobe that was biopsied and diagnosed as adenocarcinoma at an outside institution. We reviewed the slides in-house and determined the original tumor to be a mucoepidermoid carcinoma. After an unsuccessful staging procedure, a mediastinoscopy was performed, and the mediastinal lymph nodes showed hyalinizing non-necrotizing granulomata, suggesting underlying sarcoidosis. No microorganisms were identified with AFB, GMS, or PAS stains. The patient did not receive adjuvant therapy following the resection of his endobronchial tumor. Seven years later, he presented to the ER for syncope and 30 lbs. weight loss in 5 months. A CT scan was performed demonstrating a thick-walled cavitary lung mass in the right lower lobe. The patient was referred to radiology for a CT-guided FNA of the RLL mass. Fibrous tissue and abundant microorganisms with a polysaccharide capsule were identified on both FNA and core biopsy (Images 18-20). The PAS, GMS, Mucicarmine (Image 21), and Fontana Masson special stains were performed on cell block sections, with proper controls, highlighting abundant microorganisms. The patient was prescribed an antifungal for his cryptococcoma (cryptococcal lung abscess).

Diagnosis: No malignant cells identified. Abundant microorganisms, morphologically consistent with Cryptococcus species.
If you enjoyed this special series, look out for more in the future! And feel free to recommend or request interesting cases!

-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.