A 39 year old male presented to a hospital in Dallas, TX with left upper quadrant abdominal pain, nausea, decreased appetite, and a feeling of bloating. The abdominal pain was described as a gradual onset of pain over the course of 2 to 3 weeks. He had no known weight loss, night sweats, chills, diarrhea, or recent trauma. The patient was afebrile on exam with unremarkable vital signs and reported tenderness in the left upper quadrant on palpation of the abdomen. Of note, he was admitted to the hospital 6 weeks prior with abdominal discomfort and was found to have a splenic abscess on computed tomography (CT) scan of the abdomen. There was no surgical drainage of the abscess at that time, and he was treated with two weeks of antibiotics with initial improvement in symptoms. The patient had a past medical history of 3 previous episodes of acute sigmoid diverticulitis that were each treated with bowel rest and 14 days of empiric antibiotics. After the second episode of diverticulitis, the patient had a colonoscopy with findings of colitis and 2 polyps were removed that were negative for malignancy. Following the third episode of diverticulitis, the patient had a sigmoid and partial descending colectomy about 2 years prior to the current presentation.
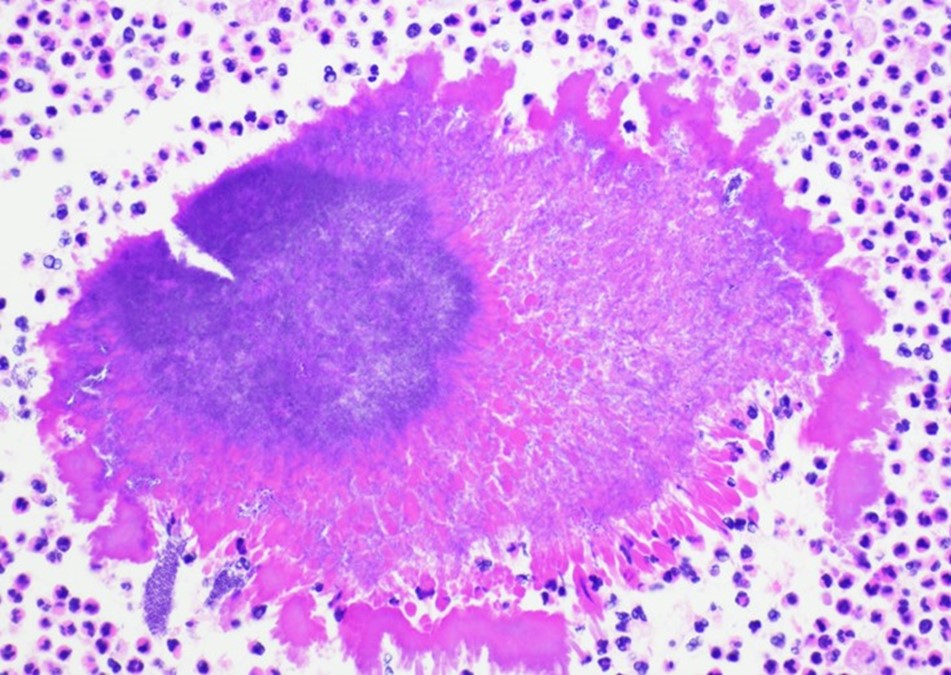
On admission, a CT scan of the abdomen and pelvis revealed a 3.5 x 1.9 cm air and fluid collection of the inferior border of the spleen and 5.2 x 1.6 cm fluid collection of lateral spleen. The collections were noted to be increased compared to the prior imaging 6 weeks before. Blood cultures were without growth at 5 days. A transthoracic echocardiogram showed no significant valvular abnormalities or vegetations. On hospital day 5, the patient was taken to the operating room for a laparoscopic splenectomy and left diaphragm repair. Surgical findings included a large spleen with omental adhesions and a thick rind along the spleen, which was closely adherent to the diaphragm. A portion of the colon closely adherent to the spleen was also noted. Histopathologic examination showed multifocal splenic abscesses with surrounding fibrosis on hematoxylin and eosin (H&E) stain and granules with surrounding Splendore-Hoeppli material on higher magnification (Figure 1). On Grocott-Gomori methenamine silver (GMS) stain, the granule was seen to be composed of mixed bacterial morphologies with a predominance of filamentous rods typical of Actinomyces (Figure 2). Based on histopathological examination, a diagnosis of splenic actinomycosis was rendered.

Discussion
Actinomycosis is a slowly progressive infection characterized by fibrotic mass-like lesions, abscesses, granules, progression across tissue planes, and the development of sinus tracts. The incidence of actinomycosis has declined in the U.S., which is thought to be due to better oral hygiene and the organism’s susceptibility to a wide range of antibiotics.4 The clinical manifestation of actinomycosis is classified by the anatomical site of infection. This includes oral-cervicofacial, thoracic, abdominopelvic, central nervous system, musculoskeletal, and disseminated forms of disease. Oral-cervicofacial disease is the most common form and classically develops with fevers and perimandibular soft tissue swelling that may have a firm or “woody” consistency on palpation.4 Abdominopelvic disease occurs in about 20% of cases with intra-abdominal manifestations usually due to appendicitis, inciting trauma, or previous surgical procedure and pelvic disease most often due to intra-uterine contraceptive devices.1 The clinical manifestations of actinomycosis are often difficult to correctly diagnose, and the presentation and imaging findings often mimic malignancy further complicating the assessment. Diagnosis relies on consideration of the disease process and diagnostic sampling for histopathology and microbiologic studies.
Although most actinomycotic lesions are polymicrobial, species of the genus Actinomyces are the predominant etiologic agents.2 Actinomyces are a group of gram positive filamentous facultatively anaerobic or microaerophilic bacteria that are normal flora of the gastrointestinal and genitourinary tracts. The organisms typically have true branching and may appear beaded due to irregular Gram staining. Importantly, Actinomyces spp. will be negative with modified acid-fast staining, which can be used to differentiate it from Nocardia spp. The bacteria are relatively slow growing on primary culture and mature colonies may have a variety of morphologies. The classic “molar tooth” appearance is characteristic of A. israelii.3 On histopathology, actinomycotic lesions have a surrounding area of fibrosis and central suppurative inflammation with granules. The granules consist of accumulations of organisms with club-shaped ends and filamentous rods seen on special staining.4 Optimal diagnosis would consist of visualization of these features on histopathology or other direct method. Isolation of the organism can be useful but should be taken in the context of the clinical picture as the mere isolation of Actinomyces in culture does not always imply actinomycosis.
Splenic involvement of actinomycosis is an uncommon cause of the intra-abdominal disease process. In our case, the most likely etiology for splenic actinomycosis was due to the recurrent episodes of acute sigmoid diverticulitis with breaches in the mucosal barrier and direct invasion into the spleen. The surgical management in this case was splenectomy to avoid splenic rupture. Medical management involves antibiotic therapy with high-dose penicillin as first-line therapy. The treatment duration has historically been to treat with parenteral penicillin for 2 to 6 weeks and then transition to oral penicillin or amoxicillin up to a year based on clinical response.
References
- Bennhoff D: Actinomycosis: diagnostic and therapeutic considerations and a review of 32 cases. Laryngoscope 1984; 94: pp. 1198-1217.
- Blaser MJ, Dolin R, Bennett JE. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Ninth edition. Elsevier; 2020.
- Pfaller, M. A., Carroll, K. C., & Jorgensen, J. H. (2015). Manual of clinical microbiology (11th edition.). ASM Press.
-Zane Conrad, MD is a medical microbiology fellow at UT Southwestern Medical Center.
-Dominick Cavuoti, DO is a professor at UT Southwestern and practices Infectious disease pathology, medical microbiology and cytology.

-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.

-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.

Interesting case but it would have been great to culture some of the biopsy. The reason being, I would have liked to see if the mixture more resembled oral flora than bowel flora. A possible hypothesis is that damage was initially by bowel incursion but the resulting damaged tissue then become colonised by oral flora after transient bouts of bacteraemia. In other types of abscesses such as the brain, the most likely source is mouth following bouts of bacteraemia.